However, despite growing awareness of the need for mental health services in this population, it is generally acknowledged that homeless people continue to have inadequate access to these services (
9 ). Consequently, rates of mental health problems in this population have not declined and in fact may be increasing. We recently showed that in Montreal and Quebec City, 60% of people using resources for the homeless reported mental disorders at some point in their lifetime, and 72% of this group had experienced serious disorders within the past year (
10 ). However, 56% of the sample had not received any mental health services in the past year, despite having access to the Canadian health care system, which allows all residents free access to such services. In this study we sought to determine what factors predict the utilization of mental health services by homeless or impoverished people.
Homeless or impoverished people with mental disorders face numerous barriers to receiving appropriate health care. Some barriers come from service providers who are reluctant to treat this type of client (
11,
12 ). Other barriers come from the people themselves, who are distrustful about the providers and the authorities (
13 ). In a well-known study, Appleby and Desai (
14 ) showed that homeless people with mental illness had lower hospital admission rates than people who were domiciled and mentally ill, that they often left the hospital against medical advice, and that few were referred to long-term facilities.
Underlying these various barriers, it has long been assumed that lack of health care insurance (or lack of economic access to health care) is one of the most important factors influencing the utilization of mental health services by homeless or impoverished people. Homelessness among U.S. patients with serious mental illness has been associated with a lack of Medicaid insurance (
15,
16 ), and both Kushel and colleagues (
17 ) and Wenzel and colleagues (
18 ) reported that lack of health insurance for homeless people was associated with barriers to mental health care. Rosenheck and Lam (
19 ) also identified economic factors as an important barrier to mental health services.
As a result of this previous research, much energy and attention have been focused on addressing the mental health needs of this population from the viewpoint of economic access. But what if lack of health care insurance is not the only important barrier to service utilization?
Very little research has been devoted to understanding factors—independent of health insurance barriers—that are associated with the use of mental health services by people who are homeless or impoverished. Our study was conducted in the Canadian setting of universal access to health care, where the study population faced no financial barriers to obtaining mental health care services. Therefore, this analysis may offer a unique view of the situation.
To our knowledge, this is the first study to use Pescosolido's network episode model (
20,
21,
22,
23 ) for such an analysis. This model takes a broad view of the person with mental illness and his or her entry into the health care system. Pescosolido and colleagues (
23 ) explained that in psychiatry the individual does not always make health-related decisions alone and in a rational manner; the individual is often forced to enter the health care system after actions taken by police officers, judges, or family members. The network episode model proposes a "career" approach to the individual's mental illness, taking events into account in a dynamic manner, while respecting the sequences of those events and the multiple options available at any given point in time. Thus actions and decisions become interwoven in a social process that involves the individual within the network. Action strategies are consequently conceptualized as emerging from a rational process intrinsically linked to the social dimension (
21 ). The four basic concepts of the network episode model are sociodemographic characteristics, or the background that helps set the trajectory of the illness; illness characteristics, or the diagnoses; illness history, or the entrances and exits from the health care system based on diagnoses and remissions; and social network, or the size and function of the individual's social network and his or her satisfaction with this support. All of these elements are believed to interact dynamically to influence each other.
Discussion
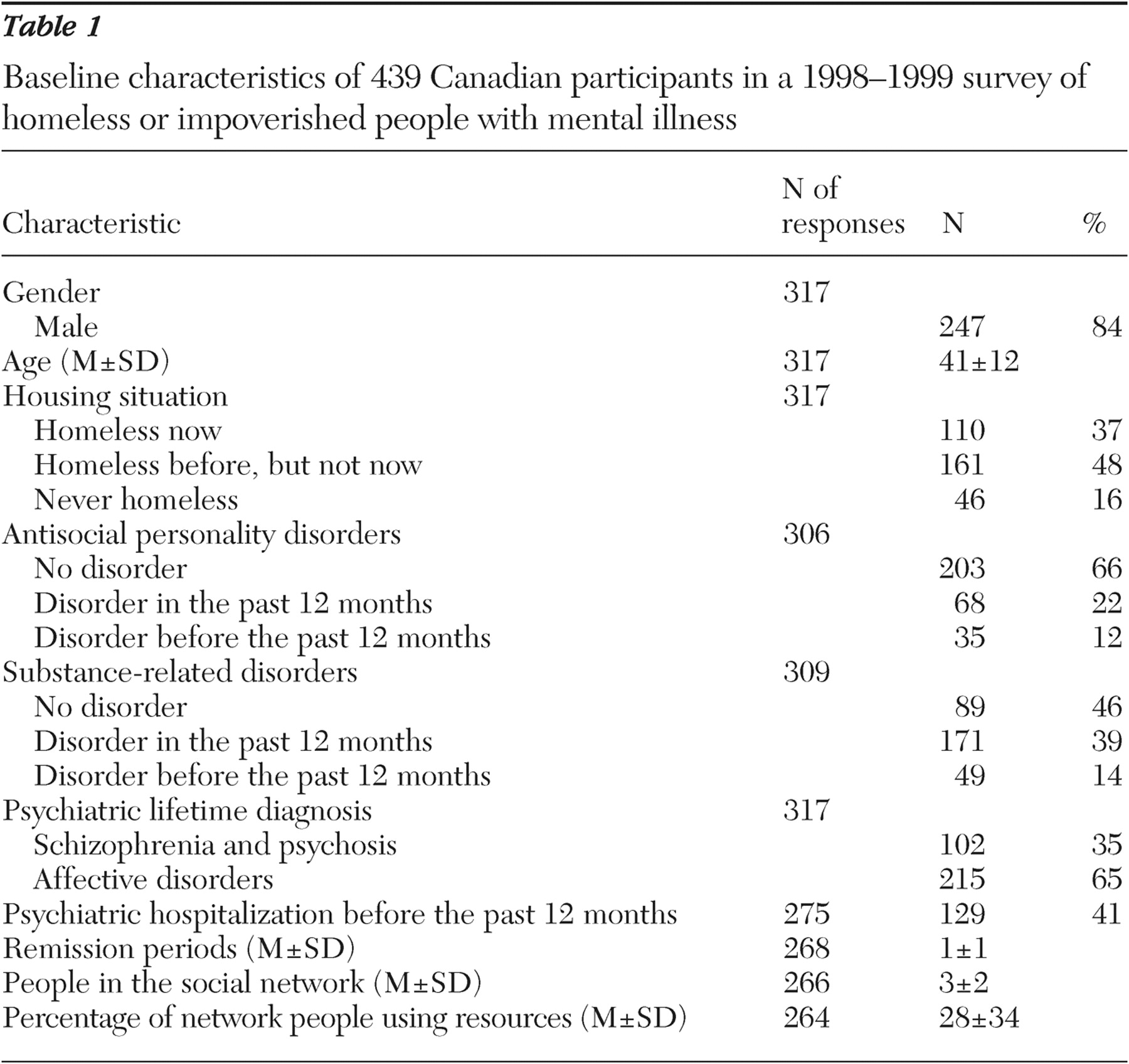
This study is one of the largest ever done in Canada. It used a rigorous sampling method based on a census in order to reach most of the population that uses resources for the homeless in Montreal and Quebec City.
By studying Canadians' use of mental health resources for homeless and impoverished people, in a country where access to health care is free to all citizens, we have confirmed that previously identified predictors of service utilization remain important. One may question our decision to dichotomize the outcome variable for service utilization, because this variable can comprise different types of services. In fact, when we considered all of our service variables, we noticed that most participants had used more than one service during his or her lifetime or during the past year. Very often all of these services are part of a continuum and are offered by one resource, which then refers a patient to another. Thus one person can be seen, for example, at an emergency unit and be transferred to a community resource or be hospitalized or, conversely, may be followed by the same doctor all this time. Moreover, we demonstrated that people with concurrent mental health and substance abuse disorders used almost the same services that persons with only mental health disorders used (
38 ).
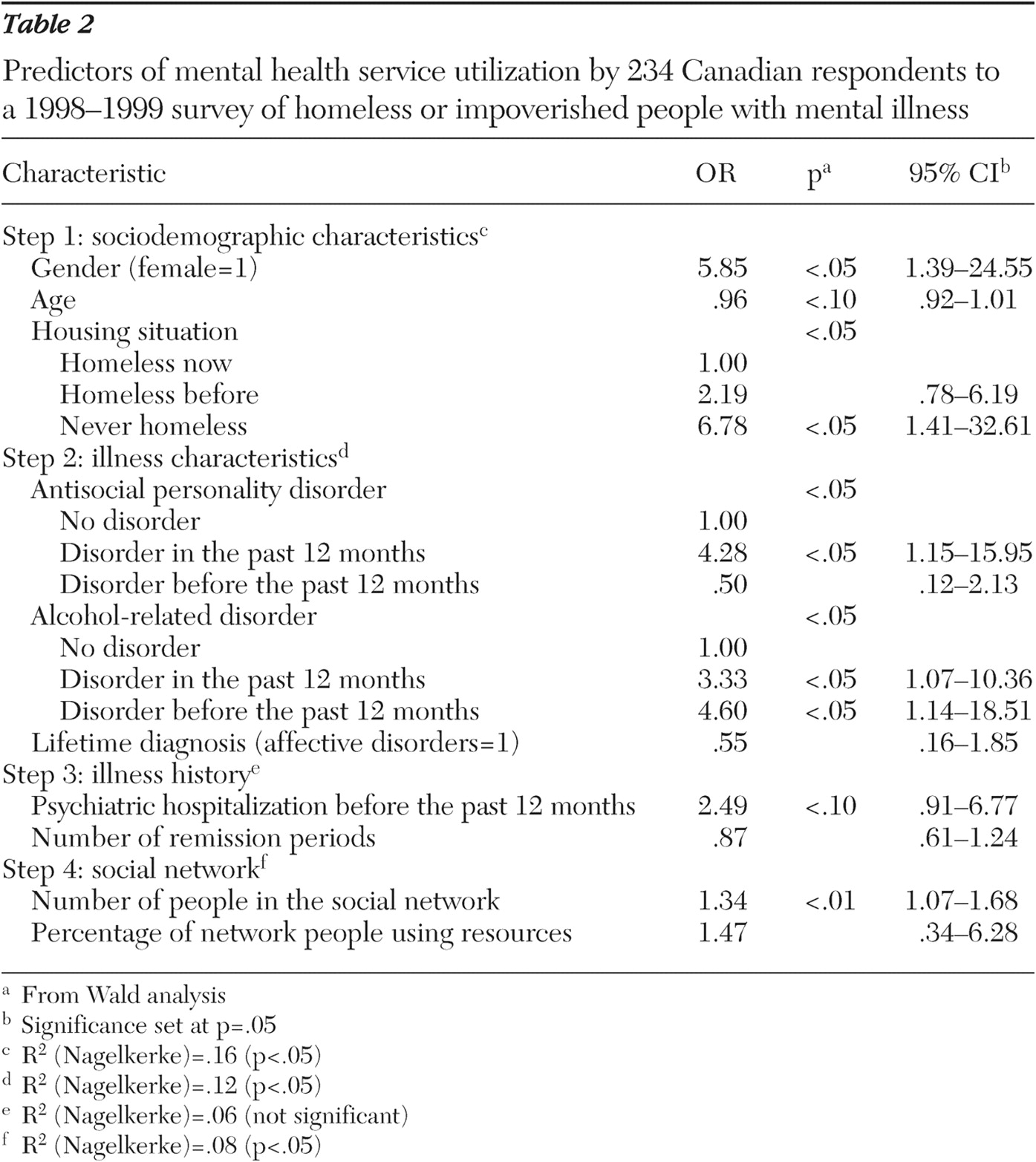
This study was the first to use the network episode model to identify these predictors. We found that all of the model's concepts except illness history were significantly related to utilization of mental health services. Illness history is undoubtedly the hardest to measure in this type of analysis. In our study, some variables reflecting the illness history, like medication compliance, could not be included in the regression analysis without creating an effect of collinearity with other variables. This concept will need more research in order to be better explained.
Only a handful of studies have used a model to analyze the use of mental health services by homeless or impoverished people. Using the Andersen-Newman model (
39 ), Padgett (
40 ) identified education, depressive symptoms, previous psychiatric diagnoses, previous psychiatric hospitalizations, and medical conditions as the main factors associated with service use. Other factors that have been identified with use of services include schizophrenia, lack of co-occurring substance use disorders, acknowledgment of a mental health problem, and having received mental health advice from outside the formal system (
41 ). In addition, both Wenzel and colleagues (
42 ) and Gamache and colleagues (
43 ) used the Andersen-Newman model to study homeless veterans and found that inpatient service use was related to the number of lifetime psychiatric symptoms, substance use disorders during the past year, and not sleeping outdoors or in public spaces. Outpatient service utilization was predicted only by psychiatric symptoms and evidence of liver dysfunction.
Our study confirms several of the findings of these studies in identifying the predictors of mental health service use by homeless people. However, unlike ours, the other studies were not conducted in the context of universal access to health care, making it difficult to assess the importance of each predictor independently. As a result, the interpretation of these previous findings may have attached a disproportionate amount of importance to issues of economic access to health care, with less focus on other potential barriers to access.
Our unique view of the use of mental health services in a free health care system confirms the presence of noneconomic barriers for people who are homeless or impoverished. We hope this important insight will allow the field to progress to a new level of understanding regarding this complex issue.
The findings of this study can be used to identify and target the underserved population but may also help community workers recognize and retain people who are being successfully served. We found that being a woman predicted utilization of services. Because women with mental health disorders are often victims of assault (
44 ), our findings underscore the importance of creating and maintaining resources that can ensure their security. There is also evidence, from the aforementioned authors, that women are more distressed than men by their mental disorders. Therefore, we suggest that it is also important to create multidisciplinary teams to help homeless or impoverished women reintegrate into normal life.
Our study indicated that people with mental disorders and co-occurring substance abuse or antisocial disorders utilize more services. Hwang and colleagues (
8 ), Canadian researchers, found that coordinated treatment programs designed to meet the needs of homeless people are effective in reducing alcohol and drug use. It may seem surprising that we found that antisocial personality disorder was associated with increased use of services, given that this population is known to reject authority. However, Booth and colleagues (
45 ) found that persons with substance use and antisocial personality disorders had more negative treatment results, leading to more intensive utilization of services. Our findings point to the need for more efficient and perhaps more integrated services to help this clientele who have multiple problems.
Our study also identified people who are least likely to seek care—namely men, older people, those without a fixed address, and those with small support networks. Brandt (
46 ) noted that because these patients are reluctant to have contact with services, it is very easy to forget them on the street. And Dixon and colleagues (
47 ) suggested that programs can be adapted for this clientele with a specific focus on their social network. Indeed, according to Denoncourt and colleagues (
48 ), people with serious mental disorders are often introduced to the outreach team by other workers or other homeless people.
Although the data were collected some time ago, between 1998 and 1999, as far as we know, there has been little change in the situation of this population since then. However, one limitation is that we did not interview people living exclusively on the streets, who have no contact with resources, and who make up 10% of the homeless population, according to the census. Toro and Warren (
49 ) found that people on the streets remain homeless longer. However, Hannappel and colleagues (
50 ) found no difference between the homeless using resources and those on the streets in terms of sociodemographic characteristics, psychological distress, and hospitalizations.
Another limitation of our study is that some people were unable to finish the questionnaire. We can assume that these people probably had more severe mental disorders or substance-related disorders, but our analyses showed that their exclusion did not significantly change our results. It is possible that our study's unique context of free access to health care services may itself influence mental health service utilization. For example, previous research (
51 ) in the setting of economic barriers to health care has found that co-occurring mental health disorder and substance abuse are associated with less utilization of services, whereas our study found these factors were related to more use of services. Perhaps, as suggested by Bland and colleagues (
52 ), in a system where everyone has equal rights to health care services, the more diagnoses an individual has, the more likely the person is to ask for services.