Sample
The JCUSH was a telephone survey conducted between 2002 and 2003. It was sponsored by the U.S. National Center for Health Statistics and by Statistics Canada and is described in detail elsewhere (
16,
17 ). The survey sampled representative community-dwelling adults stratified by province in Canada and by four geographic regions in the United States. Institutionalized populations and persons living in Canadian or U.S. territories were excluded. To ensure a sufficient sample of older adults, individuals older than 65 years were oversampled.
Households were selected through random-digit dialing. In randomly selected households, a knowledgeable adult household member was asked to supply basic demographic information on all household residents. From these households, an adult household member was then randomly selected for an in-depth interview. In cases in which the selected individual was not capable of completing the interview, a knowledgeable member of the household served as a proxy by supplying information about the selected participant.
Overall, 3,099 individuals in Canada and 5,054 in the United States were interviewed. Response rates were 66 percent in Canada and 50 percent in the United States. Final study weights were computed to adjust for oversampling and to make the composition of samples representative of the household adult population of the two countries.
Assessments
Presence of a probable major depressive episode in the past 12 months and severity and duration of depressive episodes were ascertained by using the Composite International Diagnostic Interview-Short-Form (CIDI-SF) (
18 ). The CIDI-SF is a structured diagnostic interview designed for use by trained nonclinician interviewers that screens for
DSM-IV disorders (
19 ). CIDI-SF asks about eight symptoms of major depressive disorder in the past 12 months. Individuals who endorse five or more symptoms meet the
DSM-IV symptom criteria for a major depressive episode. Previous analyses have shown that individuals who endorse five or more CIDI-SF symptoms for a minimum duration of two weeks have an 89 percent probability of meeting full CIDI criteria for a major depressive episode (
20 ). This cut-off point was used in our study to define probable major depressive episode in the past 12 months (present, 1, or absent, 0). The number of symptoms endorsed was used as an indicator of severity of the depressive episode (range, five to eight).
Severe impairment in functioning as a result of mental health problems was assessed by asking the participants a series of questions about "difficulties" they may have in "doing certain activities because of a health problem." Health problem was defined as "any physical, mental, or emotional problem or illness." Difficulties listed included difficulties in physical activities, such as walking, using fingers to grasp or handle small objects, and carrying objects; difficulties with activities outside the house, such as shopping or participating in social activities; and difficulty in doing things to relax at home or for leisure. Participants who reported difficulties in at least three specific activities were asked which health problem from a list of 18, including "depression/anxiety/emotional problem," caused the difficulties. Severe impairment in functioning caused by mental health problems was defined as difficulties in at least three areas attributed to "depression/anxiety/emotional problem" (present, 1, or absent, 0).
Sociodemographic characteristics included gender (female, 1, or male, 0), age (18 to 44 years, 45 to 64 years, and 65 years or older), race or ethnicity (minority, 1, or Caucasian, 0), marital status (married or living as married, divorced or separated, widowed, or never married), education (less than high school, high school or equivalent, vocational school or community college, or associate degree or higher), and household income adjusted for the number of persons residing in the household (
17 ). Participants were assigned to income quintiles by ranking according to the adjusted household income within each country; possible scores ranged from 1 to 5, with higher scores indicating higher income.
Health insurance was assessed only among U.S. participants because all Canadians are covered by the Canadian universal insurance plan. U.S. participants were categorized into those with health insurance coverage throughout the past year, those with insurance coverage for only part of the past year, and those without insurance coverage throughout the past year.
Regular medical doctor was ascertained by asking participants if they had a regular medical doctor (yes, 1, or no, 0).
Chronic medical conditions were ascertained by asking participants if they had asthma, arthritis, hypertension, emphysema, diabetes mellitus, heart disease, coronary heart disease, or angina, or if they had had a heart attack. Participants were asked if they had ever been told "by a doctor or other health professional" that they had each condition and whether they still had that condition. Participants who reported currently having any of these conditions were rated as having a chronic medical condition (present, 1, or absent, 0).
General health was rated on a 5-point Likert scale. Possible scores range from 0, poor, to 4, excellent.
Mental health treatment seeking was assessed with one question: "In the past 12 months have you seen or talked on the telephone to a health professional about your emotional or mental health?" Participants who reported having seen or talked to a health professional were asked about the number of such contacts and whether the contact was with a family doctor or general practitioner, psychiatrist, psychologist, nurse, social worker or counselor, or other professional. Contact with health professionals for mental health reasons was rated dichotomously as present, 1, or absent, 0. It should be noted that this definition of mental health treatment seeking is admittedly broad and does not necessarily correspond with receiving adequate mental health treatment or even any treatment. Participants were also asked if they had taken prescription medications for any condition in the past month (yes, 1, or no, 0). The type of medication or indication for use was not ascertained.
Perceived unmet need for mental health care was assessed by first asking the participants if during the past 12 months they ever felt that they needed health care but did not receive it. Participants who responded positively were then asked about the type of care that they felt they needed but did not receive. Participants who indicated that they had not received needed "treatment of an emotional or mental health problem" were rated as having perceived unmet need for mental health care (unmet need, 1, or no unmet need, 0).
Analyses
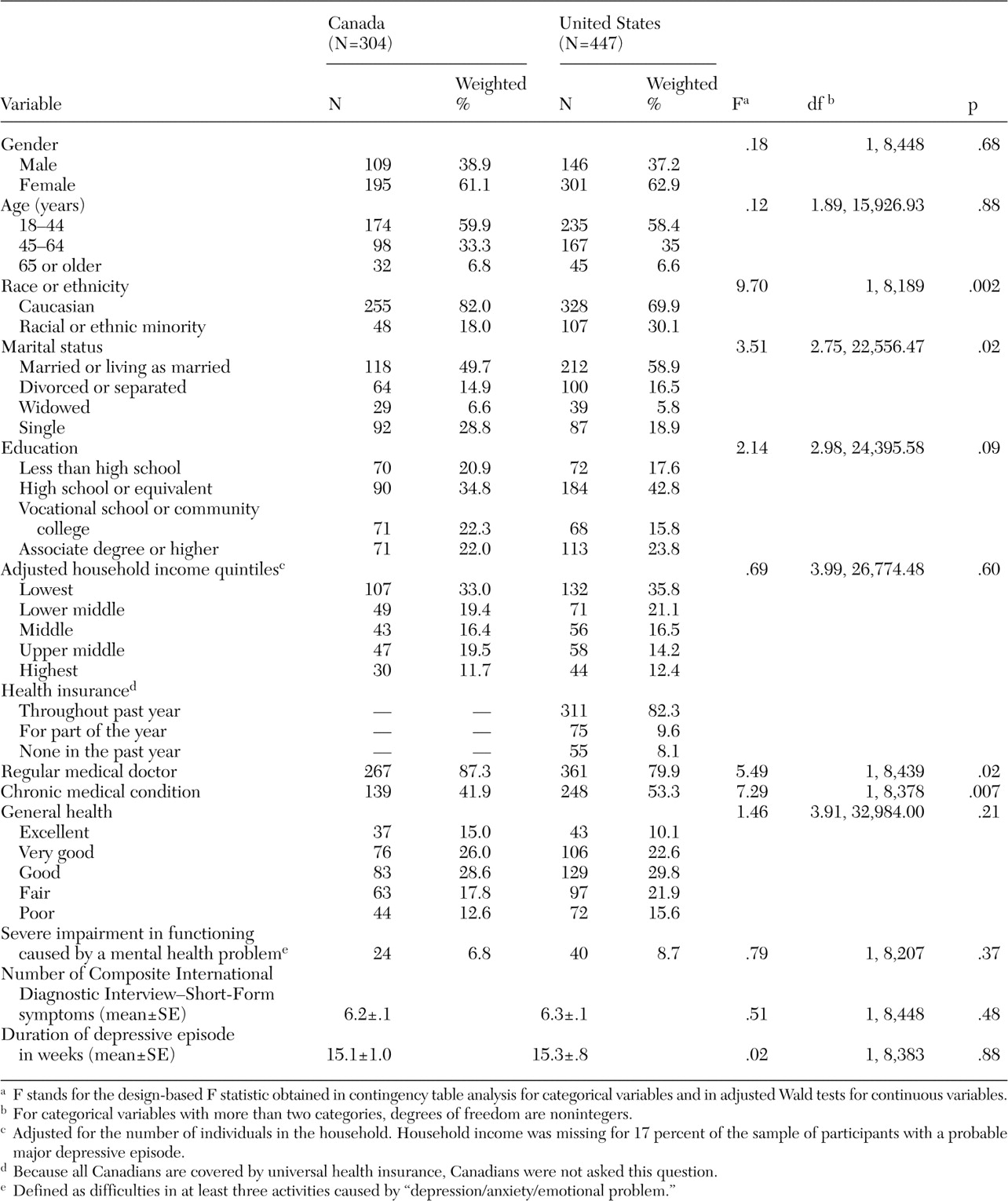
Analyses were conducted in four stages. First, as a preliminary step, the sociodemographic and clinical characteristics of participants with a probable major depressive episode in the two countries were compared by using contingency table analysis for categorical variables and the adjusted Wald test for continuous variables.
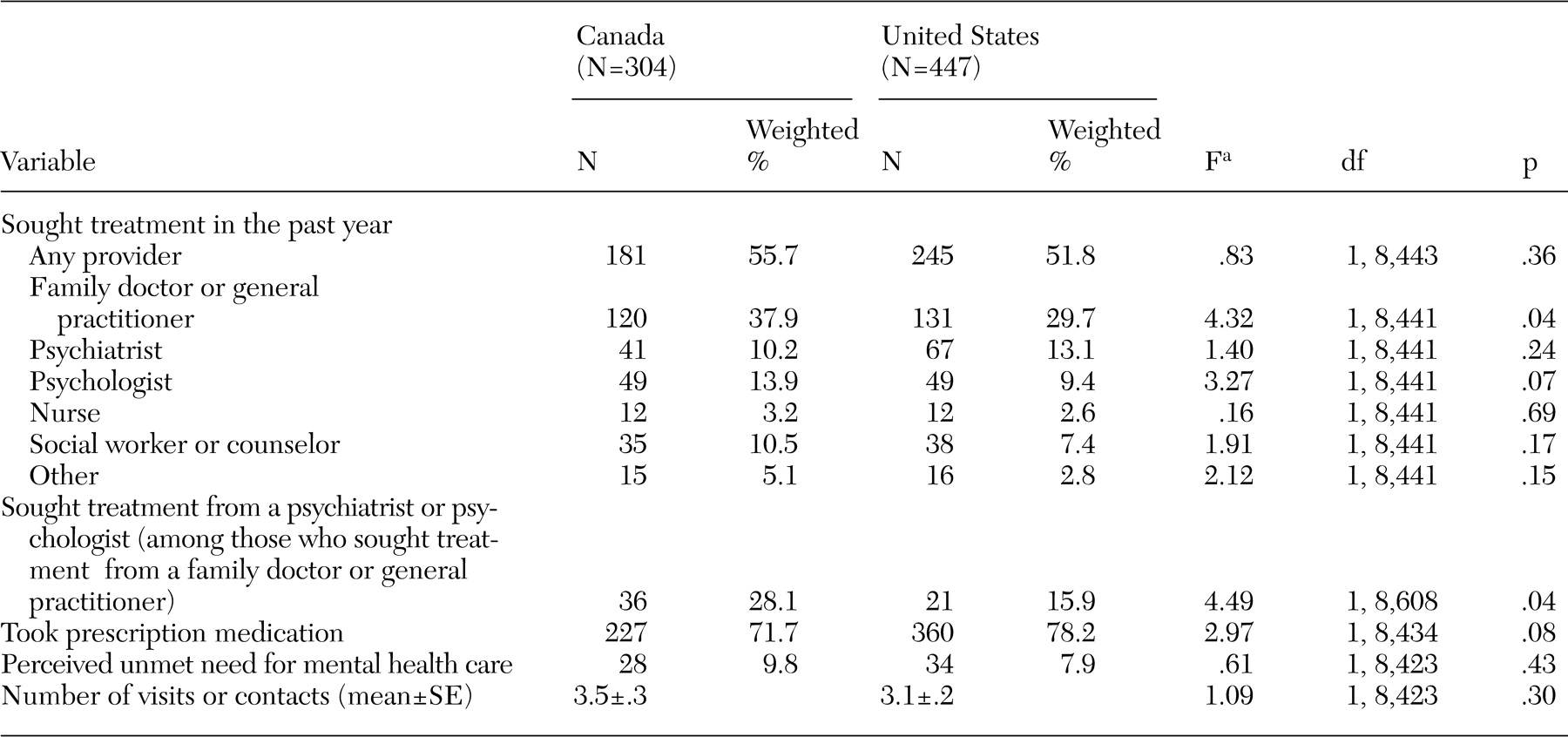
Second, participants in each country who had a probable major depressive episode were compared with respect to mental health treatment seeking from any provider, the type of provider, the use of prescription medications, perceived unmet need for mental health care, and number of mental health visits. Again, contingency table analysis and the adjusted Wald test were used for these analyses. The analyses were limited to participants with a probable major depressive episode. The analysis for comparing mental health treatment seeking from any provider across the countries was repeated in a multivariate logistic regression model, which adjusted for gender, age, race or ethnicity, marital status, education, household income, having a regular medical doctor, having a chronic medical condition, general health rating, severe impairment in functioning, number of CIDI-SF symptoms, and duration of depressive episode.
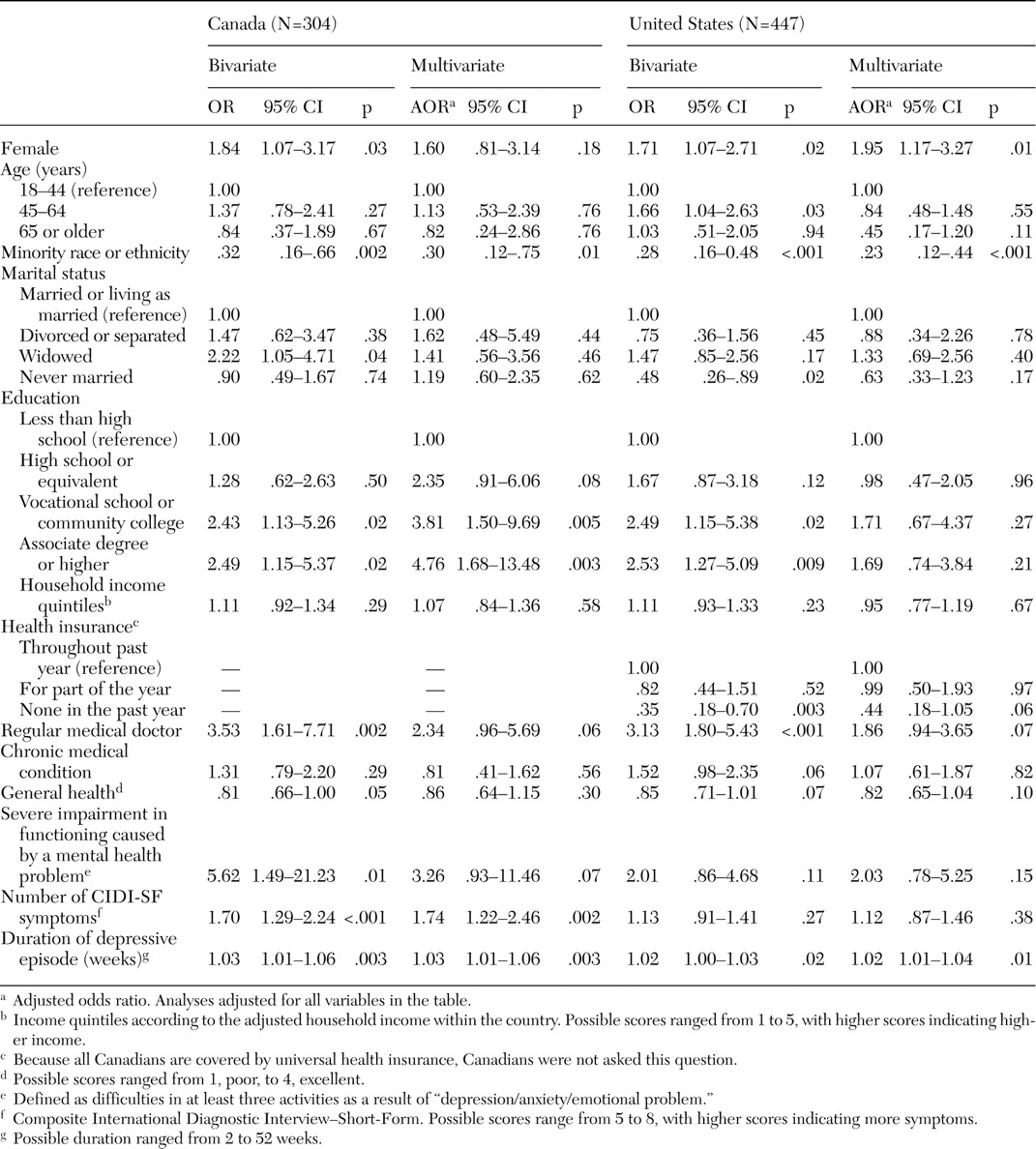
Third, the association of sociodemographic characteristics with mental health treatment seeking from any provider among participants with a probable major depressive episode was assessed separately in the two countries with bivariate and multivariate logistic regression models in which the dichotomous variable of treatment seeking was the dependent variable of interest and the sociodemographic characteristics of individuals were the independent variables of interest. Multivariate analyses produced odds ratios that were adjusted for all variables in the model described above. In addition, analyses for the U.S. sample adjusted for insurance status.
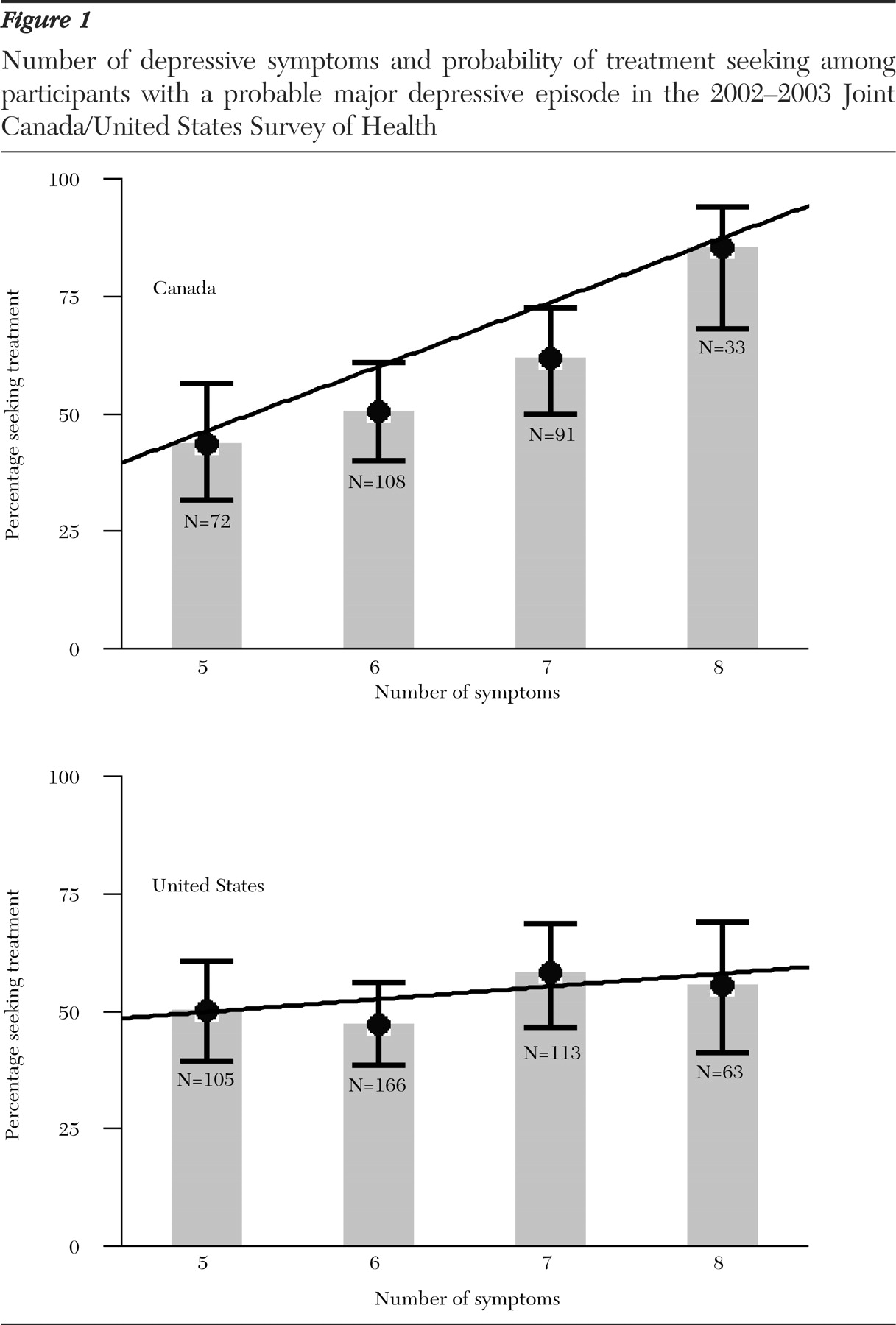
Fourth, to assess whether the findings were consistent across sociodemographic groups traditionally reported to have better access to health care, the analyses described in stage 3 for the association of the variables of number of depressive symptoms and mental health treatment seeking from any provider were repeated among participants in the upper three income quintiles, Caucasians, and U.S. participants with insurance coverage throughout the past year. Also, because some individuals continue education after the age of 18 years, the analyses of the relationship between education and mental health treatment seeking from any provider were repeated among participants with a probable major depressive episode who were older than 21 years.
Missing data were dealt with by using the method of dummy variable coding (
21 ) in which the missing values were replaced by the reference category on categorical variables (coded as 0) and the lowest values in the range on ordinal and continuous variables (for example, 1 for household income quintiles) and by entering a dummy variable for missing data (missing, 1, or not missing, 0) along with each variable in the logistic regression models of the third and fourth stages of the analysis described above. It should be noted, however, that data were missing for only a small number of cases, and adjusting the analyses for missing values had a minimal impact on the results of the analyses. For 12 of the 13 independent variables in regressions reported in
Table 3, fewer than 6 percent of the cases had missing values. The variable with the largest number of missing values was household income, with 17 percent of the cases having missing values on this variable.
Because the JCUSH used a complex stratified sampling design, the analyses were conducted by the "svy" routines of STATA 8.0 software (
22 ), which take into account the design elements of the survey, including survey weights, primary sampling units, and strata. For analysis of contingency tables based on complex survey data, STATA reports an F statistic (with noninteger degrees of freedom when the categories exceed two). This F statistic is computed from the usual Pearson chi square test by using a correction (
23 ) to account for the complex survey design. The p value for this F statistic can be interpreted in the same way as a p value for a Pearson chi square. The rationale and computation details for this F statistic have been described by Rao and Thomas (
23 ). Statistical testing for comparison of means on continuous variables is by adjusted Wald test, which also produces an F statistic (
24 ). Statistical testing of logistic regression coefficients is conducted by using t tests with degrees of freedom equal to the number of primary sampling units minus the number of strata (
25,
26 ). Technical description of these tests is beyond the scope of this paper and can be found elsewhere (
23,
24,
25,
26 ). All reported percentages are weighted. A p value of <.05 was considered statistically significant.