Delirium is common among hospitalized elderly patients, with a prevalence estimated between 15% and 50%.
1,2 This syndrome is characterized by disturbances of consciousness, attention, and global changes in cognition. Moreover, abnormalities of mood, perception, and behavior are frequent. All these symptoms fluctuate during the day. The sleep patterns of delirious patients are usually disturbed as well. At times, the entire sleep–wake cycle is reversed: patients are drowsy and nap during the day, whereas night sleep is short and fragmented.
3 Melatonin, a hormone with hypnotic effects that increase the propensity to sleep and its duration and quality, is one factor that influences human sleep patterns.
4,5,6,7,8 Melatonin also seems to be related to the biological regulation of the circadian rhythms.
9,10,11,12,13 Thus, disturbances of sleep and circadian rhythms, as seen in delirious patients, and the known influence of melatonin on these physiological parameters warrant the search for a possible link between the delirium syndrome and melatonin. To date, the only study investigating a possible link between delirium and melatonin is that of Mukai et al.,
14 who studied patients with alcohol withdrawal delirium and reported changes in melatonin production during the delirium. Although these changes were specific for the delirium period, their pattern was inconsistent. According to clinical expression, the delirium syndrome can be classified into three subtypes: hyperactive, hypoactive, and mixed.
15 Given the known effects of melatonin, we hypothesized that some relation could exist between melatonin blood levels and the subtypes of delirium. A high level of melatonin may be expected in the hypoactive type and a low level in the hyperactive type. The aim of this study was to measure urinary 6-sulphatoxymelatonin (6-SMT) as an indicator of the melatonin level in all three groups of delirious patients and to look for a link between the melatonin level and the clinical subtypes of this syndrome.
RESULTS
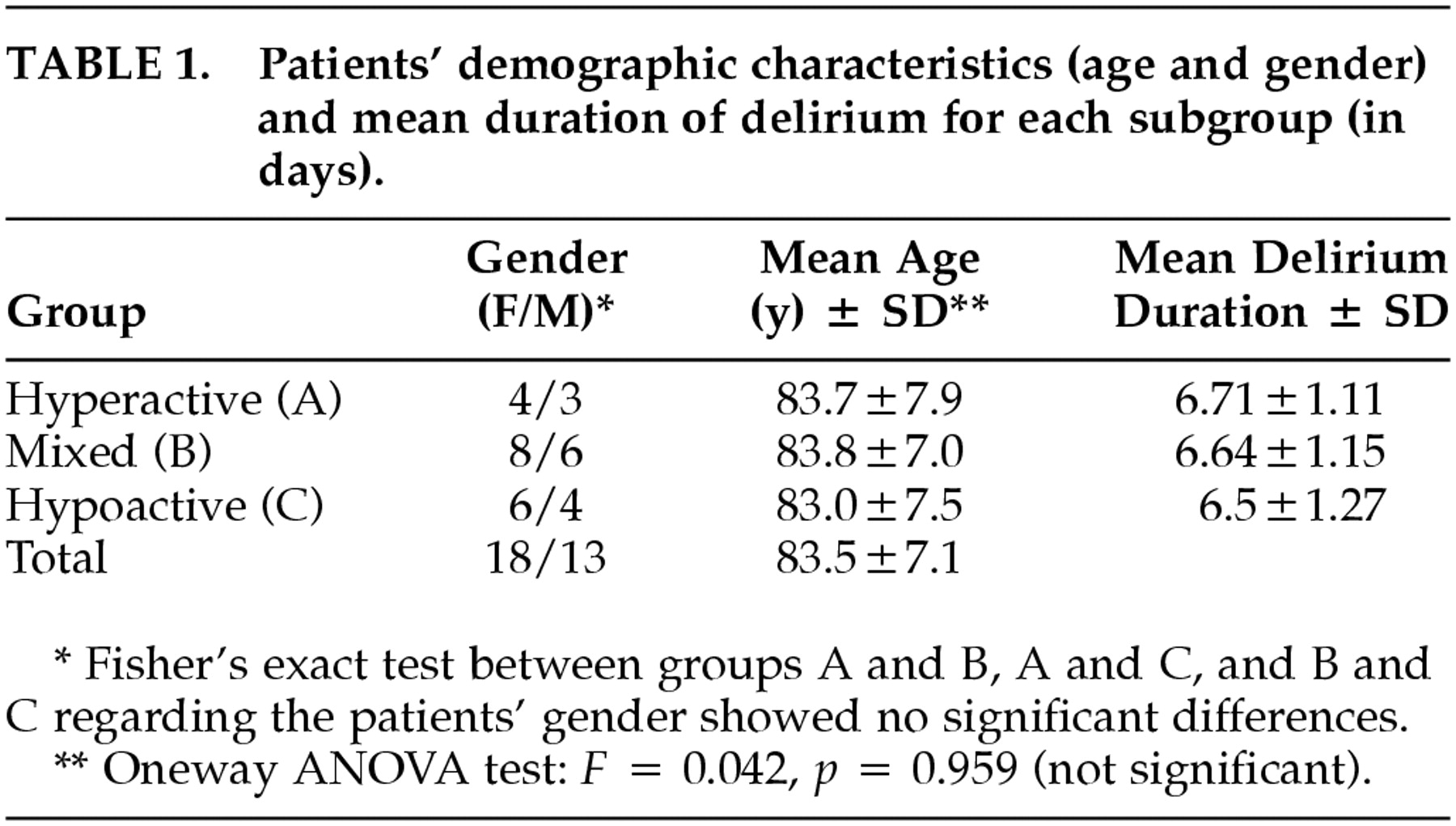
The study investigated 31 patients: 18 women and 13 men; the mean age was 83.5 ± 7.1 (ranging from 72 to 94 years). Clinically, 7 patients were hyperactive, 10 hypoactive, and 14 mixed. There were no significant differences between the groups regarding mean age, gender, and delirium duration (
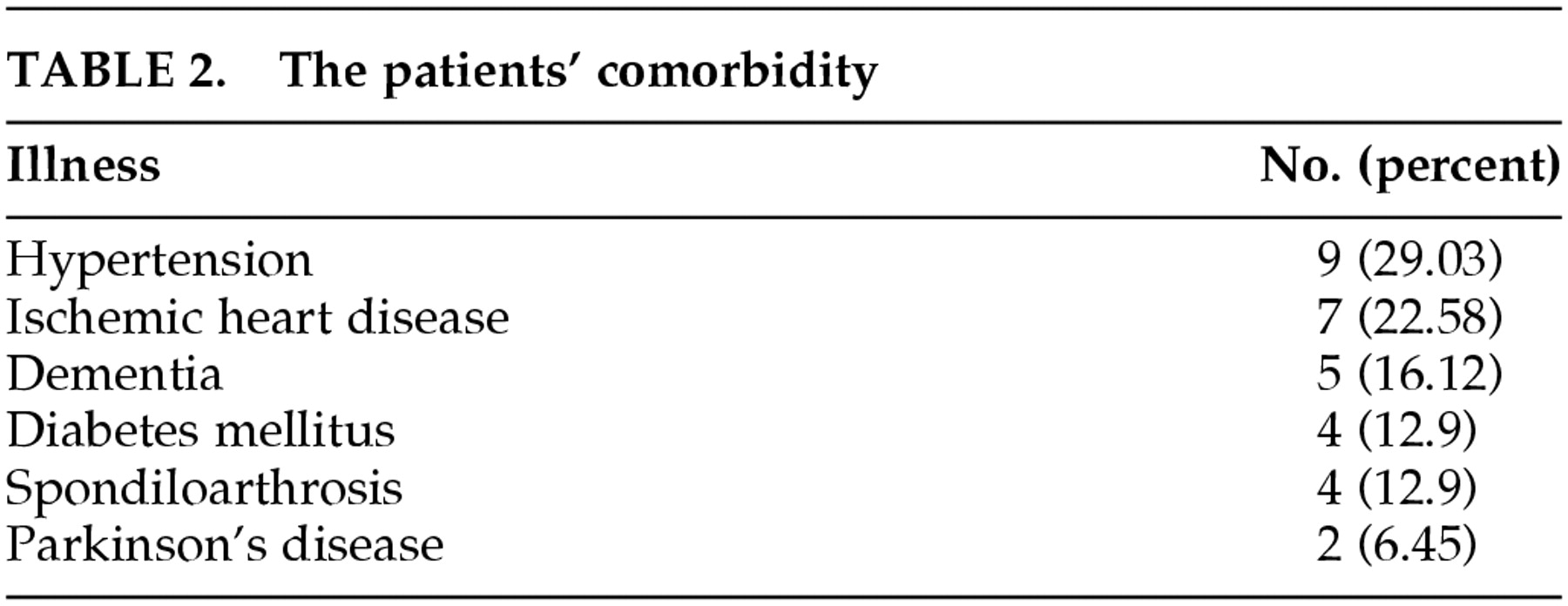
Table 1). All the patients suffered from various chronic diseases and were taking between 3 and 7 different drugs (
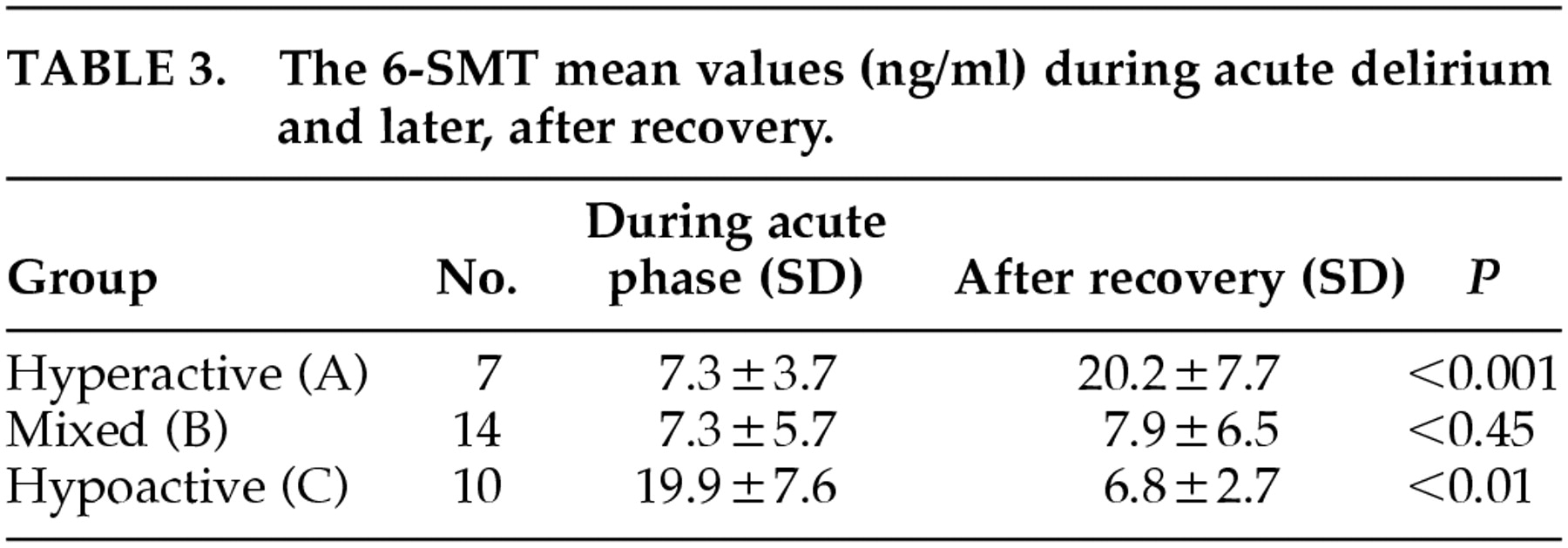
Table 2). Among the hyperactive patients, the levels of 6-SMT were lower during the acute delirium state than after recovery (
p < 0.001). In contrast, among the hypoactive patients, the levels of 6-SMT were higher during the acute delirium state than after recovery (
p < 0.01). With the mixed patients, there was no difference in the level of 6-SMT between the two phases of delirium (
p < 0.45) (
Table 3). The results of the MANOVA test indicated that a common factor exists between the 6-SMT values in all three groups, in both measurements:
F = 58.37 on two degrees of freedom,
p < 0.001.
DISCUSSION
Our data suggest that a relation exists between the delirium syndrome and melatonin. This relation was demonstrated previously in a group of alcohol withdrawal-induced delirium patients.
14 This is also suggested by the inverse relationship between the incidence of delirium and the length of the daylight hours, as we have recently reported.
32 Moreover, the results support our early hypothesis that patients, when compared at the recovery stage, with delirium of the hyperactive subtype may have lower levels of 6-SMT, whereas those with the hypoactive subtype have higher levels of 6-SMT. No significant differences between the two stages were found in patients with delirium of the mixed type. Hence, the unanswered question is the meaning of these data. Is the clinical expression of the delirium syndrome influenced by the sedative-hypnotic effects of melatonin? Such a relation was previously reported by Wahlund and co-workers, who found that melatonin levels were associated with the level of psychomotor activity in subtypes of affective disorders.
33 According to the clinical picture of delirious patients, Liptzin and Levkoff classified the delirium syndrome into subtypes.
15 These subtypes differ not only in the symptom profile and severity, but they also may differ in pathophysiologies, responsiveness to therapeutic interventions, and outcome.
34 Given the known sedative effect of melatonin, it is tempting to speculate that the clinical expression of the hyperactive or hypoactive types of delirium is related to the amount of its secretion: low levels of melatonin in hyperactive and high levels of melatonin in hypoactive patients. However, the question still arises as to why it is higher in some patients and lower in others. Further studies are needed to elucidate whether there is a connection with either the extrinsic factors that generate delirium or the intrinsic physiological characteristics of each patient. Notably, this study is the first to report a link between the clinical subtypes of delirium and a biochemical parameter (the urinary 6-SMT). The limitation imposed by the small number of patients here suggests the need for further studies before any conclusion can be reached regarding the role of melatonin in delirium.