D elayed hypoxic leukoencephalopathy is a recognized complication of carbon monoxide poisoning,
1 –
3 asphyxial gas poisoning,
4 surgical anesthesia,
4 cardiac arrest,
4,
5 and opiate or benzodiazepine overdose.
6 –
10 It typically manifests 2 to 40 days after apparent recovery from an obtunded state, and patients demonstrate cognitive impairment, upper motor neuron signs, gait disturbance, or psychosis.
1,
4 Case Reports
Case 1
A 39-year-old woman with a history of major depression became obtunded with room air oxygen saturation of 37% following an overdose of liquid methadone and cocaine. After a brief intensive care stay for aspiration pneumonia and hypotension, she was able to return to work. Four weeks after her discharge, she was readmitted with mental status decline. On examination, she was disoriented and tangential, with profound impairment of attention and short-term memory. Her reflexes were diffusely brisk, with a right-sided Babinski response. Gait was unsteady, with stumbling to the left.
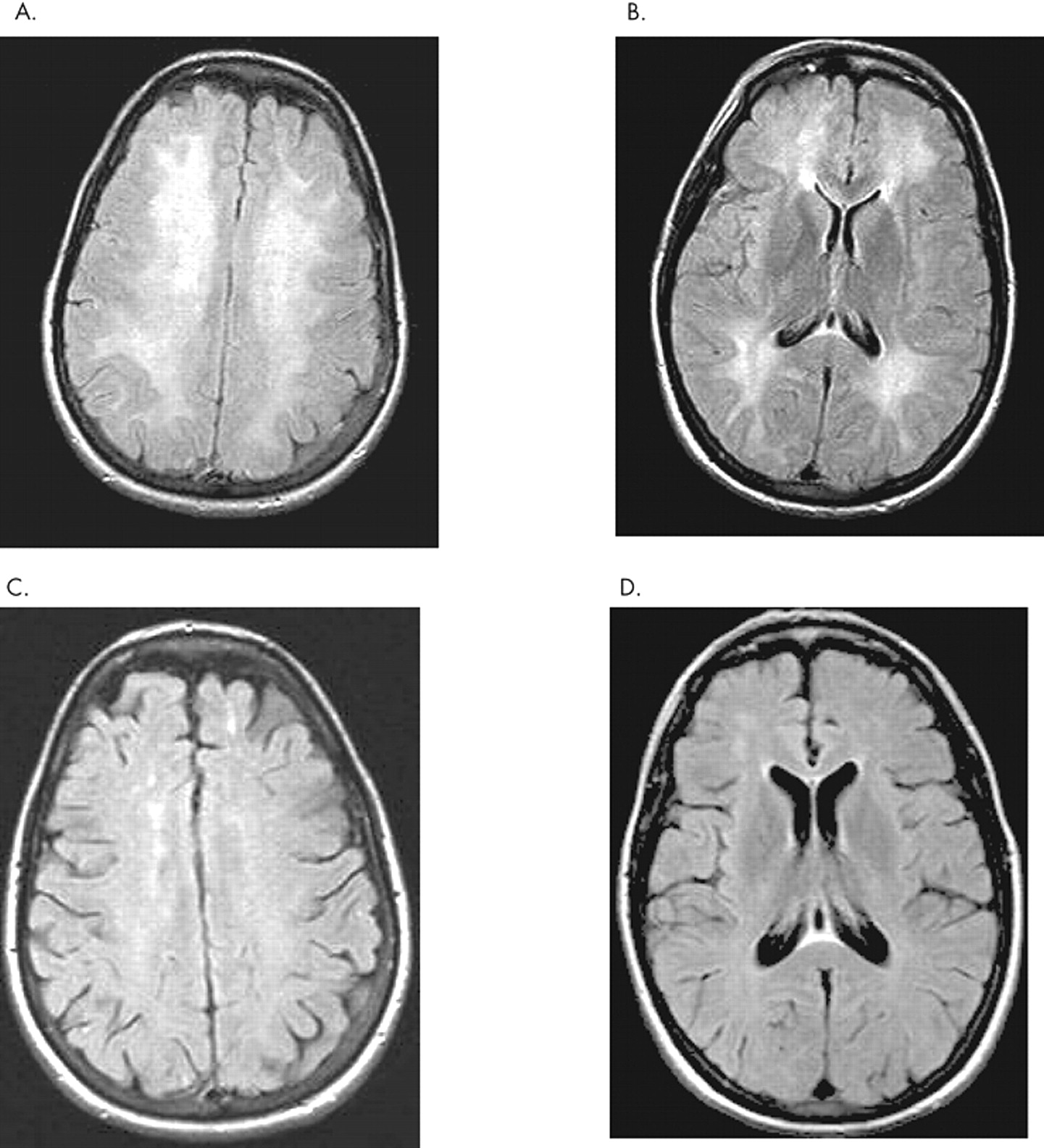
An MRI of the brain (
Figure 1 ) showed diffusely increased T2/FLAIR signal in the white matter of the centrum semiovale extending to the subcortical region, with diffuse restriction on diffusion weighted imaging. The basal ganglia and posterior fossa were normal in appearance. Single voxel magnetic resonance spectroscopy (MRS) showed mildly decreased
N -acetylaspartate peaks and no evidence of abnormal lactate. EEG showed continuous polymorphic 2–8/sec delta-alpha waves.
Laboratory studies were significant for elevated CSF myelin basic protein of 46.33 ng/ml (normal range 0.07 to 4.1 ng/ml), with normal protein, glucose, cell count, IgG index, and oligoclonal bands; AST 159 (14–50 U/liter); ALT 97 (9–52 U/liter). Leukocyte arylsulfatase-A was 5.3 (normal greater than or equal to 2.5 units per liter). Erythrocyte sedimentation rate, serum folate, thyroid-stimulating hormone, free T4, T3, Epstein-Barr virus and cytomegalovirus by polymerase chain reaction were normal. Antiglutamic acid decarboxylase, antithyroglobulin, anticardiolipin, beta-2-glycoprotein, double stranded DNA, and antinuclear antibody titers were negative.
Thirty-two weeks after the patient’s overdose, exam showed bilateral gegenhalten with grasp and palmomental reflexis, diffuse hyperreflexia, and flexor plantar responses. One year postoverdose, she continued to have emotional lability, fatigue, and impaired attention that prevented her from working or driving. MRI showed diffuse cerebral volume loss, with incomplete resolution of white matter signal abnormalities. WAIS-R had been administered 10 years prior (following a minor motor vehicle accident). Recognizing psychometric differences between the two editions, WAIS-III administered 1 year postoverdose reflected the following declines: verbal IQ from 102 to 89, performance IQ from 98 to 81, and full scale IQ from 100 to 85, with major declines in immediate memory, abstraction, inductive reasoning, and block design.
Case 2
A 51-year-old woman treated with transdermal fentanyl for fibromyalgia was switched to oral methadone. Two days later, in an apparent overdose, her family found her unconscious. Following 2 days of intubation she made a complete recovery. Twenty-one days after the event her daughter noted mental status decline, including staring at a blank TV screen, loss of interest in board games, and paranoid delusions that neighbors were watching her. By 28 days after the event, the patient was catatonic, with no participation in activities of daily living or interaction with others, incontinence of bowel and bladder, and frequent automatisms (stroking of the face and rapid sequential hip flexion). Examination showed hypokinetic-rigid mutism, vocalization only to pain, and normal upper extremity reflexes despite asymmetric rigidity. Lower extremity reflexes were absent.
Cerebrospinal fluid studies revealed myelin basic protein 41.33 ng/ml and protein 64 mg/dl (normal range 15–45 mg/dl), with normal glucose, cell count, IgG index, and gram stain; oligoclonal bands were absent. Serum toxicology screen was positive for methadone, and urinalysis was positive for leukocyte esterase and bacteriuria.
A brain MRI showed diffuse symmetric T2/FLAIR hyperintensity in the hemispheric white matter bilaterally. An EEG showed continuous polymorphic 2–6/sec delta-theta waves, with right hemispheric prominence.
Two weeks after the onset of symptoms, the patient showed mild improvement, participating in prompted voiding and walking with physical therapists, but remaining dependent in all respects.
At follow-up 16 weeks postoverdose, the patient was no longer mute and complained of fatigue, cough, generalized weakness, and myalgia. Exam showed Mini-Mental State Examination (MMSE) score of 27/30; she was unable to draw intersecting pentagrams, missed the date, and had 5-minute recall of two-thirds objects. There was mild asymmetric rigidity. Her coordination, strength, and reflexes were normal. Her gait was slow, antalgic, and wide-based.
At 38 weeks postoverdose, short-term memory and balance impairment persisted, and she required continued assistance with self-care. An MRI showed interval cerebral atrophy with incomplete resolution of white matter signal abnormalities.
Case 3
A 56-year-old woman with a history of depression was admitted with acute renal failure and rhabdomyolysis following intentional overdose of methadone, fentanyl, and benzodiazepines. She was discharged at baseline 11 days later. Day 15 postoverdose she developed severe progressive cognitive decline. An exam showed MMSE score of 15/30, with disorientation and profound impairment of attention and short-term memory. There were a right pronator drift, diffusely brisk reflexes with clonus (except for trace bilateral Achilles), and an unsteady shuffling gait.
Laboratory studies from day 18 postoverdose included normal CBC; complete metabolic panel; and CSF protein, glucose, and cell count. The blood sample for arylsulfatase-A was lost due to an error in the laboratory.
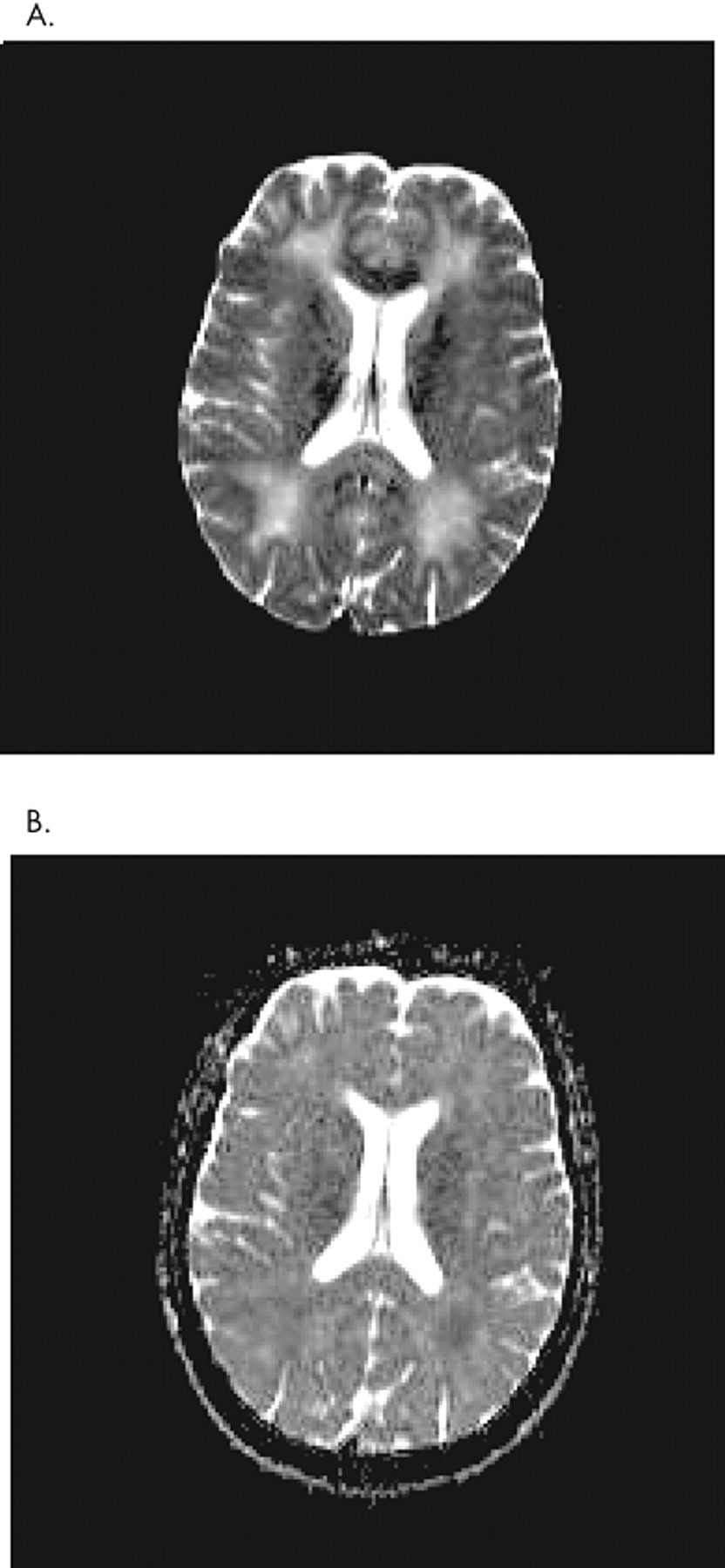
An MRI on day 14 postoverdose showed marked confluent T2/FLAIR hyperintensity, with diffusion restriction involving nearly the entire periventricular and subcortical white matter. Diffusion restriction was still present 31 days postoverdose (
Figure 2 ). An EEG showed diffuse slowing. At 8 weeks postoverdose, the patient required full-time supervision for self-care and had persistent impairment of short-term memory and attention.
DISCUSSION
Delayed hypoxic leukoencephalopathy is a rare complication of hypoxic-ischemic encephalopathy, occurring in 2.75% of victims of carbon monoxide poisoning.
1 Both the pathophysiologic mechanism and the reason why it affects only a subset of hypoxic-ischemic patients remain unclear. Prolonged moderate hypo-oxygenation of subcortical white matter due to impaired oxygen delivery and/or hypotension is thought to disrupt ATP-dependent enzymatic pathways involved in myelin turnover, resulting in delayed demyelination.
4,
11 In two patients with delayed hypoxic leukoencephalopathy,
8,
10 levels of arylsulfatase-A were 27%–50% of normal. Metachromatic leukodystrophy, a neurodegenerative disease characterized by progressive central and peripheral nervous system demyelination, is the clinical phenotype associated with deficiency of this enzyme required for sulfatide metabolism. Following a hypoxic event, sulfatide accumulation during a period of accelerated remyelination could cause delayed demyelination in those with mild arylsulfatase-A deficiency. However, normal levels of arylsulfatase-A in two of our patients, and in three reported previously,
5,
6,
9 suggest that subclinical arylsulfatase-A deficiency is not a necessary predisposing factor.
Use of the term “toxic leukoencephalopathy” to describe leukoencephalopathy due to carbon monoxide or intravenous heroin exposure
12,
13 can be misleading, as it implies a myelinotoxic rather than hypoxic-ischemic etiology. Toxic leukoencephalopathy occurs following exposure to a number of myelinotoxic agents, including inhaled heroin. The latter can cause spongiform leukoencephalopathy, which is associated with a lactate peak on white matter MR spectroscopy.
14 –
16 This suggests a defect in energy metabolism, potentially via formation of a mitochondrial toxin during heating of heroin (or its additives) on an aluminum spoon to create the inhaled vapor. Spongiform leukoencephalopathy is distinguished from delayed hypoxic leukoencephalopathy by T2 hyperintensity of white matter tracts of the brainstem, cerebellum, and supratentorial brain-sparing frontal white matter and anterior limb of the internal capsule,
15 –
18 and the absence of a biphasic course. Whereas spongiform leukoencephalopathy causes intramyelinic vacuolar edema,
15,
19 autopsy
4 and biopsy
8 of delayed hypoxic leukoencephalopathy show diffuse hemispheric demyelination sparing subcortical u-fibers, but without vacuolization.
In addition to the anatomic distribution of MRI signal changes, prolonged diffusion restriction may be useful in the diagnosis of delayed hypoxic leukoencephalopathy. Whereas restricted diffusion on MRI representative of cytotoxic edema resolves within 1–4 weeks of ischemic stroke,
20 our last case demonstrated diffusion restriction 30 days postoverdose. Marked diffusion restriction 25 days postoverdose has been reported in a patient with leukoencephalopathy secondary to IV heroin overdose.
12 In that case, although no biopsy was performed, the authors used the term “spongiform leukoencephalopathy”; however, MRI features were consistent with hypoxic-ischemic leukoencephalopathy. Prolonged diffusion restriction, with an apparent diffusion coefficient nadir of 45 days, occurs in carbon monoxide associated delayed hypoxic leukoencephalopathy.
2,
21,
22 We suggest that, as is the case with diffusion restriction seen in metachromatic leukodystrophy,
23 diffusion restriction in posthypoxic encephalopathy reflects defective formation of myelin (dysmyelination).
Our cases further delineate distinct characteristics of delayed hypoxic leukoencephalopathy regardless of initial cause of cerebral hypo-oxygenation, and a prognosis for incomplete recovery with lasting cognitive deficits.
6,
7,
9 We found myelin basic protein, an essential protein constituent of myelin, to be markedly elevated in both delayed hypoxic leukoencephalopathy cases that were tested. Myelin basic protein serves as a CSF marker of acute widespread CNS demyelination. When delayed onset of mental status change follows a known or suspected hypoxic event, myelin basic protein greater than 40 ng/ml and an MRI showing diffuse hemispheric demyelination sparing subcortical u-fibers and posterior fossa may be useful in the diagnosis of delayed hypoxic leukoencephalopathy.