Just anticipating that a medication will bring pain relief can trigger the brain's endorphin system, dispatching endogenous opioids to specific pain centers in the brain. The intensity of pain reduction, both sensory and affective, is measurable and gradual, and is not an on-off phenomenon.
These findings were reported by a research team headed by Jon-Kar Zubieta, M.D., Ph.D., an associate professor of psychiatry and radiology at the University of Michigan Medical School and an associate research scientist at the school's Molecular and Behavioral Sciences Institute. The group has spent several years developing brain-imaging techniques that keep tabs on the brain's natural painkillers in action. Currently their work is focused on the function of the μ-opioid system, one of the principal systems involved in the modulation of pain, stress responses, and stress-induced analgesia.
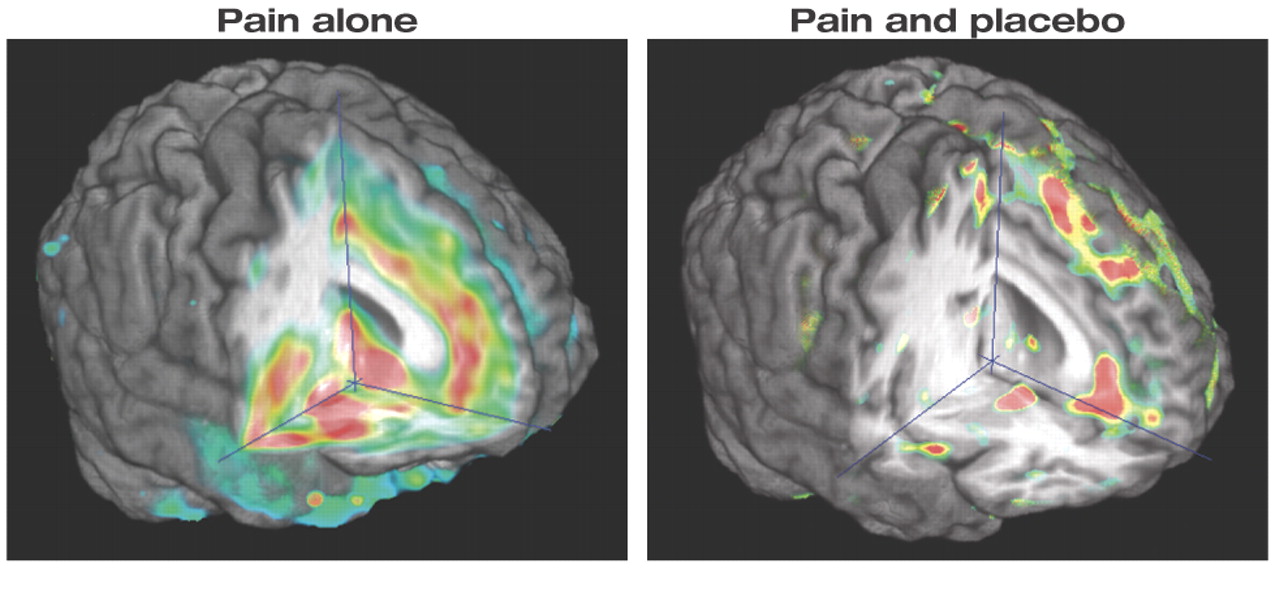
The brain at left shows areas of a subject's brain that were activated while experiencing pain. The brain at right shows areas activated after the subject was given a placebo while experiencing pain.
University of Michigan
In the μ-opioid system endogenous opioids, or endorphins, dock at pain-receptor sites on the surface of brain cells to block impulse transmission between cells.
The latest report of the team's work, which appeared in the August 24 Journal of Neuroscience, is believed to present the first direct evidence that endorphins are closely associated with the placebo effect.
“This deals another serious blow to the idea that the placebo is a purely psychological, not a physical, phenomenon,” Zubieta said.“ We were able to see that the endorphin system was activated in pain-related areas of the brain, and that activity increased when [subjects were] told they were receiving a medicine to ease their pain. They then reported feeling less pain. The mind-body connection is quite clear.”
The Michigan group used positron emission tomography (PET) to follow the response of the μ-opioid system and relate its function to subjective reports from 14 young male volunteers during a sustained pain challenge.
Subjects Injected for Pain, Placebo
Before being scanned, subjects were injected with radioactively tagged carfentanil, a molecule that binds only to μ-opioid receptors and releases positrons. Since carfentanil competes with the brain's natural endogenous opioid painkillers for space on nerve-cell receptors, PET scans reveal the activity level of the opioid system and μ-opioid receptors. Magnetic resonance imaging (MRI) scans of the subjects' brains were cross-registered with PET scans to give accurate information on exactly which brain regions were active during the experiment.
In a blind, randomized, and counter-balanced-designed trial, all subjects received two injections: one with salt solution, the other a placebo. During one scan they were told they would receive a medicine, which was actually a small amount of hydrating solution, that might relieve pain. The pain challenge consisted of 1.5 ml of 5 percent hypertonic saline injected into the relaxed masseter muscle for 40 minutes, long enough to establish the brain conditions and emotions closely related to those seen with chronic pain conditions like temperomandibular joint disorder.
While being scanned, every 15 seconds subjects rated the intensity of their pain sensations on a scale of 0 to 100 on a computer system. The same computer system controlled the intensity of the pain stimulus so that each subject's rating would be about the same throughout the experiment. This allowed the researchers to compare the response of the brain's antipain system across individual subjects and correlate the subjects' ratings with their PET scans.
As the researchers alerted the subjects that the placebo was coming and injected it, the additional volume of concentrated saline needed to maintain their pain over time increased, indicating a reduction in pain sensitivity of which the subjects were not aware. Merely imagining they were getting an analgesic helped the young men tolerate even more pain-inducing saline than before.
Opioids Migrate to Pain Centers
There were significant differences between the subjects' ratings after the scan during which they received the placebo and after the scan during which they received the saline injection alone. Nine subjects were classified as“ high placebo responders” because they had more than a 20 percent difference between pain and placebo scans in their average pain ratings per volume of saline infused. The other five were classified as “low placebo responders.”
“These subjective ratings are consistent with previous findings,” Zubieta said, “but the simultaneous imaging of the subjects' endogenous pain-reducing opioid systems sheds new light on why the placebo effect occurs.”
The results showed that opioids migrated to specific pain centers in the brain. All of the subjects had an increase in the activation of theirμ -opioid endorphin system after they were told that the“ medicine” was coming and the placebo was given. The most pronounced differences were seen in four areas of the brain known to be involved in complex responses to, and processing of, pain: the left dorsolateral prefrontal cortex, the pregenual rostral right anterior cingulate, the right anterior insular cortex, and the left nucleus accumbens.
When the researchers correlated the μ-opioid activity changes with the subjects' own ratings of their pain and emotions, they also observed that the placebo-induced activation of the opioid system was correlated with various elements of the experience of pain. For example, activity in the dorsolateral prefrontal cortex was associated with the expectation of pain relief reported by the subjects. In other areas, that activation was associated with relief of the intensity of pain, how unpleasant it was, or even how the individuals felt emotionally during the pain experience.
Because the study involved only healthy men between the ages of 20 and 30, further research is needed to determine whether the effect occurs in women and in people with various illnesses. In addition, the study only addressed the functions of the μ-opioid system, leaving open the question whether other opioid receptor neurotransmitter mechanisms may also be involved in the placebo response.
Psychiatric News asked Zubieta whether some people respond better to placebos simply because they believe in promised pain relief more than others.
“Not really,” he said. “Subsequent analyses have shown that expectations were not as important as the experience of pain itself—creating a `need' for a placebo effect.” A paper on this aspect of the study has been accepted for publication.
The study was supported by the National Institutes of Health.
An abstract of “Placebo Effects Mediated by Endogenous Opioid Activity on μ-Opioid Receptors” is posted at<www.jneurosci.org/cgi/content/abstract/25/34/7754?>. More information about pain and the μ-opioid system is posted at<www.med.umich.edu/opm/newspage/2003/paingene.htm>.▪
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.