A number of studies of schizotypy in college populations have used scores on the Chapman Perceptual Aberration Scale (PAS)
1 as their criterion measure for schizotypy (for review, see Lenzenweger
2). Individuals have been screened with this scale, and those scoring high on the PAS are designated as “high schizotypy” and compared with those scoring near or below the mean on PAS. The PAS has been used in this way because it has shown a fairly high correlation with broader measures of schizotypy.
The equating of perceptual aberration with schizotypy is a questionable practice because 1) perceptual aberration is only one of several facets of schizotypy and 2) perceptual aberration may occur in some people for reasons unrelated to schizotypy (e.g., a primary perceptual deficit). Scores on the PAS correlate with overall schizotypy scores; however, this does not mean that PAS scores accurately represent levels of schizotypy. Furthermore, the cognitive, psychophysiological, and other correlates of perceptual aberration may not be the same as the correlates of schizotypy.
The present study assessed participants on two important facets of schizotypy: perceptual aberration and magical ideation. Sustained attention, which has been demonstrated to be impaired in subjects with high PAS scores,
3 was then tested by means of a visual continuous performance test administered to each participant. Results were examined by analysis of variance to compare attentional performance in those high versus low on each measure of schizotypy. We were interested in testing whether findings of relatively poor performance on a cognitive measure in high-PAS participants would still hold when an additional facet of schizotypy was introduced into the analysis.
4,5METHODS
A group of 345 undergraduates completed scales assessing levels of perceptual aberration (Perceptual Aberration Scale
1) and magical ideation (Magical Ideation Scale; MIS
6) as part of a mass testing protocol. Students were then selected for further participation in the study on the basis of their PAS scores. The “high PAS” group included 24 individuals who scored more than one standard deviation above the mean on the PAS (PAS>10). The “low PAS” group included 27 participants who scored low on the scale (PAS=1 or 2). Written informed consent was obtained from all participants.
Each of the 51 participants completed the Degraded Stimulus Continuous Performance Test (DSCPT).
7 The DSCPT is a computerized test of attention with a high information-processing load. It involves the visual presentation of a series of degraded (i.e., highly blurred) digits at the rate of one per second. Subjects are instructed to push a button every time the target digit appears. Hit rate over 480 trials was used as the measure of attention.
For the analysis, participants were divided into high and low PAS groups. They were also divided into three equal groups based on their MIS scores (high, mid-range, and low). A two-way analysis of variance (ANOVA; PAS×MIS) was calculated for the hit rate measure of DSCPT performance.
RESULTS
Perceptual aberration scores were highly correlated with MIS scores (
r=0.74, df=50,
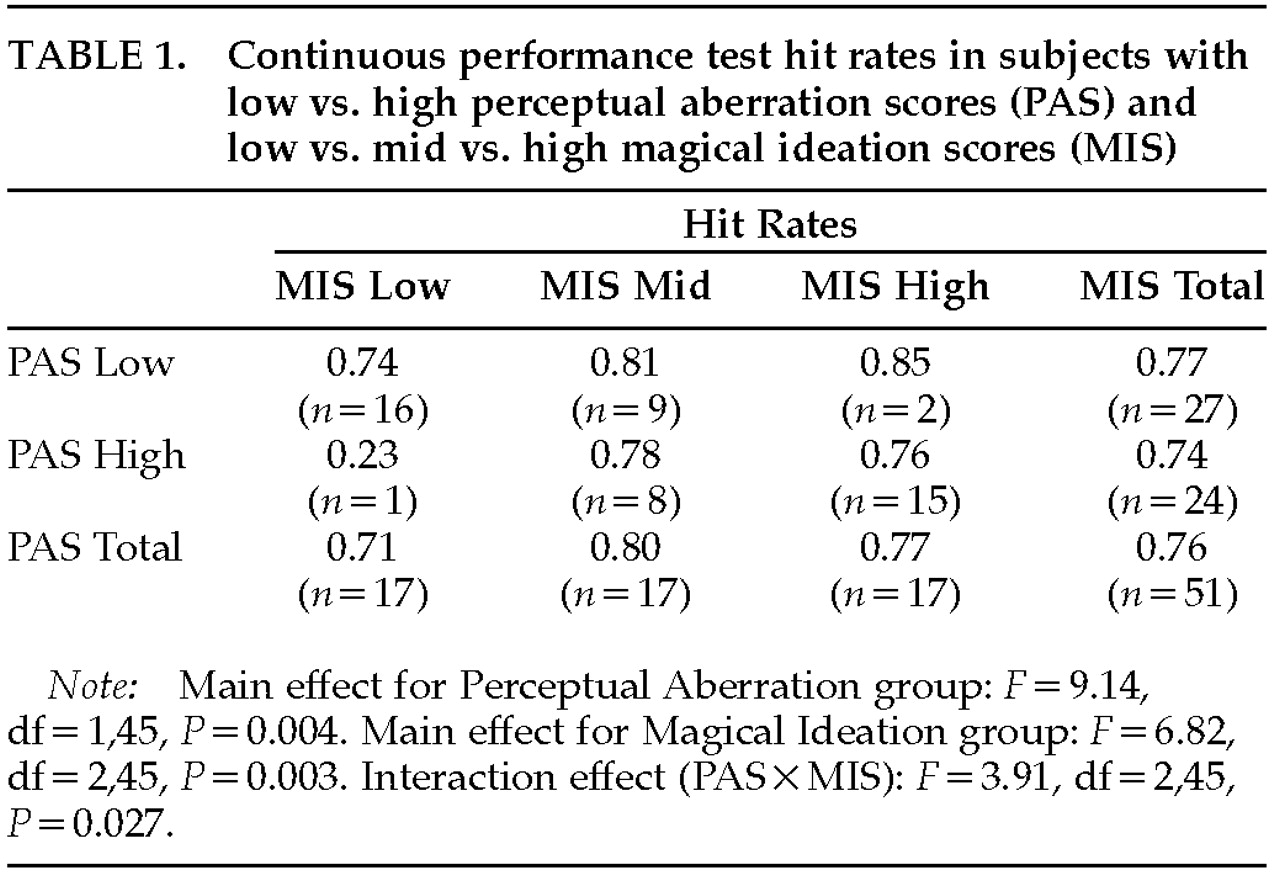
P<0.001), indicating that participants who scored high on the PAS also tended to score high on the MIS. Therefore only a few individuals were in the “low PAS/high MIS” and the “high PAS/low MIS” groups (
Table 1).
In a two-way ANOVA (PAS×MIS) with attentional scores as the dependent variable, there was a significant main effect for PAS (F=9.14, df=1, 45, P=0.004), indicating that high-PAS participants showed significantly lower hit rates on the DSCPT than low PAS participants. This is consistent with previous findings on cognitive test performance. However, there was also a main effect for MIS, indicating that mid-range and high MIS scores predicted a better DSCPT hit rate than low MIS scores, and there was a significant interaction effect between PAS and MIS scores (F=3.91, df=2,45, P=0.027).
Low PAS/high MIS participants performed best, and high PAS/low MIS participants performed worst. Although few individuals were in these two categories, when they were excluded from analysis of the total participant group, the PAS main effect disappeared. See
Table 1 for these results.
DISCUSSION
The results of this small study appear to support the hypothesis that high PAS scores, when used alone, are not an optimal criterion for measuring the larger construct of schizotypy. High-schizotypy participants showed poorer performance on the DSCPT than low-schizotypy participants when the only criterion for schizotypy was PAS score; however, this association did not hold when another criterion of schizotypy, MIS, was added. This result suggests that even though PAS scores are correlated fairly highly with measures of other facets of schizotypy, high PAS scores also may reflect something unrelated to schizotypy in some individuals. This other factor, rather than schizotypy, may be responsible for the poor attentional performance by high PAS groups.
The sample for this study was small. Subjects with high PAS and low MIS scores (or vice versa) were few. Past research has attested to the multidimensionality of schizotypy. We do not believe that our findings threaten the validity of the multidimensional schizotypy construct in any way. Our findings are merely cautionary. They suggest that use of multiple measures in selection of schizotypic subjects may be preferable to the use of a single criterion such as perceptual aberration.