The treatment of depression has changed dramatically over the past two decades. Since 1987, when fluoxetine was approved for marketing in the United States, the total number of prescriptions for selective serotonin reuptake inhibitors (SSRIs) and other new antidepressants has grown rapidly to more than 140 million prescriptions annually, second only to codeine-containing compounds (
1 ). Expenditures for antidepressants have increased by more than 450 percent over this time (
2 ), and the impact and pace of this change continue with the introduction of new antidepressants (
3 ). Accompanying this increased use of antidepressants are new forms of effective brief psychotherapy and an increase in primary care physicians' awareness of depressive disorders and comfort with treating depressed patients (
4 ). Together, these changes have provided more options for persons with depressive disorders to find effective treatment.
Despite improvements in available treatments, patients with depression often remain untreated or inappropriately treated, especially in primary care practices where most patients are seen. Fewer than half of patients who meet criteria for probable depression receive any form of depression treatment (
5 ), and only about one-fourth receive treatment consistent with current quality standards (
5,
6 ). In contrast to the quality of care for general medical disorders, the quality of depression treatment as assessed by the Health Employer Data Information Set (HEDIS) measures has not improved over time (
7,
8 ). In response to the continuing burden and poor quality of treatment, the Institute of Medicine has made treatment for depressive disorders one of five national priorities for quality improvement (
9 ).
Conceptual framework
More than a decade ago, the depression guideline panel of the Agency for Health Care Policy and Research (AHCPR) (now the Agency for Healthcare Research and Quality) and the American Psychiatric Association (APA) produced extraordinary clinical practice guidelines that identified the fundamental decisions that must be made during the course of treating a patient with major depression (
11,
12 ). A patient must recognize the presence of a significant emotional problem and bring it to the attention of a health care provider. Whether the patient has recognized the problem or not, the clinician must correctly diagnose the problem and initiate appropriate treatment. The patient must fill a prescription and take the medication for a sufficient time, at least four to six weeks, to allow for a clinical response. With complete resolution of symptoms, most patients should continue medication treatment for four to nine months to sustain remission, and many patients at high risk of recurrence should continue maintenance treatment for two or more years. If complete remission is not achieved, a change in treatment, such as dosage titration, switching to an alternative antidepressant or to psychotherapy, or augmenting treatment, is recommended.
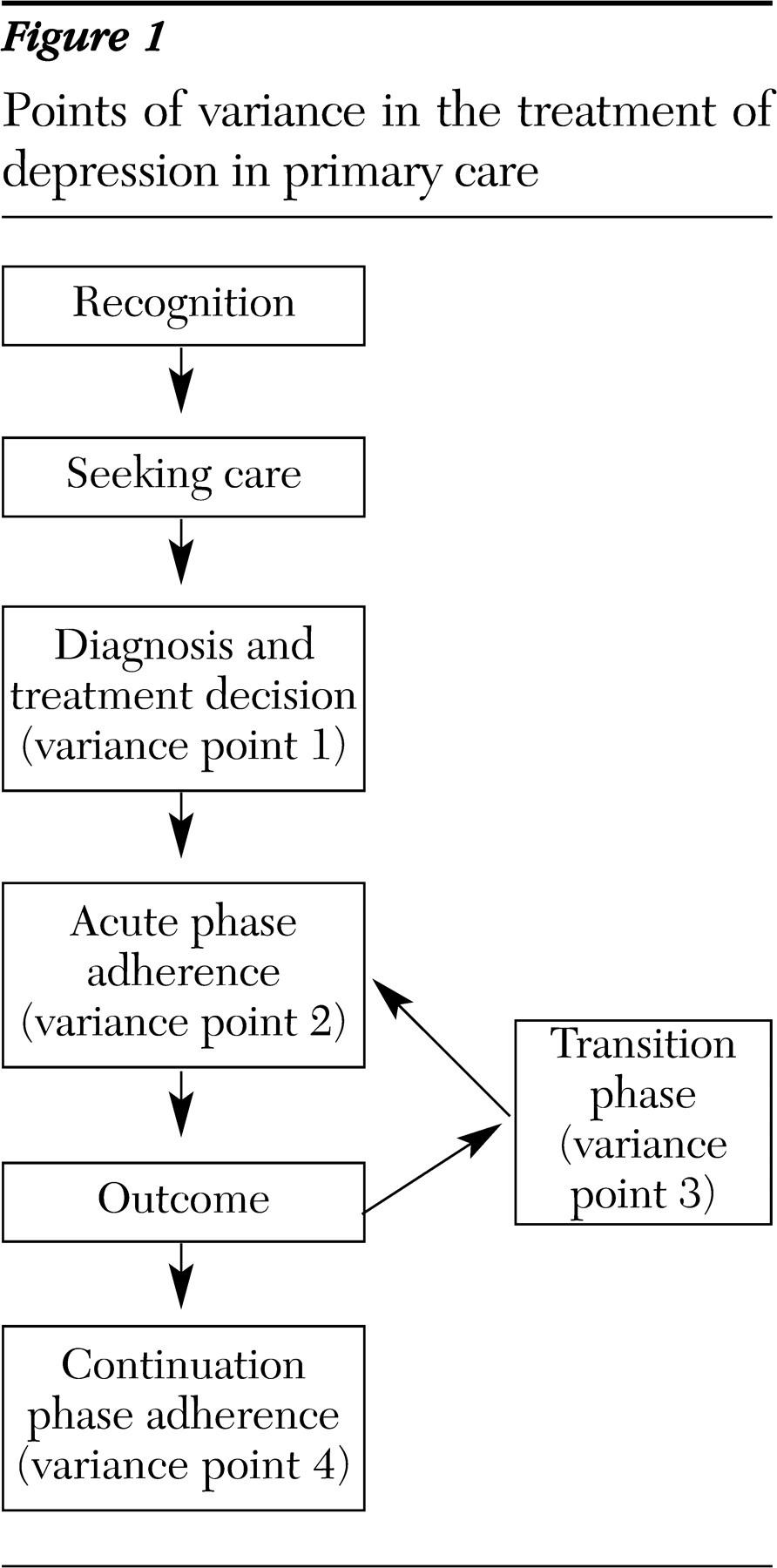
Subsequent evidence reviews and guidelines have confirmed the validity and continuing relevance of the AHCPR and APA guidelines (
13,
14 ). We have used these guidelines to create a conceptual framework, shown in
Figure 1, that includes four points of variance in the process of antidepressant treatment. Each variance point represents a distinct step in the process of treatment, and each represents a phase when care could deviate from expert guidelines. The decisions that take place at each step occur in the context of the patient's past experience, the patient-physician relationship, friends and family, and the broader social milieu. These factors may explain why even the best clinical care does not result in adherence to recommended lengths of treatment in all cases.
The first hypothesized variance point in our framework is the apparent failure to recognize, diagnose, or treat a depressed patient. Most research has focused on failure to provide treatment to those who are depressed, but very little is known about the diagnosis of patients at the time when antidepressant treatment is initiated. The lack of this diagnostic information raises concern for policy makers and purchasers of health care who believe, as we discuss in more detail, that much or most antidepressant use is unnecessary. Any conceptualization of the quality of treatment for depression should recognize the possibility that both failure to provide necessary care and the provision of unnecessary care with antidepressants can coexist.
Variance points 2, 3, and 4 in our conceptual model decompose the treatment episode. As in the depression model proposed by Kupfer (
15 ), the acute phase follows immediately after the initiation of treatment and continues for four to 12 weeks. If symptoms have not resolved by this time (an "outcome" in
Figure 1 ), the process of care then enters a transition phase, when decisions regarding the course of treatment must be made. After this transition, a new acute phase of treatment begins. Once complete symptom resolution is achieved, the patient enters the continuation phase of treatment. Approximately half of patients discontinue treatment during the first one to three months of treatment (variance point 2). Of those who do complete four to 12 weeks of treatment, many will not have complete symptom resolution and will not receive any necessary adjustments to treatment (variance point 3). Finally, we include adherence to treatment during the continuation and maintenance phases as the final, fourth, variance point.
Variance point 1: diagnosis and initial treatment decision
Variation in the quality of the initial clinical assessment and treatment decision contributes to the observed low quality of antidepressant care. Although the number of depressed persons who do not receive treatment has declined by one-third, many patients with depressive disorders still go untreated (
5,
6 ). Because most people identified as depressed in national surveys report having seen a physician at some time during a depressive episode, considerable research has focused on developing primary care-based strategies to increase the number of depressed patients who receive any depression-specific care. These strategies include patient screening in primary care (
16 ), feedback of screening results to patients and providers (
17,
18,
19 ), promotion of referrals to mental health specialty care, and dissemination of treatment guidelines and other forms of provider education. Overall, these various approaches have not been found to reduce the number of patients who go untreated or to improve patient outcomes relative to usual care (
17,
20,
21,
22 ). Community-based approaches to recognition, including hosting activities such as National Depression Screening Day (
23 ) in community venues such as churches, schools (
24 ), and workplaces (
25 ), have drawn attention as novel ways to encourage awareness and treatment of depressed people.
Although conventional wisdom maintains that the gap between the need for treatment and receiving it is largely due to the failure of physicians to recognize a mental disorder, alternative explanations are also possible. For example, the finding that sending depression-screening results to physicians does not significantly increase the likelihood of treatment suggests the existence of barriers beyond recognition, including preferences for alternative treatments (
26,
27 ). First-person accounts emphasize the ambivalence of many when initiating antidepressant treatment. For example, several authors have stated that depression is important to their experience of the world and fear that antidepressants will take away aspects of that experience and thus weaken their writing (
28 ). This literature also points to factors that influence patients to accept treatment, especially acquaintances and friends (
29 ). Qualitative research is needed to better understand the decision to go untreated that many people apparently make.
Although many depressed people are not treated specifically for depression, many policy makers and purchasers of health care believe that much of the care that is currently delivered, especially antidepressant care, is unnecessary or inappropriate (
30,
31 ). This opinion is based on several lines of circumstantial but influential evidence. First, the number of prescriptions written for SSRIs and other new antidepressants—more than 140 million in 2003, including both 30- and 90-day prescriptions (
1 )—represents enough days of therapy to treat each of the estimated 13.5 million Americans with a depressive disorder for more than a year, yet the rate of untreated depressive disorders has declined by only one-third over the past decade (
6 ). Second, analysis of pharmacy and medical insurance claims has shown that as little as 20 percent of recipients of antidepressants have a depressive disorder listed as a diagnosis (
32 ). Finally, analysis of pharmacy records suggests that many antidepressant recipients fill only one or two 30-day prescriptions, a level of treatment that is not expected to provide significant clinical benefit and is thus considered wasteful by purchasers of care (
31 ). In view of this evidence, rising expenditures for antidepressants have become both a prime target for those interested in cost containment and a barrier to adoption of quality improvement initiatives (
33 ).
There is now growing evidence that these purchaser beliefs may be correct. The World Mental Health Survey Consortium found that more than 8 percent of those receiving mental health treatment in the United States do not meet criteria for a mental disorder (
34 ), with the implication that more than one-third of all mental health care may be unnecessary. Physicians have reported prescribing antidepressants for mostly "appropriate" reasons (
35 ), but misdiagnosis of major depression may be a significant problem among those treated in primary care. Perez-Stable and colleagues (
36 ), Tiemens and colleagues (
37 ), and Klinkman and colleagues (
38 ) all reported that more than half of medical outpatients diagnosed as having depression by a primary care provider do not meet criteria for major depression as assessed by structured interviews.
There are now several published studies that directly assess the diagnosis of those in treatment. In a recent study of care management, Dietrich and colleagues (
39 ) found that one-third of those referred to the study had few or no symptoms. Bouhassira and colleagues (
40 ) found that only 65 percent of fluoxetine users, and fewer recipients of tricyclic antidepressants, met criteria for at least one of ten mental disorders on the
International Classification of Diseases (tenth revision) when responding in the Mini-International Neuropsychiatric Interview. Katon and colleagues (
41 ) reported that 63 percent of antidepressant recipients in a sample of patients treated in primary care met criteria for major depressive disorder in the prior two-year period, although this study did not report the prevalence of current disorder and used a single assessment six to eight weeks after the initiation of treatment.
Antidepressants may be appropriately used to treat disorders other than depression—anxiety disorders, for example—and such alternative uses could account for much of the overall use of antidepressants. Several studies have found that many patients taking antidepressant medication have symptoms of a mental disorder, even though they do not meet criteria for major depressive disorder (
36,
37,
38 40,
42 ). Evidence from clinical trials supports the use of antidepressants to treat anxiety, and some SSRIs are approved for this use (
43 ). Using antidepressants to treat minor depression remains controversial and could indicate unnecessary use (
44,
45 ), despite one recent trial suggesting efficacy (
46 ). Moreover, the long-term outcomes of complex situations, such as a patient with a history of major depression and current depressive symptoms or adjustment disorder, have not been studied, but many physicians may consider these situations to be appropriate for treatment with an antidepressant in order to prevent recurrence of major depression. Even more complex situations often arise in primary care, where some experts recommend a therapeutic trial of antidepressants for patients with unexplained symptoms, such as unusual levels of fatigue after a myocardial infarction (
47 ).
The costs of potentially unnecessary treatment include financial costs, possible side effects, and missed opportunities for effective care. Research that identifies the reasons for antidepressant treatment—the influence of consumer-directed advertising, for example—would provide critical direction for future quality improvement initiatives. Understanding the magnitude of use for specific conditions—for example, minor depression or symptom complexes such as fibromyalgia or myocardial infarction aftercare—would guide priorities for efficacy trials. Finding large amounts of unnecessary care would motivate evaluation of quality improvement strategies, such as utilization review, that would limit such care and save considerable sums of money that could be used more constructively elsewhere. Such a finding would also have significant implications for quality measurement. If the initial treatment is unnecessary, continuing treatment for six months should not be considered high-quality care, as is the case with some current measurement protocols such as the HEDIS.
Variance point 2: adherence during the acute phase of treatment
Efforts to improve the length and quantity of treatment have been more successful than attempts to reduce the number of depressed patients who go untreated. More than ten large trials, in a wide range of settings, have demonstrated that care management for depression can increase the rate of effective treatment and improve patient outcomes compared with usual care (
39,
48,
49,
50 ). Furthermore, these interventions have been shown to be relatively cost effective (
51,
52 ), and they may save money if one considers the monetized value of apparent work-related benefits (
53 ). Unfortunately, many patients do not have access to practices that have implemented such quality improvement activities.
Although systems approaches such as care management appear to hold great promise, treatment adherence can remain less than optimal even when these systems are efficiently implemented (
33,
49,
54 ). This finding has prompted a great deal of research on other determinants of premature discontinuation. Sociodemographic characteristics that have been found to affect the likelihood of adherence include age (
55 ), gender (
56 ), income (
55 ), knowledge and attitudes about depression and treatment (
57,
58 ), and perceived stigma (
55 ). Physicians appear to place much of the blame for nonadherence to guidelines on noncompliant behavior among patients, such as lack of established routines, but studies have not researched this point in depth (
59,
60 ).
Whether operating through cognitive deficits, feelings of hopelessness, or other factors, depression itself directly affects the likelihood of adherence to treatment (
61 ). Disease characteristics that have been found to affect the likelihood of patients discontinuing treatment include the type and severity of depressive disorder (
6,
54,
59 ), the number and type of medical and mental comorbid disorders (
60 ), any current or past treatment (
62 ), and in extreme cases, whether the symptoms are disabling (
63 ). It is important to note that not all studies find a relationship between the severity of depression and the likelihood of discontinuing treatment (
41 ). In several European studies, between 35 and 55 percent of patients who prematurely discontinued antidepressants reported having done so because they "felt better" (
64,
65 ), and in one study, feeling better was confirmed by improvement in functioning (
63 ).
The combination of antidepressants and psychotherapy appears to be associated with reduced likelihood of dropout, but patients receiving combined treatment may have higher levels of psychiatric distress, which in itself may be associated with adherence to treatment (
54 ). The choice of an SSRI over a tricyclic antidepressant may result in better adherence; however, the choice among SSRIs does not appear to make a significant difference (
66 ).
Although most quality improvement initiatives are designed to work at the system level, little research has evaluated the characteristics of systems that are associated with quality of care. Physicians represent one critical component, and recent studies show that the quality and nature of the instructions and information given to patients by their physicians appear to be associated with the quality of care (
67,
68 ). The administration of medication by psychiatrists is associated with higher levels of adherence (
69 ), and certain physician or practice characteristics, including financial incentives, managed care, the relative percentage of public patients, and age of patients, are significantly associated with quality (
70,
71 ). Broader system characteristics may also influence the likelihood of discontinuing treatment, including the nature and type of formularies (
72 ) and drug utilization review, the nature of insurance benefits for mental health care (
55,
56 ), and geographic accessibility of care (
73 ). The precise reasons for systematic improvement associated with collaborative management have not been identified (
74 ).
Social and cultural factors that exist outside the system of care—including the nature of family, community, or workplace stigma (
75,
76,
77 ); patients' social support networks; and their pathways to care (
78 )—could also have a significant effect on premature discontinuation of treatment. A recent review of older literature suggests the importance of social disorganization and disadvantaged environments (
79 ). Differences in sociodemographic characteristics and other factors may indicate underlying social constructions of illness that further determine adherence to short- and long-term medication management (
80 ). Much work remains to be done in this area.
Care management models have addressed many of the patient, disease, treatment, and system factors that appear to influence adherence to acute treatment, and these models may have reached an optimum balance of cost and effectiveness based on currently available knowledge. Future improvements in the quality of care are most likely to be the result of extending beyond clinical and health services conceptualizations to include patient experiences and the context in which they occur (
81 ). Family support, crucial during the initial phases of treatment (
78 ), can be eroded by misconceptions and impaired interpersonal relationships. With most chronic diseases, families are actively included in treatment plans, but professional ethics regarding confidentiality and failure to make use of existing family interventions may prevent their inclusion from happening in the case of depression. Broader levels of community support also may be missing. The current "don't ask, don't tell" environment in most workplaces functions as a barrier to continued treatment (
82 ). Moreover, employer accommodation of depressed workers may accentuate perceptions of stigma when it appears that an employee is receiving "special treatment."
Themes from first-person accounts add detail to this clinical picture and suggest that further understanding of the experience of depression and its treatment could result in new strategies to improve adherence to treatment. For some patients, antidepressant treatment works well. As Jane Kenyon (
83 ) noted in her poem "Back," "Suddenly I fall into my life again." Most authors, however, relate the limitations of treatment that result in poor adherence both early and late in the course of treatment. For example, Karp (
84 ) noted the partial response that often occurs ("Although it diminished my symptoms, imipramine was not my ticket to normalcy") and that even this partial response may not last ("I tried still another medication—doxepin. I did this out of a sense of desperation. Shortly after swallowing the first pill, my anxiety noticeably decreased …, but the miracle was short-lived"). Others describe side effects that undoubtedly influence decisions about adherence to treatment. Twitchell (
85 ) described "searching through trial and error for a drug that would cure what ailed me with as few side effects as possible. Some of them make you dream, every night, the kind of dream you hate to wake from. Others keep you skittering along the surface of sleep."
For many, the ambivalence and changes in identity associated with initiating antidepressants continue through the course of treatment. For example, Solomon (
28 ) decided "not to go off my medications. I'm not sure that I'm addicted, but I am dependent: without the drugs I would run the risk of emerging symptoms of illness. It's a fine line. I have gained an unbecoming amount of weight. I get weird hives for no apparent reason. I sweat more. My memory, never very good, is mildly impaired."
Variance point 3: transition-phase treatment
Most patients in antidepressant clinical trials do not achieve complete symptom resolution, but research suggests that changes in treatment are made for few patients (
86,
87 ). Rather, most patients either discontinue treatment or continue on the same treatment, a finding that could also influence the measurement of quality. Studies that rely on assessments of pharmacy records could overstate current levels of quality by considering all those who remain on their initial treatment as having appropriate care even when remission status has not been assessed. Alternatively, many patients who discontinue antidepressants prematurely may substitute psychosocial for ineffective medication treatment, and these changes in treatment are not assessed in studies that rely solely on pharmacy records. Thus measures such as the HEDIS may understate or overstate the current state of quality, or these alternatives could coexist. In either case, further research on measurement of the quality of treatment for depression is needed.
Although clinical practice guidelines are clear that treatment should be modified when symptoms have not completely resolved (
11,
12 ), we know of no research that specifically addresses whether this transition-phase management routinely occurs. In our conceptual model, we view this management as a clinical activity responding to an unsatisfactory outcome, such as an intolerable side effect or an inadequate clinical response. In these cases, options include switching medications or adding a medication from the same or different classes. Switching to or combining medication treatment with psychotherapy also may be an appropriate response.
The Sequenced Alternatives to Relieve Depression trial (STAR*D) (
88 ) and other trials are exploring the most appropriate secondary strategies when depressive symptoms persist among patients with major depressive disorder, but no guidelines or studies provide guidance for physicians when depressive symptoms persist among patients with other disorders. However, patients with these latter conditions provide a third alternative explanation for the observed low rates of augmentation or switching among those who remain on antidepressant treatment for more than a month or two. A few studies suggest higher rates of remission among patients with subthreshold depression compared with those with major depression (
44,
89 ). In the community, many antidepressant users may have minor or subthreshold symptoms and may have higher response rates. These patients would not require changes in treatment, and of course some may not have needed treatment at all. Comparisons between initial symptom levels, outcome, and the need for changes in treatment will be necessary to guide future research and development of guidelines in this area.
Discussion
When viewed in the context of a national imperative for quality improvement, treatment of depressive disorders presents a complex challenge. The unmet need among depressed patients is considerable, but unnecessary treatment also may be considerable. Quality improvement programs are typically designed to increase levels of care and focus on patients with probable depression. At the same time, efforts to limit unnecessary care typically focus on cost containment rather than quality improvement, even though the mechanisms used to control costs may conflict with strategies to reduce unmet need. As we have described, many studies have provided valuable information regarding individual domains or factors that influence the trajectory of treatment. We know little, however, about how these factors fit together and influence one another. Failure to provide high-quality care for depression at all levels of the treatment system signals the difficulty of the task.
The conceptual framework we have outlined here builds on prior mental health services concepts and theory to provide a broad look at the current state of quality of treatment for depression and points toward steps to improve it. We offer four areas for future research and endeavor to improve the quality of treatment for depression. First, it is apparent that too many people with depression do not receive treatment. Attempts to improve recognition of major depressive disorder and treatment in primary care have not been successful for the most part. However, our review suggests that several new approaches, including extension of outreach and policy change in nonmedical settings such as schools and workplaces, where many Americans spend most of their nonsleeping hours (
90 ), could be worthwhile.
Second, although pharmaceutical marketing and other efforts to increase awareness and recognition have resulted in large increases in the amount of treatment provided, at least some of this treatment seems to be indiscriminate and not applied to people most in need (
91 ). We believe that it is important to understand whether this treatment is truly unnecessary or whether those who receive short-term antidepressant treatment for disorders other than those in the depression and anxiety spectrum actually benefit from that treatment. Understanding the magnitude of unnecessary care would at once identify an area for potential improvement in quality and indicate the magnitude of one source of bias in the current measures of quality. A third benefit of understanding the nature of the conditions for which treatments are commonly used would be to provide priorities for clinical trials to determine the potential benefits of these treatments.
By identifying the critical junctures where treatment can stray from an evidence-based course, the existing clinical and health services approach to the quality of treatment for depression offers continuing opportunities to improve care as it is currently delivered. However, this approach by itself fails to capture the complexity of how and why depressed individuals make decisions about treatment—information that is essential to understanding the course of that treatment. The self-concepts that underlie depression and decisions about treatment are also social constructions regarding identity, stigma, social and family relationships, and the value of "impaired life" (
92 )—constructs that are based on past experiences and interactions with those who make up one's social world. Thus, as a third step to improving the quality of treatment for depression, we believe that new theoretical insights and research strategies are needed to enable researchers to identify the intervening mechanisms between sociodemographic variables and specific behaviors related to accepting the need for antidepressant treatment and then adhering to it.
Finally, our review suggests the need to improve methods to measure the quality of antidepressant treatment. Current measures commonly used in both research and practice settings frequently rely on administrative data that may not accurately reflect diagnosis (
93 ). This error is compounded by measures that are based on notions of a fixed duration of treatment that do not recognize the need to extend treatment for those whose initial course of treatment fails, that count stable treatment as high quality in all cases even though most patients will require changes in treatment, and that count the discontinuation of medication as poor-quality treatment even though there are appropriate reasons for doing so, such as a patient's not being depressed in the first place or switching to cognitive psychotherapy.