As states attempt to reduce the census in their chronic psychiatric facilities, increasing numbers of institutionalized geriatric schizophrenic inpatients are being discharged to nursing home and other geriatric care settings. Therefore, it is important to understand the factors that prevent discharge in some patients, as well as common problems facing elderly formerly institutionalized patients as they make the transition to residence in alternative settings. One of the factors that may affect patients' discharge status to a less restrictive environment may be the frequency and severity with which they display overt aggressive behavior.
1Aggression plays a substantial role in the course and outcome of schizophrenia. In addition to its causative role in psychiatric hospitalization,
2 physically aggressive behavior is likely to prevent hospitalized patients from being discharged
3–5 and increases the probability that they will be rehospitalized after discharge.
5 White et al.
1 found that elderly inpatients who were retained in an institutional setting had more severe symptoms of excitement, hostility, and impulsive behavior than patients who were discharged. Thus, aggressiveness plays a crucial role in determining schizophrenic patients' ability to reside outside the institutional setting and their potential to be discharged in later life. Therefore, it is important to understand factors associated with aggression in older patients with schizophrenia.
Previous studies have generated widely disparate estimates of the frequency of aggression in inpatients with psychotic disorders. McNiel and Binder
6 found that 23% of a sample of psychiatric inpatients (33% of schizophrenic patients) displayed physical aggression during an acute hospitalization period that averaged 18 days. Cheung et al.
7 found 63% of inpatients in rehabilitation wards displayed some form of aggressive behavior over an 8-week period. Sample and methodological differences may account for the wide variability. The frequency of verbal aggression may be as high as three times that of physical aggression,
8 and physical attacks that cause serious injury are rare in inpatient settings.
7–9 Citrome and Volavka
10 provide a synopsis of epidemiologic studies of violent behavior in schizophrenia, addressing these issues in detail.
One symptom of schizophrenia that may be a factor in aggressive behavior is cognitive dysfunction; in particular, cognitive decline in later life. Because cognitive impairment in late-life schizophrenia is known to be severe in many state hospital and nursing home patients,
11 it is important to understand if this impairment is associated with aggressive behavior. Given the absence of research on aggression in late-life schizophrenia, we must rely on the literature regarding the link between cognitive decline and aggression in dementing disorders. Several studies have shown that cognitive deficits predict the occurrence of aggression in patients with various dementing conditions.
12–15 Aggression in geriatric care settings, such as nursing homes, is an important issue in patient care because it occurs in a large proportion of these patients
16,17 and tends to be directed at nursing staff as they provide assistance with activities of daily living.
18 There appears to be a relationship between cognitive functioning and the type of aggression in elderly demented patients. Specifically, verbal aggression is generally associated with delusions, affective disorders, and preserved cognitive functions, while there appears to be a positive relationship between physical aggression and a decline in cognitive functioning.
13,14,19 Thus, cognitive functioning and psychotic symptomatology appear to be factors associated with aggression in demented patients. However, this relationship is not linear. In many severely impaired patients, the presence and seriousness of aggressive acts decreases.
20Although the link between cognitive impairments and aggression in patients with schizophrenia has not been studied to the same extent as in dementia, some correlations have been identified. Adams et al.
21 concluded that global impairment on a neuropsychological test battery was related to adult history of violence in the community, but not inpatient violence, among a group of 37 male schizophrenic patients. Krakowski et al.
22 found more neurological abnormalities (e.g., in right-left orientation, tandem walk, stereognosis, graphesthesia) and visuospatial abnormalities in schizophrenic patients with a high rate of violence than in those with a low rate of violence. Similarly, Krakowski and Czobor
23 showed an association between persistent violence and frontal lobe impairment, as measured on a quantified neurological scale, in schizophrenic inpatients. In a study of forensic patients, most of whom were patients with schizophrenia, Foster et al.
24 found that frequency, but not severity, of aggression could be predicted from performance on the Judgment of Line Orientation, Stroop Color Word Test, and Emotion Perception Test. However, the Wisconsin Card Sorting Test, Test of Nonverbal Intelligence, and Symbol Digit Modalities Test did not account for a substantial portion of the variance. In addition to correlations with neuropsychological test performance, aggression in schizophrenia has been associated with dysfunction in the amygdala
25 and parieto-occipital atrophy on CT scan.
26Other characteristics of schizophrenia that are likely to influence aggressiveness are positive and negative symptoms. Studies have produced discrepant findings in examining the symptom correlates of aggression in schizophrenia. Although some studies point to a relationship between positive symptomatology and aggression,
27,28 others have found an association with affective symptoms, but not with positive symptoms.
29,30 In partial reconciliation of these discrepant findings, a detailed analysis by Cheung et al.
31 of the relationship between aggression and hallucinations and delusions detected intervening variables. Specifically, the likelihood that a patient would be aggressive was a function of the tone and content of the hallucinations and delusions, the patient's emotional reaction to these symptoms, and his or her ability to cope with these symptoms. Thus, the role of schizophrenic symptomatology in aggressive behavior is complex and may be contingent on the content of the symptoms and the individual's characteristics.
Factors extrinsic to the schizophrenic patient may also contribute to aggressiveness. Such conditions may include overcrowding,
32 limit-setting and communication problems involving staff,
8 and dissatisfaction with ward environment.
33 The environment of a nursing home compared with an inpatient ward may influence patients' propensity to behave aggressively, and as such should be explored as a correlate of aggression.
A number of psychotropic medications have been shown to reduce aggressiveness in schizophrenic patients and should be considered in examinations of the correlates of aggressive behavior. Clozapine has shown specific antiaggressive effects in the treatment of schizophrenia.
34 Risperidone has shown a greater effect on reducing hostility,
35 and comparable results in reducing levels of aggression,
36,37 when compared with conventional antipsychotic medication. Additionally, risperidone reduces behavioral disturbances and aggression in dementia.
38,39 Because treatment of aggression is not limited to antipsychotic medications
40 and is likely to effect the frequency, intensity, and duration of aggression, it is important to consider the differential effects of medication status when examining correlates of aggression. The previous studies of aggression in schizophrenia have studied younger patients, and violence associated with dementia occurs most often in older patients; it is therefore important to understand the frequency, characteristics, and correlates of aggression in chronic geriatric schizophrenic inpatients residing in both chronic psychiatric hospitals and nursing home settings.
In the present study, we examined aggressive behavior and its correlates in institutionalized geriatric schizophrenic patients who resided either in nursing homes or chronic psychiatric hospitals. The frequency and type of aggression (verbal or physical) were examined in psychiatric inpatients compared with patients who were discharged to a nursing home setting. In both groups of patients, we examined correlations between aggressive behavior and cognitive functioning, psychopathology (positive, negative, and general symptoms), and social and adaptive functioning.
METHODS
Participants
All patients included in this study were participants in a large-scale program of research on cognitive functioning and clinical symptoms in geriatric chronic psychiatric inpatients. In this study, the entire population of a state psychiatric center was rediagnosed and reevaluated with a comprehensive assessment of clinical, cognitive, and functional status. All patients assented to participation; the Internal Review Boards at Pilgrim Psychiatric Center and Mount Sinai School of Medicine approved a waiver of a signed informed consent. Research staff members performed diagnostic assessments and used a structured consensus procedure in making DSM-III-R diagnoses of schizophrenia. The entire assessment procedure for that study has been published, and all subjects in this study were diagnosed and assessed with that procedure.
41,42Potential participants were excluded from this study if they were in active treatment for a seizure disorder or if they had a previous cerebral vascular accident, a prior diagnosis of alcohol/drug dependence, head trauma with loss of consciousness in the past, or concurrent pervasive developmental disorder, mental retardation, neurological diseases or damage, or other psychiatric diagnoses. Patients were also excluded if their current overall Clinical Dementia Rating (CDR)
43 was greater than 3 (indicating they could no longer use or understand language adequately or recognize even close family members, or required total care because they were bedridden, completely uncommunicative, and incontinent). All patients received an annual physical and neurological examination. In order to exclude patients with newly incident dementing conditions, any patient whom a neurologist determined, on the basis of a scheduled annual clinical evaluation, had experienced “rapid cognitive decline” in the past year was also excluded.
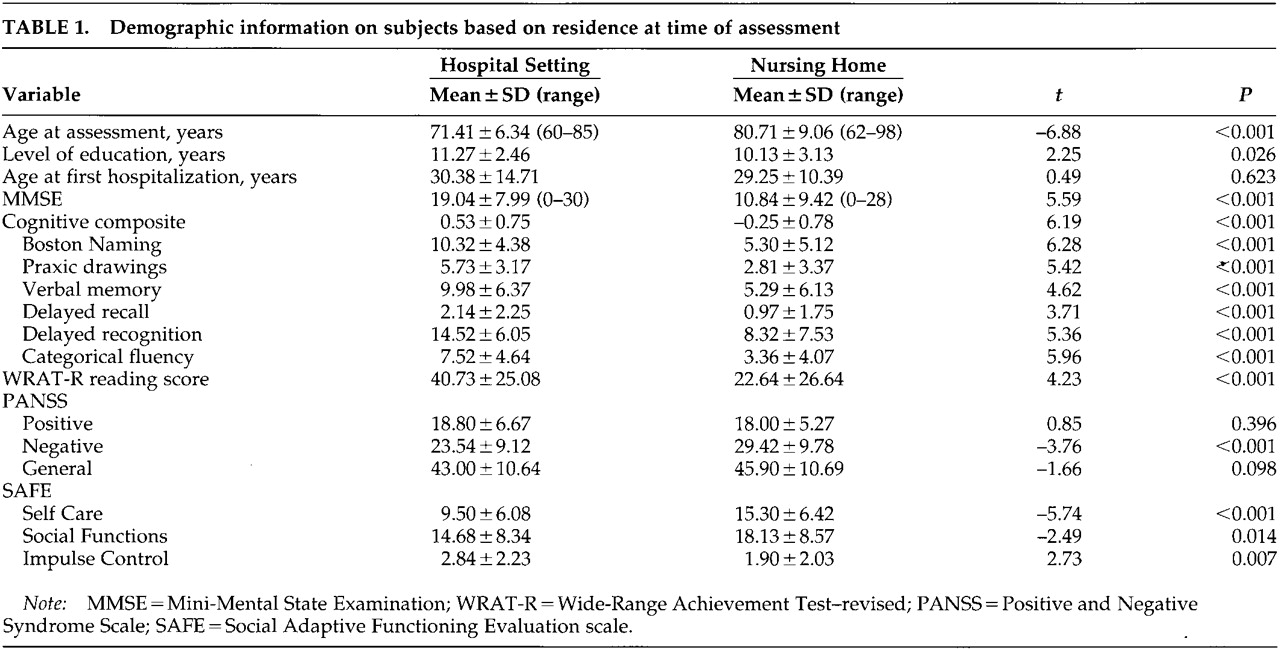
A total of 170 patients (88 female, 82 male) met inclusion criteria for this study. The mean age of the patients was 77.56±9.35 years, mean age at first hospitalization 29.61±11.89 years, and mean number of years of education was 10.50±3.00 (means±SD). At the time of assessment, participants were either long-stay patients at a state institution, patients at a Veterans Administration Hospital, or residents in a nursing home (
Table 1).
Assessments
Negative and Positive Symptoms:
Severity of schizophrenic symptoms was assessed by using the Positive and Negative Syndrome Scale (PANSS).
44 This is a 30-item scale with 7 items measuring positive symptoms, 7 items measuring negative symptoms, and 16 items measuring general aspects of psychopathology. The total scores on positive and negative subscales were used as the dependent measures. Interrater reliability of these ratings in our patients was previously found
41 to be acceptably high, with intraclass correlations (ICC;
n=30) ranging from a low of 0.86 to a high of 1.00 (all
P<0.001).
Global Cognitive Assessments:
In this study, both global and specific measures of cognitive functioning were used. The Mini-Mental State Examination (MMSE) was used as a global measure of cognitive functioning. MMSE scores range from 0 to 30 and comprise the results of an assessment of registration, memory, orientation, praxis, and verbal skills such as naming.
CERAD Cognitive Battery:
This brief neuropsychological assessment battery was developed for the diagnosis and staging of Alzheimer's disease.
45 As a result, it measures several crucial cognitive impairments that are present in dementia. Previous research with this battery has demonstrated that Alzheimer's disease patients can be discriminated from patients with schizophrenia on a cross-sectional basis.
42 Additional studies with the CERAD battery demonstrated that schizophrenic patients have high test–retest stability coefficients and do not decline as a group at a 1-year follow-up on any of the measures in the battery.
46 In previous analyses of this battery,
47,48 a composite measure of cognitive functioning was created by standardizing all of the scores within the sample of schizophrenic patients and averaging them together into a single score. Measures included in the battery are described below.
Word List Learning and Delayed Recall—A 10-item list of words was presented to the subject on three separate learning trials. After each trial, free recall of the list was required of the subjects. After a delay, filled by the Praxis Drawings described below, a delayed recall of the word list was required, as well as a recognition task. The dependent variables were the total number of words correctly recalled over the three learning trials and the number of words recalled at the delayed recall.
Praxic Drawings—Four drawings (Circle, Diamond, Overlapping Rectangles, Cube) were presented to the subject, who was instructed to copy them exactly. Reproductions were scored according to predetermined criteria, and the dependent measure was the total score for the 4 drawings.
Modified Boston Naming Test—Subjects were presented with 15 line drawings and asked to name the object depicted. The drawings consisted of 5 objects with high frequency of occurrence in spoken English, 5 of moderate frequency, and 5 of low frequency. The dependent variable was the total number of correct namings.
Category Fluency—Subjects were instructed to name as many different animals as possible in one minute. The dependent variable was the number of unique animals named.
The scores on these five measures (Word List Learning, Delayed Recall, Praxic Drawings, Modified Boston Naming Test, and Category Fluency) were then integrated into a single composite score. This was done by transforming each raw score into a z-score, in order for each to be equally weighted, and using the mean of the z-scores for each measure as the individual's cognitive composite score.
An additional assessment was performed in order to obtain an estimate of premorbid intellectual functioning. The Wide-Range Achievement Test–Revised (WRAT-R
49) word recognition reading subtest was administered as a measure of putative premorbid academic competence. The dependent measure was the total score.
Social Adaptive Functioning Evaluation (SAFE):
This 17-item scale, developed by the current investigators,
50 and measures social-interpersonal, instrumental, and impulse-control deficits. This scale was designed to be rated on geriatric patients living in an inpatient facility after observation of and interaction with the subject, a caregiver interview, and chart review. Previous research with this scale found that both social and instrumental skills deficits were related to cognitive impairments, while deficits on the impulse control subscale were not.
51 This scale has suitable reliability, with interrater reliabilities of the items all exceeding 0.88 (ICC,
n=60). The total score is used as the primary dependent measure. Measures of self-care ability, social functioning, and impulse control were also derived through previously validated subscales of the measure.
Overt Aggression Scale (OAS):
This 16-item scale was designed to use family or staff observations to document and quantify overtly aggressive behaviors.
52 In the present study, overtly aggressive behaviors exhibited over both the 24 hours and the 7 days prior to assessment were quantified by interviewing caretakers and reviewing patient charts. The scale is divided into four types of aggressive behaviors: verbal aggression, physical aggression against objects, physical aggression against self, and physical aggression against other people. Reliability analysis indicated adequate internal consistency scores (coefficient alpha) for the current sample on the verbal aggression subscale and the physical aggression against others subscale. The overall alpha for the verbal aggression subscale was 0.94. The overall alpha for the physical aggression against others subscale was 0.81. However, with the fourth item (“Causes severe personal injury”) deleted, the alpha was 0.91. Therefore, a composite of only the first three items to quantify physical aggression against others was used. Lower internal consistencies were found for physical aggression toward objects or physical aggression against the self, with alphas equal to 0.01 and 0.42, respectively. Therefore, these two subscales are not reported in this study. The total number of occurrences of each type of event in the past 7 days was the variable used in all analyses.
RESULTS
Demographic Information
Of the subjects, 56 (10 female, 46 male) resided at a state psychiatric institution or at a Veterans Affairs Medical Center at the time of the evaluation, and 113 (78 female, 35 male) resided in various nursing homes in the New York City area.
Patients from the two hospital settings were compared via a series of independent-samples t-tests on cognitive and adaptive functioning, symptom severity, and certain demographic variables (age at assessment, years of education attained, and age at first hospitalization). As these groups were not statistically different at the 0.01 alpha level on any of the variables assessed, these groups were collapsed.
There were significant group differences between hospital and nursing home residents in age at the time of assessment and level of education achieved (
Table 1); the nursing home patients were older and had less education. The groups were also compared on levels of cognitive functioning, functional status, and symptomatology. Group differences were found on the cognitive composite, the Mini-Mental State Examination, self-care ability, social functioning, impulse control, and severity of negative symptoms. Because there were significant differences between patients residing in hospitals and those residing in nursing homes in demographic characteristics, levels of cognitive functioning, functional status, and symptomatology, the correlations with aggressive behavior were calculated separately for these variables.
Frequency of Aggressive Behaviors
The total number of occurrences of each particular behavior was used to evaluate the levels of verbal and physical aggression. A series of one-way analyses of variance (ANOVAs) found no group differences on any type of verbal aggression or physical aggression against others (
Table 2). Subjects assessed while residing in nursing homes were no different in severity or frequency of verbal or physical aggression toward others than were patients residing in a chronic psychiatric hospital.
For the patients residing in a hospital setting, verbal aggression was correlated at a statistically significant level with severity of positive symptoms (r=0.27, P<0.05), severity of general symptoms (r=0.31, P<0.05), and the SAFE impulse control items (r=0.29, P<0.05). Physical aggression against others was correlated with severity of negative symptoms (r=0.38, P<0.01), severity of general symptoms (r=0.55, P<0.001), SAFE total score (r=0.34, P<0.01), self-care (r=0.36, P<0.01), and impulse control subscales (r=0.37, P<0.01).
For the patients residing in the nursing homes, verbal aggression was correlated with severity of positive symptoms (r=0.29, P<0.01). Physical aggression against others was correlated with SAFE total score (r=0.20, P<0.05) and self-care scores (r=0.20, P<0.05).
Two regression analyses were run to identify the predictors of frequency of verbal and physical aggression against others (OAS scores), within each group. For each group, a simultaneous regression analysis was first used to determine if there was a significant overall relationship between age at assessment, cognitive, clinical, and social and adaptive functioning variables, and frequency of aggression. Significant simultaneous regression results led to reexamination of the variables in a forward entry stepwise regression analysis.
For the institutionalized patient group, the simultaneous regression analysis of the effects of positive symptom severity (PANSS Positive Symptom total), negative symptom severity (PANSS Negative Symptom total), cognitive functioning (Cognitive Composite), social (SAFE Social Functions score), and adaptive functioning (SAFE Self-Care score) on verbal aggression were not significant (F=1.29, df=5,50, P=0.282, R2=0.114). The same series of regression analyses was performed with physical aggression toward others as the dependent variable. The results of the simultaneous regression equation were statistically significant (F=03.91, df=5,50, P=0.005, R2=0.28). In the stepwise regression analysis, only negative symptom severity entered the regression equation at a statistically significant level (F=8.83, df=1,54, P=0.004, R2=0.14).
For the nursing home resident group, simultaneous regression analysis of the effects of positive symptom severity, negative symptom severity, cognitive functioning, and social and adaptive functioning on verbal aggression was significant (F=3.85, df=5,106, P=0.003, R2=0.154). In the stepwise regression analysis, only positive symptom severity entered the regression equation at a statistically significant level (F=11.02, df=1,110, P=0.001, R2=0.091). Simultaneous regression analysis of the overall effect of positive symptom severity, negative symptom severity, cognitive ability, and social and adaptive functioning on physical aggression in the nursing home population was significant (F=2.57, df=5,106, P=0.031, R2=0.108). In the stepwise regression analysis, only self-care ability entered the regression equation at a statistically significant level (F=4.10, df=1,110, P=0.045, R2=0.036).
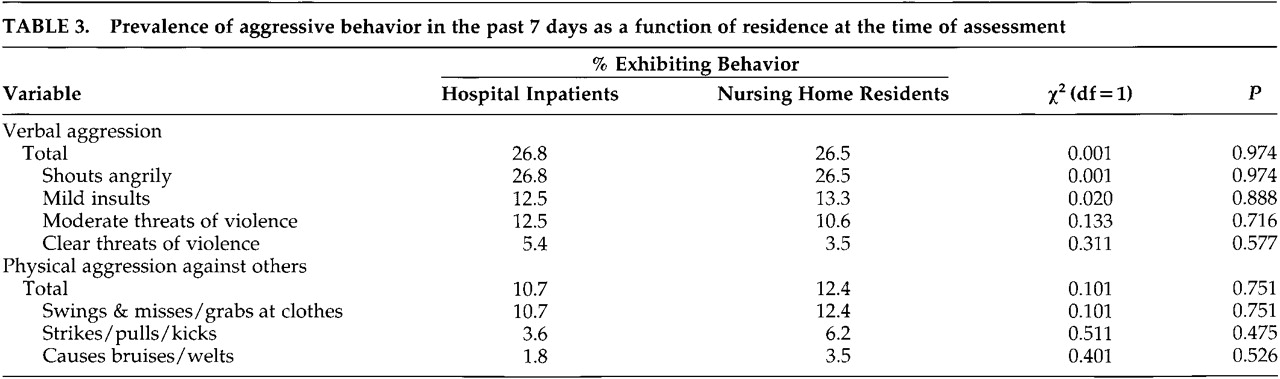
Prevalence of Aggressive Behavior
A series of 2×2 chi-square tests, with population and type of behavior serving as the variables, was conducted to determine the prevalence of each type of behavior within each group and whether more participants exhibited a particular type of aggression in one group than in the other. Occurrence of the behavior was defined as either presence or absence of the behavior over the past 7 days. There were no differences in the percentages of subjects within each group who exhibited verbal aggression or physical aggression against others, or on any of the specific aggressive behaviors examined.
Table 3 displays prevalence within each population and chi-square results.
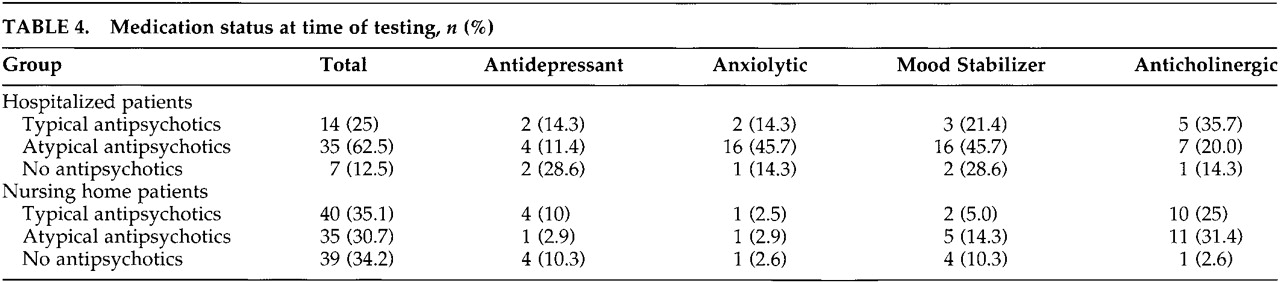
Medication Status
One-way ANOVAs were conducted to determine if patients receiving atypical, typical, or no antipsychotic medications had different rates of verbal or physical aggression. In the hospitalized patients, there were no significant differences in verbal aggression (F=0.358, df=2,53, P=0.701) or physical aggression (F=1.526, df=2,53, P=0.227) based on antipsychotic medication status. Similarly, the patients residing in the nursing homes did not differ significantly in verbal aggression (F=0.962, df=2,111, P=0.385) or physical aggression (F=0.747, df=2,111, P=0.476) based on medication status.
A series of
t-tests was conducted to determine if patients receiving other psychotropic medications differed in rates of verbal and physical aggression. For both the hospitalized and the nursing home groups, independent sample
t-tests were conducted, with verbal aggression and physical aggression as the dependent variables, for the following medications: antidepressants, anxiolytics (including both benzodiazepines and non-benzodiazepines), mood stabilizers (anticonvulsant medication and lithium), and anticholinergic medication. The only group difference observed was in the hospitalized group, where patients taking antidepressant medication were more verbally aggressive than patients not taking antidepressant medication (
t=−2.213, df=54,
P=0.031). No group differences were found in the hospitalized group for anxiolytic medication, mood stabilizers, or anticholinergic medication, nor were differences found in physical aggression for any of the medications. The nursing home patients did not differ in rates of verbal or physical aggression for any of the medications.
Table 4 summarizes medication status of hospitalized and nursing home patients.
DISCUSSION
The present study examined verbal and physical aggression in chronic, geriatric, poor-outcome schizophrenic patients in two types of settings: inpatient hospital and nursing home residences. Comparisons between these groups revealed differences in symptomatology, cognitive functioning, social functioning, and adaptive skills. Notably, the hospital group had significantly greater deficits in impulse control than the nursing home group. Despite this, the two groups did not significantly differ on any type or level of aggression rated with the OAS. Thus, nonaggressive episodes of impulsive behavior may be qualitatively different from aggressiveness.
Although medications are typically used in the treatment of aggressive behavior in schizophrenia, significant group differences were limited to verbal aggression in the hospitalized patients: those receiving antidepressant medications exhibited more verbal aggression than those not receiving antidepressants. Thus, it appears that in the hospitalized group, although some patients were receiving medications that may be given to control aggressiveness, these patients did not show less aggression than patients not receiving those medications. These results must be interpreted with caution, however, as cross-sectional data do not imply a causal relationship between medication status and behavior.
For both populations, verbal aggression was associated with severity of positive symptoms. Verbal aggression was also associated with general psychopathology and lack of impulse control in inpatients. Physical aggression was associated with lack of impulse control in both groups. However, physical aggression was associated with cognitive functioning and general psychopathology in inpatients, whereas it was associated with self-care and overall social-adaptive functioning in nursing home residents. Thus, the frequency and characteristics of aggression was similar in patients who were discharged to nursing home residences and those who remained in institutions, but it was associated with different factors in these two groups. Previous research has identified patient characteristics, specifically impulsiveness and aggression, that influence the referral process in determining if patients are discharged from a state hospital to a nursing home, or stay institutionalized.
1,4Potential limitation of this study should be mentioned. Although patients were excluded from the present study on the basis of a number of diseases found to affect cognitive functioning, other medical diseases may have influenced aggressiveness and should be considered in future analyses. The nursing home patients scored lower on the cognitive assessments and this may have reduced our ability to identify correlates of aggression with cognitive functions. Perhaps also relevant is that in patients with Alzheimer's disease, grossly advanced cognitive impairment is associated with a reduction in the frequency of aggressive acts.
20Another point to consider is that specific setting factors may contribute to aggression. Variables such as staff ratio, overcrowding, and ward milieu were not considered in these analyses but may influence aggressiveness.
8,31,32 The OAS relies on staff perceptions of behavior, and thus the difference between nursing home and hospital staff in their training and experience with patients with mental illness may have affected our findings.
As in some previous studies on aggression in younger patients with schizophrenia,
27,28,31 the present findings support the association between aggression and positive symptoms. However, the association between cognitive functioning and aggression was found only in inpatients and was limited to physical aggression. The frequency of physically aggressive behavior in this geriatric population (10.7% of hospital patients and 12.4% of nursing home residents) was less than that of younger, recently hospitalized patients (25.4%) in a recent study.
9 On the other hand, the relative rate of verbal aggression was similar in this geriatric group to that of younger groups of patients with schizophrenia.
8 Thus, the overall rate of aggressive acts in the present sample was only mildly reduced relative to younger, more acutely admitted patients.
9 This is potentially quite important, considering a number of factors that would seemingly reduce the likelihood of aggressive acts in geriatric patients. The present sample consisted of chronically hospitalized patients who were stabilized on medications, not acutely disturbed or unmedicated patients. The age and physical condition of these patients may have reduced their ability to perform physically aggressive acts, and their long history of institutionalization certainly reduces the likelihood that they used drugs or alcohol, which is known to be a risk factor for aggressive behavior in patients with schizophrenia.
53Statistically significant predictors were found for verbal and physical aggression, but they accounted for very little variance. Unfortunately, even using a wide range of clinical indicators, aggressive behavior is still very difficult to predict. The frequency of aggressive behavior in this study indicates that, as with the severity of positive symptoms previously reported,
11 there is considerable persistence of aggression into late life in patients with schizophrenia. Although the frequency of physically aggressive behavior in this population appears to be one-half that of younger acutely admitted patients, the potential impact of this aggressive behavior may be great. Physical frailty of these patients and the other patients around them associated with advanced age greatly increase risk of serious, possibly life-threatening injury from physically aggressive incidents that would have minimal impact on younger, healthier patients. As a result, aggression appears to remain a problem for patients with chronic schizophrenia up to the end of their lives.
ACKNOWLEDGMENTS
The authors thank Stephanie Bowler, R.N., Thomas Coleman, M.A., Dana Lieber, M.A., Dante Mancini, M.A., and Heidi Jacobson, M.A., for assistance in subject assessment and data collection. This research was supported by the assessment core (Philip D. Harvey, Principal Investigator) of the Mt. Sinai Mental Health Clinical Research Center (Kenneth L. Davis, PI) and the Mental Illness Research Education and Clinical Center, Veterans Integrated Service Network 3 (MIRECC-VISN 3), Department of Veterans Affairs. Portions of this paper were presented at the Society for Research in Psychopathology 14th Annual Meeting, Montreal, Quebec, October 2000.