Recent national and local policy statements have promoted greater access to services and housing for homeless adults with behavioral health disorders (
1,
2 ). Despite this, extreme limitations on housing acquisition remain for homeless adults with disabilities. Obstacles include stigma associated with mental illness and substance use and the disparity between prevailing rent levels and the incomes received by individuals through federal or state disability programs (
1 ). The affordability problem can be addressed through rent subsidies, but prospective landlords may still exclude homeless people from housing based on other factors.
Criminal convictions can result in ongoing postincarceration consequences for people with mental illness in the areas of housing and behavioral health treatment (
3 ). Most rental subsidies are supplied by the federal government, which has established policies designed to severely limit access for people with a criminal history. For example, federal legislation enacted in 1996 required public housing authorities to enhance their screening of housing applicants so that more people with a criminal history would be excluded. Although housing authorities were required to reject applicants for only a few types of criminal offenses, typical implementations of the law followed rigid guidelines in excess of federal requirements. One analysis estimated that as many as 3.5 million Americans are currently ineligible for most federal housing assistance as a result of this law (
4 ).
Homeless individuals have high levels of criminal justice system involvement, especially when behavioral health problems are present, and homelessness is an overrepresented characteristic among inmates in correctional facilities. Nationwide data showed recent homelessness among people in U.S. jails was 7.5 times higher than the rate in the general population (
5 ). Immediate prior homelessness for a jail population in one city was found to be 16% among all inmates and 20% for inmates with psychiatric diagnoses (
6 ). Similarly, data for the entire population incarcerated in prisons and in jails show that 10% were homeless immediately before incarceration, and of the incarcerated population with mental illness, 20% were homeless (
7 ). Arrest rates for a sample of homeless adults over a 12-month period range from 10% for those without substance use disorders to 20% for those abusing alcohol or other drugs (
8 ). Almost one-quarter of all homeless adults have been in prison for a serious offense at least once (
9 ). Homeless adults with mental illness and lifetime incarceration lengths of at least six months are more likely than other homeless adults with mental illness but without an incarceration history to experience long-term homelessness (
10 ).
Although homeless adults with behavioral health problems have little ability to secure housing through the large stock of public housing mentioned above, there is a small but growing effort to create specialty programs designed to house and serve this particular population. Housing models within the array of approaches necessary to reach the goal of ending chronic homelessness fall under the rubric of "permanent supportive housing," and they have been shown to be successful at keeping formerly homeless people from returning to homelessness, with one-year retention rates of 72% or higher (
11,
12,
13,
14,
15 ). Additionally, such housing has been found to be preferred by consumers and less expensive than conventional psychiatric care residences, and consumers in supportive housing have housing tenure outcomes equivalent to those in more conventional psychiatric congregate care residences (
12 ). Failure in housing has been associated with younger age (
12,
13 ), substance abuse (
14,
15 ), and male gender (
11 ).
There is no uniform type of supportive housing, however, and programs aiming to house homeless people with behavioral health disorders use any number of techniques to select residents. Some programs, like those of Seattle's Downtown Emergency Service Center (DESC), employ an approach to select clients with the most severe challenges. This approach, where receipt of housing is not contingent on clinical stability or on acceptance of treatment or other services, is known as "Housing First" and shows promising results in terms of housing retention (
2,
16 ). Other programs attempt to limit risk exposure by screening out homeless clients who are assessed as being unsafe for housing. Studies of housing programs specifically created for homeless people with serious mental illness have reported high rejection rates based on perceived dangerousness (
17,
18 ).
Criminal recidivism data may have an influence on housing operator policies to exclude people with certain types of criminal records from housing. The data are clear that most individuals released from prison commit crimes again, but they typically do so quickly, with a diminishing risk of reoffense over time (
19 ). Individuals with mental illness who have been in prison for serious offenses likewise commonly commit new offenses after being released to the community, although only a small portion of these new crimes are felonies committed against other people (
20 ). In general, homeless individuals with mental illness, whether previously in prison or not, have high arrest rates for minor offenses (
21 ). However, those with an incarceration history have remained in mental health services nearly as well as those without any criminal history (
10 ).
Criminal history is useful in predicting short-term reoffense risks, but it has not been studied as a predictor of housing retention. It is unclear whether there is an empirical basis for the categorical exclusion of people with criminal backgrounds from housing. DESC's supportive housing programs were not created as specific criminal justice system interventions like the forensic assertive community treatment programs in place in a small number of communities (
22 ). Instead, the DESC program aims simply to alleviate the homelessness of highly vulnerable homeless people with mental illness. Because of the high level of involvement in the criminal justice system among homeless people with mental illness and the fact that DESC does not exclude people on the basis of criminal background, the program provides a good test site for examining whether individuals with various criminal histories are able to remain housed as long as otherwise similar people who do not have the same types of criminal backgrounds. The study was undertaken to discover whether exclusion from housing on the basis of the presence of a criminal history is sound policy for programs intending to assist individuals with housing retention.
Methods
This retrospective cohort study examined housing outcomes among adults with behavioral health disorders who moved into supportive housing operated by DESC in Seattle after having been homeless. DESC is a nonprofit homeless service agency providing supportive housing, emergency shelters, and mental health and substance abuse treatment for long-term homeless adults with disabilities. Supportive housing residents are provided with apartments, mostly in discrete supportive housing projects operated by DESC and staffed 24 hours per day, although some are in scattered-site leased apartments. Residents are offered comprehensive services, including psychiatric treatment, counseling, social supports, and assistance with obtaining food and meeting other basic needs, but resident acceptance of any of these services is entirely optional.
All individuals moving into DESC's housing between January 1, 2000, and June 30, 2004, were included for the purpose of examining risk factors and characteristics, particularly criminal background information, associated with the subsequent achievement of the dichotomous outcome variable of housing success (defined as maintaining continuous retention of housing for two years or, if moved out before then, going to appropriate living situations). All data came from existing information collected by DESC in the course of normal operations. Criminal history records collected by DESC came from public sources, principally the Washington State Patrol. Institutional review board approval was obtained from the University of Washington. Informed consent was waived because the study used deidentified administrative records and there was no contact with study participants.
Analysis
The primary research question was whether success or failure in DESC's housing is associated with the presence of any criminal history or with the presence of specific types of criminal backgrounds. Each criminal record was coded into one of 12 summary categories modeled on a taxonomy used in a study looking at recidivism among felons with mental illness (
20 ). Additional coding was done to organize crimes into four basic types, which allowed for the creation of a new "criminal versatility" variable, a count of how many of the four categories an individual's record included.
Basic demographic statistics and frequencies of the different crime types were examined. Bivariate associations between the independent variables and the outcome variable (housing success) were determined by using chi square tests, and relevant variables were entered in a logistic regression model to determine adjusted associations between the independent and outcome variables.
For bivariate associations with the outcome, one-sided (one-tailed) chi square results were used. The study was undertaken to discover whether exclusion from housing on the basis of the presence of a criminal history is sound policy for programs intending to assist individuals with housing retention. The basic hypothesis for this investigation was the null hypothesis, that there is no difference in the presence of criminal background among people who succeeded in housing versus those who failed. The one-sided test then provided greater opportunity for an association between criminal history and housing failure to be discovered, so using it was a more conservative strategy for testing the hypothesis.
Statistical tests were run with SPSS, version 13.0.
Results
There were 386 unique admissions to DESC's supportive housing in the study period, consisting of 371 different individuals, including 15 who had two separate admissions. Criminal background checks had been performed and added to the DESC data system for 342 of the 371 individuals (92%). Individuals who died within two years of moving in were excluded from analysis. The remaining 332 individuals had 347 unique residencies in DESC housing during the study period, thus accounting for 347 total cases in the analysis.
Basic characteristics of the 332 unique individuals included in the final analysis are shown in
Table 1 . Nearly all had a mental illness, and most had a substance abuse problem. A majority (52%) had at least one criminal conviction.
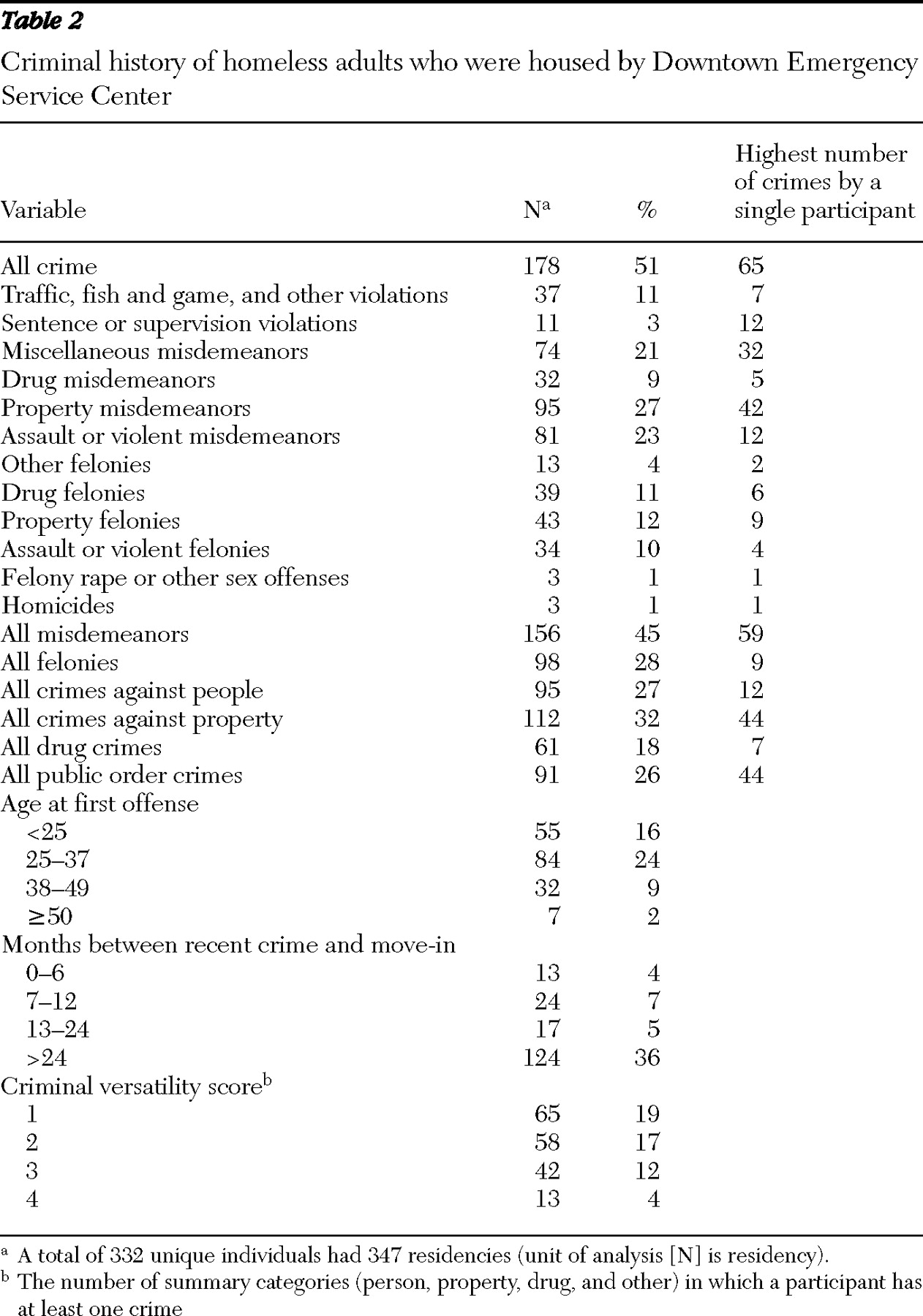
Criminal background information for all 347 cases appears in
Table 2 . The average number of crimes per resident was 3.1, or 6.1 when looking only at people with convictions. Although a majority of participants committed at least one crime and 45% had at least one misdemeanor, no particular crime classification or other grouping was common to as many as one-third of participants. Property crimes were most prevalent, at 32%. Twenty-eight percent of participants had felony convictions.
The housing success rate was 72% (N=249), accounting for participants who went on to reach two years of continuous residency in DESC's housing or who moved out to appropriate and adequate housing before two years. Seventy percent (N=124) of participants with a criminal history achieved the outcome, compared with 74% (N=125) of participants without a criminal history. The difference was not statistically significant with chi square testing (Fisher's exact test, one-sided). Expressed another way, 50% of the participants achieving the outcome had a criminal history, compared with 55% of the participants failing to succeed in housing.
Associations between the demographic characteristics of the study population and housing success are shown in
Table 3 . Few differences among the participants appeared to be associated with the outcome. Older participants at time of move-in were more likely to succeed than younger participants, as were participants without substance abuse problems, compared with those with substance abuse problems. No other variable reached statistical significance when compared against the outcome.
Testing of specific types of criminal history against the outcome showed statistically significant associations between only two crime variables and housing success (
Table 4 ). Higher numbers of property and drug crimes were associated with lower housing success rates.
Multivariate analysis using logistic regression showed a different result. Higher numbers of drug crimes and property crimes and the presence of a substance abuse problem were not associated with housing failure when adjustments were made for each other and for move-in age. Move-in age remained significantly associated with housing success when analyses adjusted for the other three variables in the model. Specifically, the odds that a person under the age of 38 at time of move-in would succeed in housing were .49 times the odds that a person 50 or older would succeed in housing (95% confidence interval=.17–.80, p=.04). None of the other variables reached statistical significance when analyses adjusted for the other variables.
Move-in age was compared with substance abuse to help in determining why adjusting for age caused substance abuse to be insignificant in multivariate analysis. The mean age of participants with substance abuse problems (43.1 years) was significantly less than the mean age of participants without substance abuse problems (46.9 years) in an independent-samples t test (p<.001).
Additional analysis was performed to address the possibility that participants shown as having no criminal history may in fact have had criminal records in other states. Elapsed time between each participant's first entry in the DESC database (related to the use of any DESC service, including emergency shelter or contact with street outreach workers) and the date of move-in to supportive housing was a gauge of how long the person was known to DESC and therefore may have been in Washington. Comparing mean time known to DESC of people achieving the outcome of housing success versus people not achieving the outcome yielded no difference between the groups. People failing in housing were known to DESC an average of 5.8 years before move-in, compared with 5.6 years for people succeeding in housing.
Discussion
Criminal history appears to be largely unrelated to the ability of homeless persons with behavioral health disorders to succeed in supportive housing, suggesting that policies and practices that keep homeless people with criminal records out of housing may be unnecessarily restrictive.
People with a more extensive criminal history succeeded at rates equivalent to those of others, as did people with more recent criminal activity, people with more serious criminal offenses, and people who began criminal activity at an earlier age. In other words, the criminal history of those who succeeded in housing was nearly indistinguishable from that of those who failed in housing.
Our finding that younger age was associated with housing failure is consistent with findings from other studies (
12,
13 ). The older cohort may comprise people with less severe disabilities, as a result of premature mortality among those who had been in the cohort previously. Alternatively, because of physical limitations that increase with age, those who are older may be less likely to leave housing. The study data set did not contain information sufficient to point to the likely underlying reason, however.
Policy implications
Examinations of similar questions about criminal history and housing retention do not appear in the literature, making this study unique and its findings new. The finding that criminal history does not provide good predictive information about the potential for housing success is additionally important because it at least partially contradicts the expectations of housing operators and others. It certainly runs counter to common beliefs that housing needs to be free of offenders in order to be safe for the other residents. Public entities and individual housing operators use criminal background information to assess for risk and screen out undesirable people, perhaps with little resulting value in terms of housing success outcomes among the people they choose to house.
The results of this study also suggest that recidivism potential is not a good proxy for housing problems. Reoffense is common among offenders, but offenders succeeded in housing as did nonoffenders. It is unknown whether study participants with a criminal history were committing crimes after entering the supportive housing. If they were, there appeared to be little effect on their ability to remain housed.
Other known predictors of criminal recidivism, such as young age at first offense and high criminal versatility, also were not associated with failure to succeed in housing, supporting the theory that criminal activity is not necessarily related to housing retention abilities. It may be that supportive housing reduces the continued criminal activity of previously homeless individuals or that criminal behavior can be compartmentalized away from the housing so that tenancy is not affected. In either case, there are implications for further study.
Limitations
Limitations of the study included criminal data reliability and sample size concerns. Criminal history data were retrieved by DESC from public records that are normally available to housing operators and others. As such, records are not necessarily as complete as those a researcher might expect to acquire if conducting research in conjunction with criminal justice system officials, although presumably the records are more reliable than if the information had been obtained from participant self-report. Additionally, no criminal history information from outside Washington was available, creating the likelihood that some participants actually had criminal pasts that did not show up on their clean Washington records. Analysis of the amount of time participants had been connected in some way or another to DESC showed that this limitation likely applied evenly to both the housing success and housing failure groups, however.
The sample size allowed for determining only medium effects of any of the predictor variables on housing success. A larger sample could have shown that some of the subtle differences seen among participants were statistically associated with housing success, but it is unclear how useful that would be. Without substantial predictor differences between people who succeed in housing and those who fail, housing operators would get little utility out of the information. For example, a 5% housing success difference between people with one type of criminal background and people without that background would probably not provide enough information of value to cause an operator to make changes (that is, to adopt policies to reject those with the particular background or, if accepting them anyway, to develop different approaches for serving them better). In short, small effect sizes would suggest little in the way of policy consequences.
Study participants were representative of the highest-priority clients seen by DESC in Seattle. DESC sees many thousands of homeless individuals over the course of any given year, and it focuses its efforts and prioritizes its housing and other resources for clients deemed to be most vulnerable. These individuals are generally considered to be the most difficult to serve or difficult to house of the homeless population, and in recent years they increasingly have been referred to as the chronically homeless. Although chronic homelessness status was not examined for participants in this study, in a recent study, 84% of a small sample of DESC housing residents (N=25) were found to fit the definition of chronic homelessness (
16 ). Because the study presented here involved individuals with specific characteristics (lengthy homelessness and behavioral health disorders) who received a particular intervention (supportive housing), generalizing the results of our study to other situations may not be valid. It may be that the robust array of clinical, social, and recreational services tailored to the individual needs of DESC's supportive housing residents, which has been described in part elsewhere (
2,
16 ), is what allows participants with a criminal history to succeed in housing. There are substantial numbers of supportive housing programs for homeless people with behavioral health disorders, however, so the results still may be relevant to a large audience.
Conclusions
The results of this study call into question the wisdom of policies attempting to predict tenancy success by the use of criminal background information. A link between criminal history and housing failure has been assumed in the establishment of screening criteria for a long time, but empirical evidence of the link has not been studied and reported. The fact that this study found no link should help establish the need for larger, multisite studies to be done to establish stronger conclusions about the predictive utility of criminal background information. If the findings of this study are supported, housing policy should be altered to ensure that criminal history does not remain the barrier to housing acquisition it is now. If the findings of this study are not supported, additional study will help provide an evidence base for the establishment of programs targeted to subsets of the population more likely to fail.
Acknowledgments and disclosures
David Lovell, Ph.D., provided guidance on the statistical analyses. Dr. Lovell and Jack Thompson, M.S.W., provided review comments on an earlier version of this article.
The author reports no competing interests.