W hite matter changes are defined as areas with high signal intensities on T2-weighted magnetic resonance imaging (MRI) and areas with low attenuation on Computed Tomography (CT). White matter changes are found often in patients with vascular dementia, especially of subcortical subtypes including Binswanger’s disease, and are generally considered to be a consequence of chronic ischemia associated with microangiopathy.
1,
2 However, white matter changes are not associated exclusively with vascular dementia and are common in patients with Alzheimer’s disease,
3,
4,
5 though the mechanisms for the development of white matter changes in Alzheimer’s disease are not yet fully understood.
Presently, only limited numbers of MRI or CT studies have examined the association of white matter changes with the neuropsychiatric manifestations of Alzheimer’s disease, and there is a lack of agreement among the results of these studies. Some studies have shown a significant association between white matter changes and certain neuropsychiatric symptoms, such as depression,
6 apathy,
7 suicidal ideation or low self-esteem,
8 and aberrant motor behavior,
9 whereas other studies have failed to find any relationship in Alzheimer’s disease patients.
10,
11 No previous study on white matter changes in Alzheimer’s disease has indicated a relationship between psychotic symptoms and white matter changes, though a CT study conducted for Alzheimer’s disease patients suggested a relationship between delusion and lacunar infarcts of white matter.
12 Psychotic symptoms also have been observed in many white matter disorders, such as adult-onset metachromatic leukodystrophy,
13,
14 multiple sclerosis,
15 Binswanger’s disease,
16 and normal pressure hydrocephalus.
17,
18 These discrepancies may be related to the differences not only in study population but in definition and quantification method of white matter changes or assessment method of neuropsychiatric symptoms.
Most previous studies on white matter changes of Alzheimer’s disease have examined only the relationship between global white matter changes and neuropsychiatric symptoms without exploring further the effect of regional white matter changes,
7,
9 –
11 though specific focal changes of cerebral white matter may contribute to the development of particular neuropsychiatric symptoms.
This study aimed to examine the relationship between white matter changes seen on MRI and neuropsychiatric symptoms in probable Alzheimer’s disease patients. We tried to explore the association of brain region-specific white matter changes and global white matter changes with those symptoms.
METHOD
Subjects
Subjects for this study were recruited from a cohort of Alzheimer’s disease patients who regularly follow up at the Dementia & Age-Associated Cognitive Decline Clinic of Seoul National University Hospital in Seoul, Korea. All candidate patients were examined by psychiatrists with advanced training in neuropsychiatry and dementia research according to the protocol of the Korean Version of the Consortium to Establish a Registry for Alzheimer’ disease Assessment Packet (CERAD-K).
19,
20 Reliable informants were interviewed to acquire accurate information regarding the cognitive and functional changes and medical history of the subjects. Psychiatric, general physical and neurological examinations, and routine laboratory tests were performed. After reviewing all of the available raw data, a panel of four psychiatrists with expertise in dementia research made the clinical decisions, including clinical diagnosis, clinical dementia rating (CDR),
21 and scoring for modified Hachinski Ischemic Scale (mHIS).
22 All the subjects included in this study met both the Diagnostic and Statistical Manual of Mental Disorders (DSM–IV) criteria for dementia
23 and the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’ disease and Related Disorders Association (NINCDS-ADRDA) criteria for probable Alzheimer’s disease.
24Exclusion criteria consisted of any serious medical, psychiatric, and neurological disorders that could affect mental function; evidence of focal brain lesions on MRI, including lacunar infarcts and hematoma; presence of severe behavioral or communication problems that would make clinical or MRI examination difficult; and absence of a reliable informant. The Institutional Review Board of Seoul National University Hospital approved the study protocol and informed consent was obtained from all of the subjects and their relatives.
Assessment of Cognitive Functions and Neuropsychiatric Symptoms
We assessed the cognitive function of the subjects with eight neuropsychological tests (verbal fluency, animal category; 15-item Boston naming test; Mini-Mental State Examination; word list memory; word list recall; word list recognition; constructional praxis; constructional recall) included in CERAD-K.
19 The subjects’ neuropsychiatric symptoms were assessed during an interview with the informant by using CERAD Behavioral Rating Scale for Dementia (BRSD).
25 The BRSD includes 46 items on the behavioral problems and psychiatric symptoms of dementia patients and each is scaled by frequency of occurrence. Severity is also reflected in the BRSD in two ways: first, a number of items are followed by a probe, and the score is adjusted according to the response to the probe; and second, a number of items are combined to generate six factor-based subscale scores (Depressive Symptoms, Inertia, Vegetative Symptoms, Irritability/Aggression, Behavioral Dysregulation, and Psychotic Symptoms), so that the more items that are rated present on a given subscale, the greater the severity of the construct represented by the subscale.
26MRI Acquisition and Assessment of White Matter Changes
MRI was performed using General Electronics 1.5-tesla SIGNA Scanner (GE Medical Systems, Milwaukee, U.S.). Spin-echo pulse sequences were used to generate a series of 15 T2-weighted images (repetition time = 4,500 msec, echo time = 99 msec, number of excitations = 1), which then were used to assess white matter changes. These were complemented by either T1-weighted (repetition time = 500 msec, echo time = 12 msec, number of excitations = 1) or fluid-attenuated inversion recovery (FLAIR) (repetition time = 10,002 msec, echo time = 133 msec, inversion time = 2,200 msec, number of excitations = 1) images to discriminate white matter changes from lacunar infarcts. In all image acquisitions, the field of view was 210×210 mm, and the matrix size was 256×256.
White matter changes on MRI were classified as ill-defined hyperintensities ≥ 5 mm on T2-weighted images. Lacunar infarcts were classified as well-defined lesions with a diameter of > 2 mm with hyperintensity on T2-weighted images and the hypointensity on T1-weighted or FLAIR images. If lesions with this characteristic were ≤ 2 mm, they were considered as perivascular spaces, except around the anterior commissure, where perivascular spaces can be large. Changes in the basal ganglia were rated in the same way and considered white matter lesions even if located in the gray matter nuclei, which contains a small amount of white matter.
White matter changes were assessed by a scale proposed by the European Task Force on Age-Related White Matter Changes.
27 Eight different regions were rated separately: left and right frontal areas (the frontal lobes anterior to the central sulcus); left and right parieto-occipital areas (the parietal and occipital lobes together); left and right temporal areas (the border between the parieto-occipital and temporal lobes was approximated as a line drawn from the posterior part of the Sylvian fissure to the trigone areas of the lateral ventricles); and left and right basal ganglia (the striatum, globus pallidus, thalamus, internal and external capsules, and insula). Rating scores for white matter changes of frontal, parieto-occipital, and temporal areas were designated as follows: 0 = no lesions including symmetrical, well-defined caps or bands; 1 = focal lesions; 2 = beginning confluence of lesions, and 3 = diffuse involvement of the entire region, with or without involvement of U fibers. Scores for basal ganglia lesions were as follows: 0 = no lesions; 1 = 1 focal lesion ≥5 mm; 2 = >1 focal lesion; and 3 = confluent lesions. The overall score for white matter changes was calculated by adding up the eight regions’ scores. The interrater reliability between two psychiatrists for the rating of each region was examined with 20 randomly selected patients, and good kappa coefficients were obtained: 0.77 for left frontal, 0.70 for right frontal, 0.73 for left parieto-occipital, 0.64 for right parieto-occipital, 0.58 for left temporal, 0.57 for right temporal, 0.69 for left basal ganglia, 0.62 for right basal ganglia. Final white matter changes ratings were carried out by one psychiatrist who had no knowledge of the subjects’ clinical data, including cognitive test results and BRSD scores.
Statistical Analysis
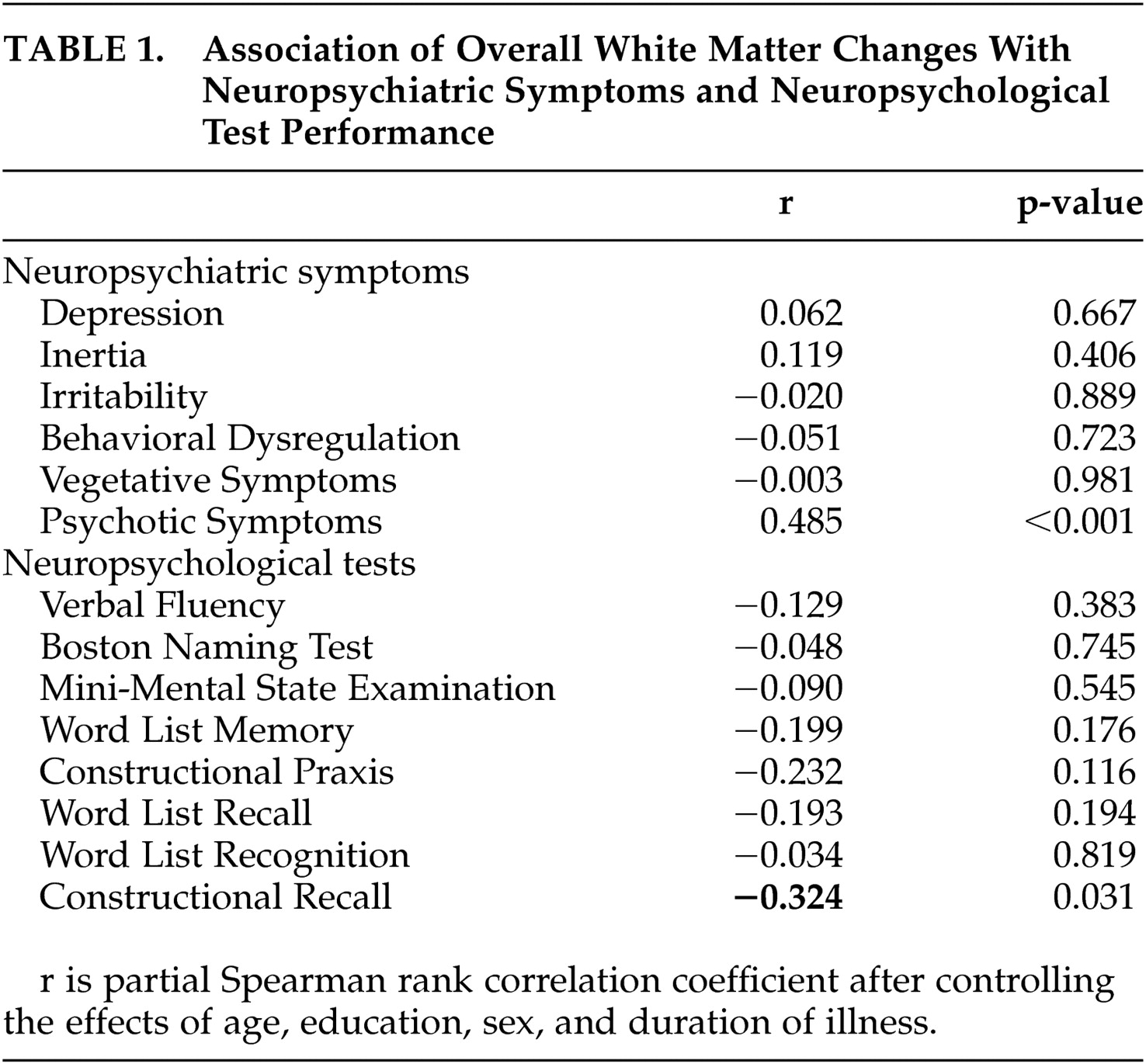
Nonparametric statistical analyses were performed because the scores of white matter changes were assessed as ordinal scales. All correlations were examined by using partial Spearman rank correlation coefficients after controlling for the effects of age, education, sex, and duration of illness, which have been associated with neuropsychiatric symptoms,
28,
29 cognitive dysfunctions
30 and white matter changes
31 in Alzheimer’s disease. For all analyses, α level was set at 0.05. We did not make any adjustment for multiple comparisons because we tried to explore only the relationship between neuropsychiatric manifestations and white matter changes with no specific hypotheses to be tested. All statistical analyses were carried out with the SAS program, version 6.12 (Statistical Analysis Systems).
DISCUSSION
This study showed that the severity of white matter changes significantly correlated with specific psychotic symptoms. As far as we know, this is the first report that demonstrates the relationship between white matter changes without infarcts or lacunae and psychotic phenomenon in Alzheimer’s disease patients.
The reason that previous studies conducted for Alzheimer’s disease subjects could not find the relationship between psychosis and white matter changes may be related to the nature of psychotic symptoms included in analyses. While there is no formal classification yet, the psychotic symptoms associated with Alzheimer’s disease could be divided into three groups: paranoid delusions, delusional misidentification, and hallucinations.
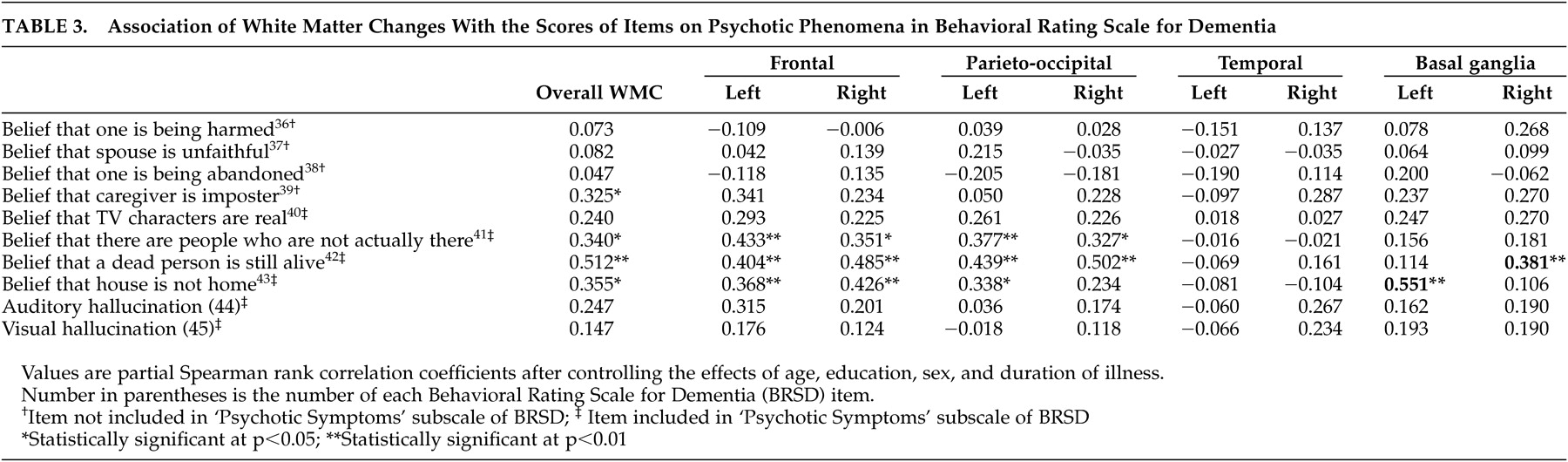
32 The psychotic symptoms subscale of BRSD, which significantly correlated with overall and regional white matter changes in our analyses, does not include items on paranoid delusion, but only includes delusional misidentification items,
32,
33 (e.g., phantom boarder; belief that a dead person is still alive; belief that house is not home; capgras syndrome), and hallucination items (e.g., auditory and visual hallucination). In additional analyses on individual BRSD items for specific psychotic symptoms, only delusional misidentification items were significantly correlated with white matter changes; paranoid delusion and hallucination items were not. In contrast to our study, previous studies either did not assess or did not analyze delusional misidentification separately from paranoid delusion or hallucination.
6 –
11 Then, in case of hallucination, the number of patients with hallucinations (three patients with visual hallucination and three patients with auditory hallucination) was too small to draw a conclusion on the relationship with white matter changes.
Very limited numbers of studies
33,
34 focused specifically on delusional misidentification associated with regional brain dysfunction in Alzheimer’s disease patients. Mentis et al.,
34 referring to cerebral metabolic findings, suggested that abnormal frontal integration of perceptual information from multimodal association cortex and affective information from paralimic-limbic structures give rise to delusional misidentification in Alzheimer’s disease patients. Similarly, white matter changes in frontal or parieto-occipital region may possibly disrupt the functional connection between frontal cortex and other association cortex or paralimbic-limbic structures and, as a result, lead to delusional misidentification. White matter changes of basal ganglia also may contribute to the development of delusional misidentification through frontal-subcortical connection.
35A CT study conducted by Förstl et al.
33 also indicated an accentuated degeneration of the right frontal lobe with relative preservation of the left frontal lobe in association with delusional misidentification. In our study, the correlation coefficients between white matter changes and delusional misidentification symptoms were greater relatively for the right side than for the left side. These findings support the importance of right side cerebral dysfunction for the development of delusional misidentification phenomena.
Depression,
6 apathy,
7 suicidal ideation,
8 and aberrant motor behaviors
9 associated with white matter changes in Alzheimer’s disease patients have been reported by some authors. However, none of these findings was replicated by other studies. We also could not find any significant relationship between such symptoms and white matter changes. The inconsistent findings may arise from differences in study subjects, and definition and quantification method of white matter changes as well as in neuropsychiatric symptom assessment. One study included not only Alzheimer’s disease patients, but dementia patients with other causes.
6 Another selected only Alzheimer’s disease patients with no vascular risk factors.
8 Excluding the cases with vascular risk factors may result in excluding severe white matter changes and distorting the clinical significance of white matter changes. In contrast, we targeted probable Alzheimer’s disease patients without any evidence of definite cerebrovascular disease, but did not exclude cases with vascular risk factors, unless they were serious enough to alter present mental function. In some studies, periventricular changes in the form of caps or smooth halos were included in the white matter changes category,
9,
10 but not in other studies including ours. Caps or smooth halos are known to be of nonischemic origin, while other white matter changes represent ischemic tissue damage and have different clinical significance compared to halos or caps.
11,
36,
37Some possible limitations should be discussed. First, we did not consider the degree of cortical brain atrophy as a covariate in correlation analyses because there was little evidence supporting the significant relationship between regional cortical atrophy and neuropsychiatric symptoms in Alzheimer’s disease. Some functional imaging studies using single photon emission tomography or positron emission tomography, however, indicated that regional cortical dysfunctions were associated with certain neuropsychiatric manifestations including psychotic symptoms.
34,
38 –
40 Further multimodal imaging studies are, therefore, needed to differentiate regional cortical and subcortical contributions to the development of neuropsychiatric symptoms in Alzheimer’s disease. Second, as described in the methods section, we did not make any adjustment of a significance level for multiple statistical comparisons because this study was an exploratory one. While we can get very important clues about the relationships between white matter changes and neuropsychiatric manifestations in Alzheimer’s disease, the possibility of false positive associations cannot be excluded. Therefore, the findings from this study need to be replicated before they can be confirmed.
In conclusion, the results of this study indicate that white matter changes in Alzheimer’s disease patients, especially located in frontal and parieto-occipital regions, probably contribute to the development of a specific type of psychotic symptom, namely, delusional misidentification. Other neuropsychiatric or behavioral symptoms seem not to be related with white matter changes.