Astudy in press with Drug and Alcohol Dependence provides what may be the clearest picture yet of Americans with alcohol dependence.
The study analyzed the clinical features of 1,484 Americans found to be alcohol-dependent t hrough the 2001-2002 National Epidemiological Survey on Alcohol and Related Conditions and then grouped those persons according to their clinical features.
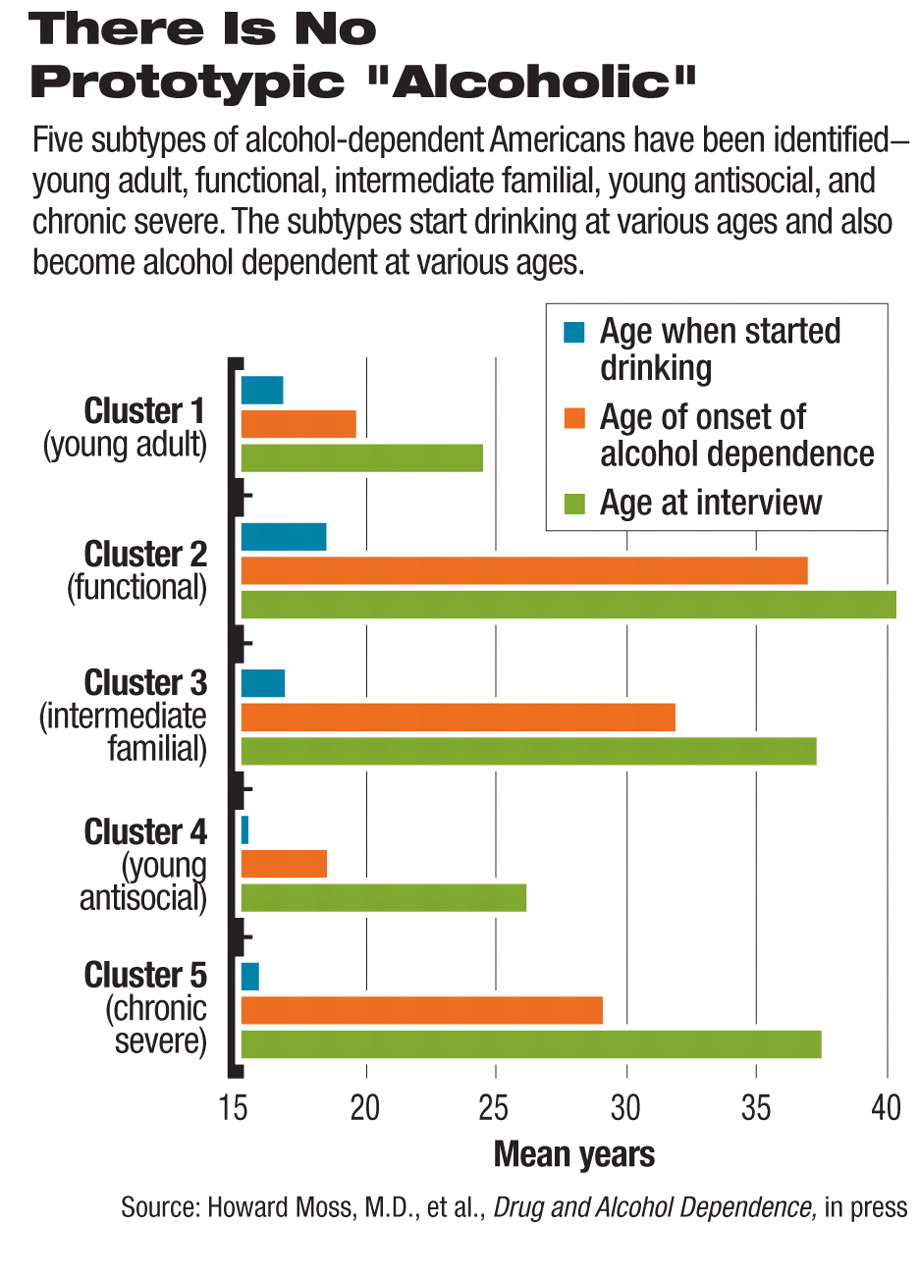
The study found that there is no such thing as a “typical alcoholic,” rather that alcohol-dependent subjects tend to fall into five subtypes—young adult, young antisocial, intermediate familial, functional, and chronic severe.
•
Young adult subtype. This is the most common alcohol-dependent subtype, constituting 32 percent of alcohol-dependent Americans. They are typically young, male adult drinkers with relatively low rates of co-occurring substance abuse and other mental disorders. They have a 22 percent rate of familial alcoholism and rarely seek help for their drinking.
•
Young antisocial subtype. This is the second most common category of alcohol-dependent individuals, constituting 21 percent of alcohol-dependent Americans. They are apt to be in their mid-20s and to have started drinking early. About half come from families with alcoholism, and about half have a diagnosis of antisocial personality disorder. Three-fourths of these individuals smoke cigarettes; two-thirds meet criteria for marijuana abuse or dependence. About a fourth use cocaine, and about a fifth abuse opioids. About one-third seek treatment for their drinking problem.
•
Intermediate familial subtype. Nineteen percent of alcohol-dependent Americans fall into this category. They tend to be middle-aged, with about half coming from families in which a member has alcoholism. Almost half have experienced a major depression, and almost a quarter have been diagnosed with bipolar disorder. About one-fifth abuse marijuana or cocaine. One quarter of these people seek treatment for their drinking problem.
•
Functional subtype. Nineteen percent of alcohol-dependent Americans fall into this category. They are, on average, older than other subtype members and tend to drink in an excessive, although less severe, manner than other subtypes. They have the highest family income, are college-educated, and are most likely to be married. They also include the highest proportion of retired individuals. From a psychosocial perspective, they represent the highest functioning subtype of alcohol-dependent persons. Nonetheless, they may still ultimately be at significant risk of the biomedical consequences of alcohol dependence. Seventeen percent seek treatment for their drinking problem.
•
Chronic severe subtype. This is the smallest category of alcohol-dependent Americans, constituting 9 percent of them. The subtype is composed mostly of middle-aged persons who had early onset of drinking. Over three-fourths come from families afflicted with alcoholism. This subtype has the highest probability of all the subtypes of having both first- and second-degree family members with alcohol dependence. Almost half have antisocial personality disorder. Of all the subtypes, they have the highest rate of major depression, social phobia, and bipolar, anxiety, and panic disorders. Over three-fourths smoke cigarettes. They often abuse substances in addition to alcohol. Two-thirds seek help for their drinking. They are the largest subgroup who seek treatment.
Unexpected Results Found
In an interview with Psychiatric News, lead researcher Howard Moss, M.D., associate director for clinical and translational research at the National Institute on Alcohol Abuse and Alcoholism, said the study's findings were unexpected.
“We were surprised that so many of the individuals who met diagnostic criteria for alcohol dependence were young adults. We thought we were going to see a substantial proportion of folks with alcohol dependence being of the chronic recurring subtype that is seen in Veterans Administration hospitals and in other kinds of settings where people treat chronic disease. Another surprise was the breakout in terms of family history of alcohol problems and the fact that only about half the sample had familial transmission of alcohol dependence.”
The study results suggest that certain therapies might work better with certain subtypes than with others, Moss said. In fact, he and his coworkers will now be attempting to see whether certain types of therapies work best for this or that subtype. Until such results are obtained, how should individuals in the various categories be treated?
Treatment Choices Vary
“The young adult variety may be addressed with screening and brief intervention techniques rather than much more expensive approaches to therapeutic intervention,” Moss advised. “It may also be—and again this is speculation, as we have to do the studies—that certain types of pharmacotherapies that are now available could be better targeted to this subgroup. For example, this subgroup might benefit from pharmacotherapy that reduces the reinforcing effect of alcohol.”
Since the antisocial group has the worst prognosis of any of the subtypes, Moss said, “the focus there has to be on complete abstinence and elimination of other forms of substance abuse and also mainstreaming their behaviors so that they are much more like the rest of society.”
“The functional subtype,” Moss emphasized, “represents individuals who essentially have fewer psychosocial consequences from their alcohol dependence. So the focus of the therapy there needs to be on recognition of the impairment that their alcohol dependence is producing in their life and also focusing on either abstinence or a return to a much less hazardous level of drinking.”
As for individuals with chronic severe alcohol dependence, “We would certainly assume that they are going to need substantial treatment,” said Moss. “They might benefit from therapies that are directed toward relapse prevention.” Furthermore, this group is going to have substantial psychiatric comorbidity, he pointed out, “so we have to simultaneously address their alcoholuse disorder as well as manage their psychopathology.”
Charles O'Brien, M.D., Ph.D., a professor of psychiatry at the University of Pennsylvania, who was unaffiliated with the study, told Psychiatric News that this study marks an important step in subcategorizing alcoholism because it includes a community sample rather than simply examining the 25 percent who present for treatment; it is based on a large dataset, and the five subtypes seem quite recognizable based on the data used: family history, age of onset, and presence of other psychiatric disorders.
“The next step,” he said, “[is to identify] biomarkers for even more precise subcategories, such as genotype or biochemical test.”
An abstract of “Subtypes of Alcohol Dependence in a Nationally Representative Sample” can be accessed at<www.sciencedirect.com/science/journal/03768716> by clicking on “Articles in Press.” ▪