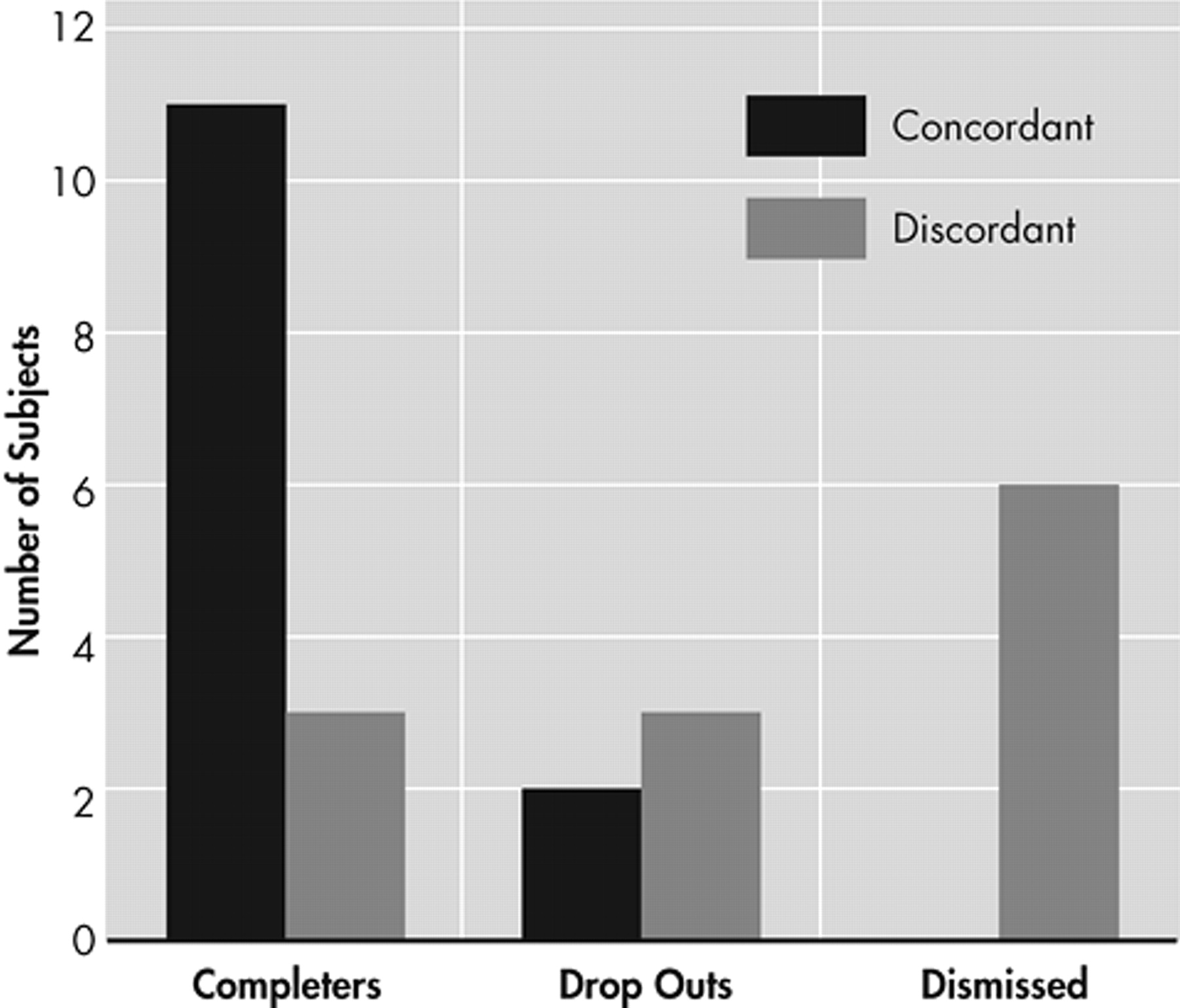
These results suggest that there is variation in the neurophysiological function of potential cocaine-dependent study participants prior to enrollment in a medication treatment trial for dependency. In addition, this variation may be related to the probability of trial completion, dismissal of or dropout by the participant. A significant percentage of participants who successfully completed the trial were classified as concordant in their brain state as opposed to those who did not complete the trial. The neurophysiological differences reported here are significant even after controlling for benzoylecgonine levels, suggesting that there are fundamental differences in brain function which are independent of recent drug use. The differences in outcome among these participants cannot be explained on the basis of the many common clinical factors that contribute to heterogeneity in clinical trials.
36 Consistent with previous research, the levels of depression or craving
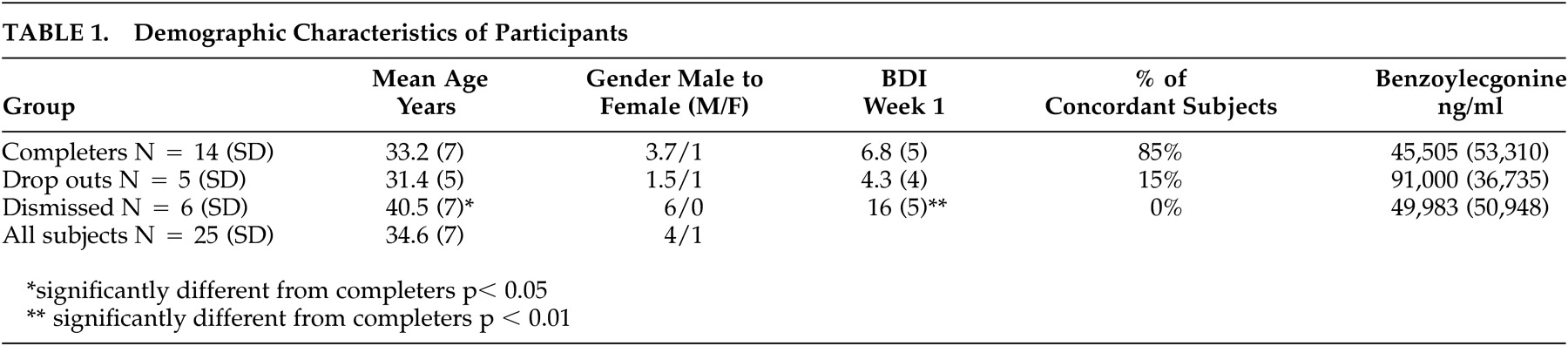
23 were not powerful factors in explaining participant retention. Those who were removed from the study did have slightly higher levels of depression than either those who remained or dropped out, but there was considerable overlap in the range of depression scores among the three outcome groups. Congruent with Kampman et al.’s work,
24 we observed a statistical trend toward a difference in levels of benzoylecgonine between those who completed and those who dropped out; however, this indicator did not reach the level of significance. Because of the moderately strong association between cordance and cerebral perfusion,
28 one may hypothesize that the participants who completed the study had higher levels of cerebral perfusion globally, and therefore may have suffered less brain dysfunction than those participants who dropped out or were dismissed. Studies of cerebral perfusion in cocaine-dependent participants without apparent neurological defects have shown widespread perfusion defects.
37 It is important to note, however, that no direct measurements of perfusion were performed on any of the participants in this study. Future studies of treatment retention should examine other indicators of brain dysfunction in cocaine dependent trial participants, including brain structure using magnetic resonance imaging (MRI) as well as neuropsychological test results. For example, cocaine dependence has been associated with an arrest of normal white matter volume increase as well as evidence of premature white matter damage with age.
18,
38 The participants that were dismissed were significantly older, more dysfunctional (as seen in their inability to follow protocol), and more depressed. Further examination with measures such as single-photon emission computed tomography (SPECT) or functional magnetic resonance imaging (fMRI) could elucidate specific brain structures giving rise to concordant and discordant brain states. No conclusions can be drawn about the relationship between baseline cordance characteristics and effectiveness of the medication examined in the treatment trial. This study used only retention, a crude indicator of treatment outcome, as the measure of interest. The small sample size precludes our examining indices of treatment effectiveness, and the medications were assigned randomly and not according to the neurophysiological characteristics of the participants. Internal validity would have been increased if participant baseline QEEG measures were all obtained at identical abstinence length. Our inability to collect baseline measures at identical times may have confounded our measure, with differences in brain activity dependent upon length of abstinence or initiation of treatment. Future studies with more participants should examine the relationship between neurophysiological measures and clinical indicators of outcome such as frequency and/or intensity of use, periods of abstinence, functional impairment, or derived measures such as the treatment effectiveness score (TES).
39 Examination of these types of outcome measures will help determine whether neurophysiological heterogeneity is related to the overall functional outcome in cocaine-dependent participants.