The provision of decent and affordable housing is one of the most important elements for integrating persons with serious mental illness into the community and is fundamental to their recovery. Housing is a basic human right, and having a home is a requirement of living in society (
1,
2 ). However, access to stable housing for persons with serious mental illness remains problematic. This may be explained by the fact that mental health professionals have planned housing for this population without the involvement of consumers (
3,
4 ). Numerous efforts have been made to evaluate housing for this population (
5,
6,
7,
8,
9,
10,
11,
12 ), but no one has simultaneously assessed consumers' and professionals' perspectives on a representative sample of all consumers in a catchment area. The purpose of this study was to evaluate the housing preferences of a representative sample of consumers living in all types of supervised settings in Montreal, Quebec, and to compare these preferences with the preferences of the consumers' case managers.
Housing preference studies of psychiatric consumers emerged in the 1990s (
13,
14,
15 ). Studies have consistently reported that consumers prefer independent living (
8,
15,
16,
17,
18,
19,
20 ), whether the consumers are inpatients (
21,
22 ), live independently (
21,
22,
23 ), or live in supervised housing (
24,
25 ). Studies have noted that consumers already living in their own apartment (
21,
22,
23 ) preferred autonomous housing more than those living in structured housing (
20,
24,
25 ). The housing preferences of consumers and their family members were examined by Friedrich and colleagues (
26 ), who concluded that consumers' families prefer housing with more support. Only one study compared consumer preferences with those of their treatment teams. Minsky and colleagues (
27 ) surveyed 80 hospitalized patients and treatment teams to compare their perspectives about appropriate housing. Patients preferred more independent living arrangements, whereas treatment teams favored more structured environments. Both families (
13,
26 ) and professionals (
27,
28 ) preferred more supported environments, with more staff care, than consumers preferred.
The housing preferences of the homeless population have been well studied. Persons without homes also would prefer to live independently (
29 ), and these proportions are no different from those of symptom-free homeless persons (
30,
31 ). Studies indicate that staff are also less likely to prefer independent living for homeless consumers (
30,
32 ).
Methods
This study was conducted in Montreal, the second largest urban center in Canada, with a population of 3.6 million (
33 ). The study population of 3,164 included all persons with a
DSM-IV diagnosis of serious mental illness living in housing supervised by the health and social service network in Montreal. In Quebec, as in the rest of Canada, health and social services are universally accessible and free of charge to consumers (
34 ). Hospital and community health services fall under the jurisdiction of the Quebec Ministry of Health and Social Services and have been regionalized over the past two decades.
Sample selection
Consumers had to meet the following criteria: a diagnosis of serious mental illness (schizophrenia, schizoaffective disorder, bipolar disorder, or major depression), a minimum of six months' residence in their current housing, age between 18 and 64 years, no primary diagnosis of intellectual handicap, a minimum of three months of supervision by a case manager, not living independently in an apartment, and considered well enough by their case manager to participate.
Sample selection involved a three-step process. First, an inventory of all housing for this population in Montreal was developed in consultation with administrators responsible for housing in the three major psychiatric hospitals and the regional health board. The housing inventory was organized into seven categories: housing in a hospital setting, hostels (larger than group homes, and with more supervision), group homes, foster homes, supervised apartments, social housing (low-income housing or cooperative), and private rooming homes. A list of all persons living in these seven categories was drawn up, and then a stratified random sample of 48 persons was selected in each category.
The case manager (social worker, nurse, psychologist, or community worker) initiated contact with each person selected and asked if he or she was interested in participating in the study. In case of refusal or ineligibility another person was selected in the same category until the 48-person quota was attained. Recruitment quotas were attained for five of the seven categories. Although all eligible persons living in a hospital setting were contacted (220 patients), only 38 persons were included for participation. Only 37 persons living in private rooming homes agreed to participate.
Overall 557 persons were contacted to participate in the study: 85 persons (15%) were excluded because of the case manager's judgment about the inability of his or her client to participate. Of the 472 potential participants, 157 persons (33%) refused to participate because of lack of interest. In all, 315 persons and their case managers were interviewed between April 2004 and April 2006. Although the number of persons residing in each of these housing categories was unequal, the number of persons recruited in the sample from each housing category was equal. Thus data presented were weighted to ensure that each person corresponded to the number of persons he or she represented in the population of reference. The weight attributed to each respondent is the inverse of its probability of selection in this population.
Instruments
Two instruments were administered: the Consumer Housing Preference Survey-Short Version (
14 ) and the Canadian Toolkit (
35 ). Both questionnaires were administered in English or French, depending on the language of the respondent. The short version of the Consumer Housing Preference Survey consists of 22 statements concerning the person's current living situation, housing preference, and support services required to live in the preferred housing. Most questions have a response choice. Although this questionnaire has not been formally validated, it has been frequently used to evaluate housing preferences (
30,
36 ).
In order to represent housing in Montreal, we modified Tanzman's (
14,
15 ) original list, from 12 housing choices to 15 housing choices, through a consultation process with key stakeholders: the Montreal Regional Health Board; administrators of three psychiatric hospitals; two panels of consumers, one English speaking and one French speaking; and representatives from the Federation of Nonprofit Housing in Montreal. The final list of housing presented to consumers and their case managers included six types of autonomous housing, six types of supervised housing, two types of institutional housing, and an "other" category. [The complete list of housing options is provided in an appendix in an online supplement to this article at ps.psychiatryonline.org.]
The Canadian Toolkit (
35 ) was also administered. This questionnaire provides sociodemographic data (age, sex, native language, and marital status), as well as education level, work history, residential history, and financial, legal, and diagnostic information.
Interviews lasted between 60 and 90 minutes and were conducted in the place chosen by the consumer. This included 151 in consumers' residences (48%), 73 in a hospital office (23%), 73 in a public setting (restaurant, café, or park) (23%), and 18 in the person's room or community organization meeting room (6%). Interviewers had backgrounds in social work, nursing, or rehabilitation. They all had previous experience with this population.
Participation in the study was voluntary. The research was approved by all hospital and community agency ethics review committees. After complete description of the study to participants, written informed consent was obtained.
Results
Description of sample
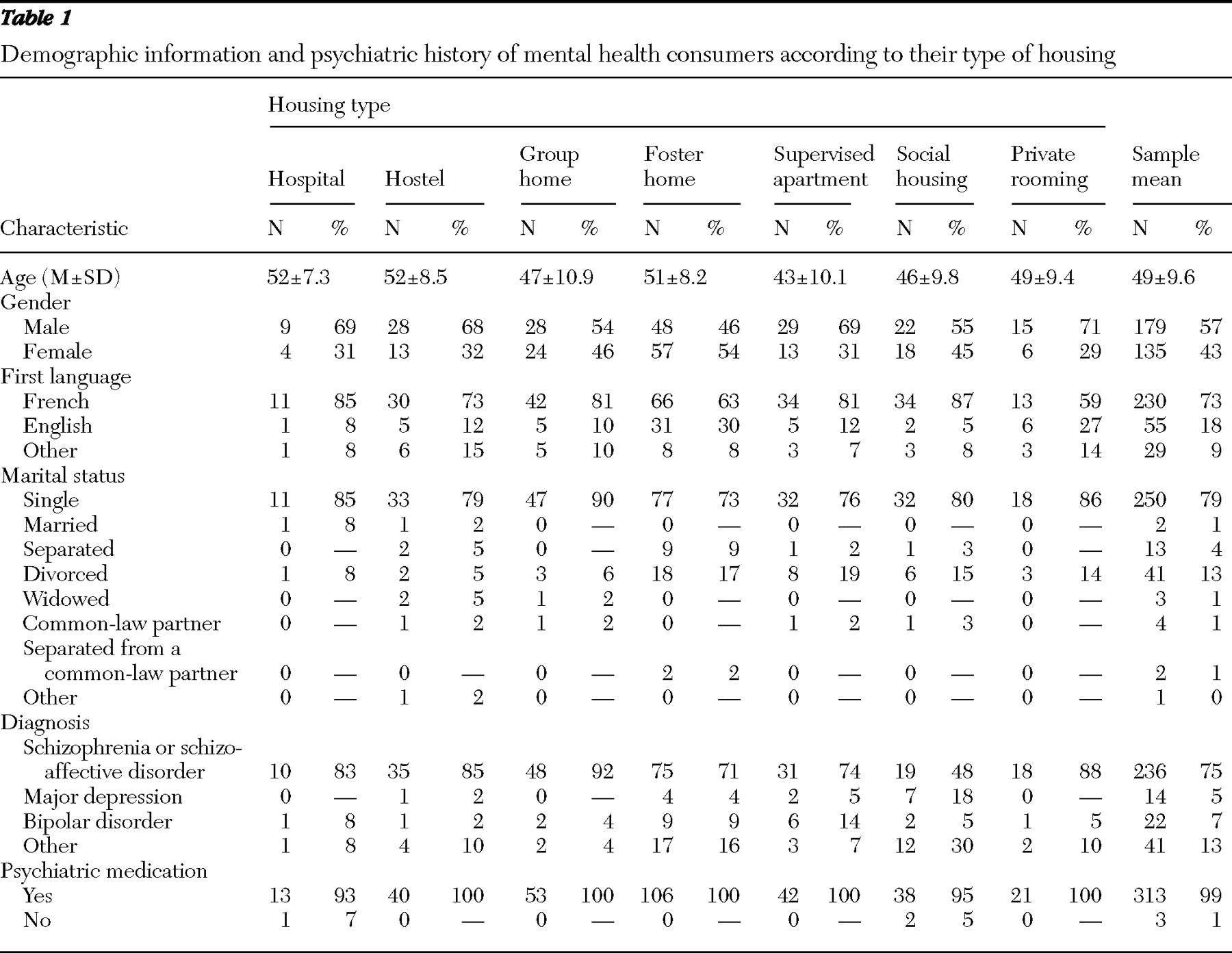
Consumers. Table 1 presents the demographic characteristics of the 315 residents. The mean age was 48.6±9.6 years. The sample was predominantly male, at 57%. Seventy-three percent of respondents' first language was French, 18% English, and 9% another language (Spanish or Italian). Most respondents were single (79%); only 2% were married or living with a common-law spouse.
Most respondents (75%) had a primary diagnosis of schizophrenia. Almost all respondents (99%) stated that they took medication for their psychiatric problems. A majority (N=139, or 44%) indicated that a psychiatric hospital was doing follow-up, and the remaining respondents indicated that an acute care hospital (N=105, or 33%) or a community organization (N=73, or 23%) was doing follow-up.
Case managers. A total of 179 case managers provided responses concerning 315 consumers (some case managers responded about more than one consumer). Most responses (N=230, or 73%) were from female case managers, and the average case manager's age was 44.9±10.5 years. More than half were 46 years and older. Forty-two percent of case managers were social workers, 28% were community workers, and 17% were nurses. A total of 156 case managers (50%) had more than 15 years of experience in the mental health field, and 56 (17%) had worked in this area for more than 25 years. Case managers participated in an average of 1.8 interviews (median=2) (
Table 2 ).
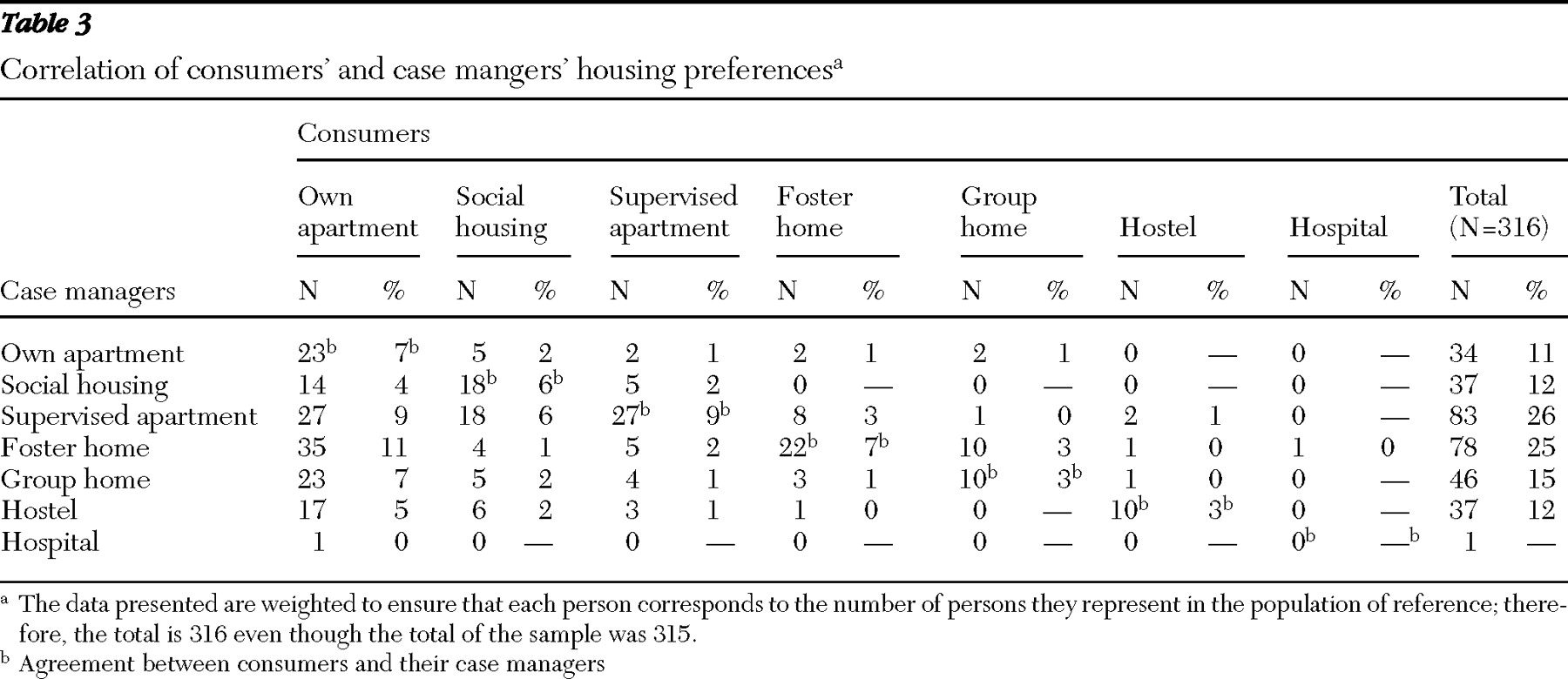
Overall housing preferences. Table 3 presents the overall housing preferences of consumers and their case managers. In all, 44% of consumers (N=140) preferred to live in their own apartment without subsidies, but only 11% of their case managers (N=34) preferred this choice for their clients. Social housing (N=56, or 18%), supervised apartments (N=46, or 15%), and foster homes (N=36, or 11%) ranked next in popularity among consumers. For their part, case managers preferred supervised apartments (N=83, or 26%) or foster homes (N=78, or 25%), group homes (N=46, or 15%), or hostels (N=37, or 12%) for their clients.
A third of all consumers indicated that they currently live in the type of housing that they would prefer to live in. In comparison, a majority (N=175, or 55%) of their case managers believed that consumers already live where they would prefer them to live. The most popular housing in which consumers were currently living and would prefer to live was social housing (N=17, or 44%), supervised apartments (N=18, or 44%), and foster homes (N=31, or 30%). However, for case managers, the most popular housing in which their consumers were currently living and in which case managers would prefer that they continue to live were supervised apartments (N=32, or 78%), followed by social housing (N=30, or 75%), hostels (N=28, or 67%), and group homes (N=26, or 50%).
For most consumers, their current housing ranked second to their preference of living in their own apartment. The only exception was consumers who were living in supervised apartments and preferred to remain there; 44% (N=17) compared with 29% (N=12) would prefer their own apartment. In contrast, case managers preferred (in six of the seven categories) that their clients live where they are currently living, with the exception of clients in a hospital psychiatric unit, to which case managers would prefer a group home. In order to better understand the specific choices of both respondent groups, we outline below the housing preferences according to where consumers lived at the time of the study.
Social housing
A majority (N=19, or 49%) of consumers living in social housing preferred to live in their own apartment, in contrast to 13% of their case managers (N=5). Otherwise 44% of consumers (N=17) already living in social housing preferred to live in this type of housing, compared with a majority (N=30, or 75%) of their case managers. Only 8% of consumers (N=3) living in social housing preferred to live in a more structured environment, such as a supervised apartment, compared with 13% of their case managers (N=5).
Supervised apartments
Consumers and their case managers ranked living in supervised apartments as their first preference. Forty-four percent of consumers (N=18), compared with 78% of their case managers (N=32), indicated a preference for this type of housing. Otherwise, consumers and case managers ranked a client's own apartment (N=12, or 29%, versus N=5, or 12%, respectively) as their second housing preference and social housing (N=11, or 27%, versus N=3, or 7%, respectively) as their third preference.
Foster homes
Forty-two percent of consumers (N=44) living in foster homes, compared with only 9% of their case managers (N=9), would prefer to live in their own apartment. However, 30% of consumers (N=31) already living in foster homes, compared with 48% of their case managers (N=51), preferred this type of housing. Consumers then ranked their preferences as social housing, 14% (N=15), compared with 2% of case managers (N=2); supervised apartments, 11% (N=11), compared with 29% of case managers (N=31); and last group homes, 4% (N=4), compared with 9% of case managers (N=9).
Group homes
Forty-seven percent of consumers (N=24) living in group homes would prefer to live in their own apartment, compared with 10% of their case managers (N=5). For almost one-third of these consumers (N=15, or 29%), a group home was their preferred type of housing, versus 50% of their case managers (N=26). However, 10% of consumers (N=5) in this category, compared with 2% of their case managers (N=1), preferred social housing. Only 4% of consumers (N=2), compared with 17% of case managers (N=9), would prefer foster homes, whereas 2% of consumers (N=1) in this housing versus 4% of case managers (N=2) would prefer to live in hostels.
Hostels
Close to half (N=20, or 49%) of consumers living in hostels indicated that they would prefer to live in their own apartment, compared with 2% of their case managers (N=1). Another 29% of consumers (N=12) already living in hostels indicated that they would prefer to live in this type of housing, compared with 67% of their case managers (N=28). A similar percentage of consumers (N=3, or 7%) and case managers (N=2, or 5%) preferred a supervised apartment. Finally, 5% of consumers (N=2), compared with 7% of case managers (N=3), would prefer a group home, and 2% of consumers (N=1), versus 19% (N=8) of case managers, would prefer a foster home.
Agreement between consumers and case managers
Overall, of the 315 pairs of consumers and their case managers, 35% (110 of 316) agreed on their housing preference (
Table 3, diagonal). Only 16% of case managers who would prefer that their clients live in their own apartment (23 of 140) agreed with them on their preference. This agreement increased to 32% for social housing (18 of 56), 43% for group homes (ten of 23), 59% for supervised apartments (27 of 46), 61% for foster homes (22 of 36), and 71% for hostels (ten of 14).
Discussion
This study's findings demonstrated that most consumers preferred living in housing that would offer them more autonomy than the housing in which they were currently living. The more autonomous the housing, the more popular it was. In each of the seven housing categories close to half of consumers wanted to live in their own apartment or in social housing. Although case managers also preferred more autonomous housing for their clients than where they were currently living, the case managers were more conservative in their preferences, preferring housing that offers more structure and clinical involvement, such as supervised apartments. This finding is similar to findings of previous studies (
27,
28 ). It is likely that case managers' preferences were influenced by several factors. Until recently, decisions about housing have been based on professional expertise—that is, knowledge of clients' clinical characteristics. In addition, case managers have been trained to minimize risk. Allowing consumers to choose their preferred housing and supporting more autonomous housing are not part of the professional culture in mental health care.
Although many consumers preferred to live in their own apartment, it was not a majority; only 44% of all consumers interviewed expressed this preference. This finding is in contrast to most studies, in which autonomous housing has ranked highest (
8,
14,
15,
16,
18,
19,
20,
21,
22 ). The composition of the sample in this study may explain this difference. In contrast to previous studies, the sample of consumers in our study lived in housing subsidized by the health and social service network and did not include persons living in their own apartments. Most previous studies included persons living in their own apartments. Although a majority of people with serious mental disorders and followed by health and social services in Montreal (about 1% to 2%, or 1,000 to 2,000 per 100,000 of the general population) live in their own apartments or with relatives, this study investigated the group that is heavily supervised and costly to the system. About 150 per 100,000 live in the types of residential settings investigated in this study (
4,
12 ). It is quite possible that this group may never have had the opportunity to discuss their preferences or, after having lived for many years in structured housing, may be afraid to live alone.
It is interesting that more than one-third of consumers preferred to live in their current housing before moving on to another type of housing. Social housing and supervised apartments were the most popular categories preferred by consumers already living in them, whereas hospital psychiatric units were the least popular. This was also true for case managers.
Although certain similarities existed between the housing preferences of consumers and their case managers, it would appear that the choices of the two groups were based on different criteria. Although it is probable that for consumers and case managers, living in more autonomous housing is an ideal to be attained, case managers seemed to favor a more gradual approach and viewed the need for greater support in the community as more important than consumers did.
Other hypotheses may help explain the case managers' preference for more structured housing. Case managers, because of their position, are more aware of the availability or the lack of housing for this population. In addition, case managers tend to be more conservative and prefer housing that is part of the health and social service network because they exercise a certain amount of control over these resources compared with community-based housing, about which they know less and over which they have little control (
12 ). In Canada, service providers are only beginning to learn about the recovery philosophy—the importance of consumer choice and risk taking in service provision. As this shift to a recovery orientation takes hold, case managers are being encouraged to rethink their previous notions about housing for this population.
This study has several limitations. The refusal rate may have introduced a bias. It is unclear whether the demographic and clinical characteristics of the consumers participating in the study were similar to, or different from, those who refused to participate. Social desirability may have also influenced the responses of consumers and case managers. However, recruitment of consumers was done randomly, and the population of reference included all persons with serious mental illness living in all types of subsidized housing in Montreal and part of the public managed care system covering this population. More important, the strength of this study is that findings were supported by a large representative sample of consumers matched to their case manager.
Conclusions
This study has important implications for future planning of housing for this population. Given that current national policies favor autonomous housing for persons with serious mental illness, our findings point to the need to take into consideration the viewpoints of mental health consumers. More important, when evaluating housing preferences, special attention should be given to the type of housing where consumers currently live. It is clear from this study that a variety of housing, not just autonomous housing, is necessary to meet the specific housing preferences of individuals.
Acknowledgments and disclosures
This study was funded through Project 3891 by the Fonds de Recherche en Santé-Quebec Health Research Fund. The authors thank the consumers and case managers who gave their time for this study.
The authors report no competing interests.