Suicide among elderly persons is a matter of grave concern. According to Waern and colleagues (
1 ) one-fifth of all suicides are committed by elderly persons. Suicides have been predicted to become the tenth most common cause of death of older people in the world, although in some countries a decreasing trend in suicides among elderly has also been observed (
2,
3 ).
On the basis of psychological autopsy studies, psychiatric disorders (most commonly depression) have been found to be involved in 75% to 97% of all suicide cases (
4,
5,
6 ). Depression seems to be more strongly associated with suicide in older age groups than in other age groups (
5 ), and several additional psychiatric disorders have been observed among at least one-third of elderly suicide victims (
6 ).
Regardless of the age group monitored, a higher proportion of suicides occurs during the first few weeks after discharge from psychiatric hospitalization (
7,
8 ). Focusing on only the elderly population, Erlangsen and colleagues (
9 ) confirmed these observations. Suicide risk has also been reported to be significantly higher among patients who had spent less than the average amount of time in hospital care or had not had any treatment at all (
10 ).
The aim of our study was to investigate the timing of suicide among elderly and middle-aged persons after their final hospitalization. The characteristics of suicides were examined in relation to the timing of suicide and compared between elderly and middle-aged victims. By using a large suicide database (and focusing on elderly persons), we were able to study the characteristics of suicides within one week after hospitalization, compared with different time periods.
Methods
The database consisted of all suicide victims (N=1,877; 1,535 males and 342 females) from 1988 to 2003 from the province of Oulu in northern Finland. The study presented here included all of the suicides committed in two age groups: middle aged (50–64 years; N=370; 284 males and 86 females) and elderly (65 years or older; N=194; 146 males and 48 females). In addition, we used data from the Finnish Hospital Discharge Register, which included treatment histories of hospitalized patients in all somatic and psychiatric wards. Diagnoses of suicide victims were converted to
ICD-10 classification according to National and Development Centre for Welfare and Health instructions (
11 ) as follows: schizophrenia and other psychoses, F20–F29; mood disorders, including depression, F30–F34.1; substance use disorders, including alcohol-related disorders, F10–F19; and other psychiatric diagnoses, F00–F09 and F40–F61. The study protocol was approved by the ethics committee of Oulu University.
Our data contained only cases that were classified as suicides by the forensic examiner. Data on age, gender, suicide method (violent: hanging, drowning, shooting, jumping from a height, into traffic, and other methods; nonviolent: poisoning and gas), previous suicide attempts, and whether or not a victim was under the influence of alcohol at the time of the suicide were based on the information from the forensic medicolegal autopsy investigations. Data from elderly suicide victims were compared with those from adult victims aged 50–64 years from the same area.
The suicide victims were categorized into five groups according to the number of days between the last hospitalization and suicide: one to seven, eight to 30, 31–90, 91–180, and more than 180 or no previous hospitalizations. For statistical analyses, the group that committed suicide between one and seven days was used as the control. Statistical significance of group differences in categorical variables was examined with Pearson's chi square test. The statistical software used in the analyses was SPSS, version 14.
Results
Among all suicide victims aged 50 years and older, 86 (15%) committed suicide during the first week and 154 (27%) during the first month after hospitalization. No statistically significant difference was found between the middle-aged and elderly groups in the timing of the suicides. A statistically significant gender difference in suicide timing was noted for elderly persons but not for middle-aged persons. That is, almost one-half of elderly female suicide victims (N=23, 48%) committed suicide in the first month after hospitalization, but for elderly male victims, the proportion was 25% (N=36) ( χ 2 =9.23, df=1, p=.002).
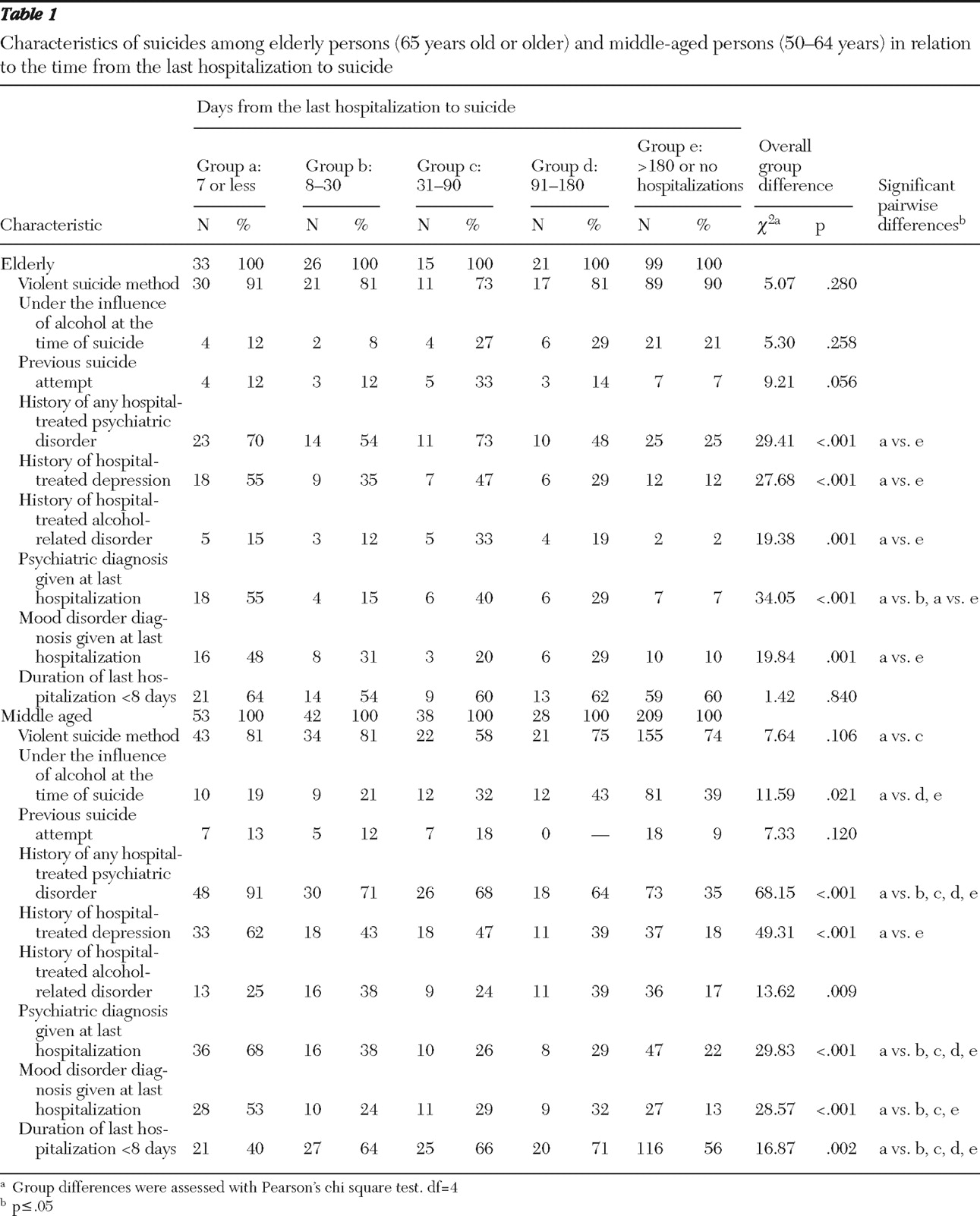
Characteristics of the suicides (as well as overall and pairwise differences in the elderly and middle-aged groups) in relation to time after last hospitalization are presented in
Table 1 . Persons who committed suicide within one week after hospitalization were the reference group for pairwise comparisons. Among elderly victims, compared with persons whose suicide took place 180 days or more after hospitalization or who had not had any hospitalization, those who committed suicide within one week were more likely to have a history of a hospital-treated psychiatric disorder (70% versus 25%) (
χ 2 =21.13, df=2, p<.001), a history of hospital-treated depression (55% versus 12%) (
χ 2 =25.37, df=2, p<.001), and a history of hospital-treated alcohol-related health problems (15% versus 2%) (
χ 2 =8.50, df=2, p=.004). Furthermore, among elderly persons who committed suicide 180 or more days after hospitalization or who had not had any hospitalizations, elderly persons who committed suicide within one week were more likely to have been given a psychiatric diagnosis (55% versus 8%) (
χ 2 =31.78, df=2, p<.001) or a diagnosis of mood disorder during their last hospitalization (48% versus 10%) (
χ 2 =19.60, df=2, p<.001). A diagnosis of a psychiatric disorder given during the last hospitalization was also significantly more common among those who committed suicide during the first week after hospitalization than among those who committed suicide within eight to 30 days (54% versus 15%) (
χ 2 =9.54, df=2, p=.002).
We found differences between elderly and middle-aged victims. Among those who committed suicide within one week after hospitalization, a larger proportion of elderly persons had a final hospitalization stay less than eight days (elderly, 64%; middle aged, 40%) ( χ 2 =4.69, df=2, p=.030), and a smaller proportion had a history of hospital-treated psychiatric disorders (elderly, 70%; middle aged, 91%) ( χ 2 =6.15, df=2, p=.013). Among those who committed suicide eight to 30 days after hospitalization, we found statistically significant differences between those with a history of hospital-treated alcohol-related disorders (elderly, 12%; middle aged, 38%) ( χ 2 =5.63, df=2, p=.018). Third, among those who committed suicide more than 180 days after hospitalization or who were never admitted to a hospital, a larger proportion of elderly persons used a violent method of suicide (elderly, 90%; middle aged, 74%) ( χ 2 =10.11, df=2, p=.001), and a smaller proportion were under the influence of alcohol at the time of suicide (elderly, 21%; middle aged, 39%) ( χ 2 =9.34, df=2, p=.002), had a history of hospital-treated alcohol-related disorders (elderly, 2%; middle aged, 17%) ( χ 2 =14.36, df=2, p<.001), and had received a psychiatric diagnosis during the last hospitalization (elderly, 8%; middle aged, 29%) ( χ 2 =14.41, df=2, p<.001). In the group of persons who committed suicide 180 days after hospitalization or who were never admitted to a hospital, a smaller proportion of elderly persons had never been hospitalized (elderly, N=10, 10%; middle aged, N=43, 21%) ( χ 2 =5.17, df=2, p.023).
Discussion
The novel findings of our study are that about 30% of all suicides among elderly and middle-aged populations occurred during the first month after discharge from a hospital. Significantly more elderly (N=23, 48%) than middle-aged women (N=29, 34%) committed suicide within that time frame. A higher proportion of elderly women than elderly men committed suicide within one month after being discharged from a hospital, a finding that could indicate a higher degree of impulsiveness and intent among female victims. This phenomenon was, however, not apparent among middle-aged women.
It also seems worth mentioning that about 80% of the diagnoses given during the last hospitalization among elderly persons were nonpsychiatric. It would, therefore, seem important for all physicians, not only psychiatrists, to recognize the suicide risk that elderly persons face when they leave a hospital after having been treated for a general medical condition. Suicide risk among elderly persons has been noted to increase in connection with serious illness and physical or psychiatric disorders leading to hospitalization (
1 ). Our observation that over half of the elderly victims had committed suicide within a week after the psychiatric hospitalization suggests that the proper length of hospitalization should be evaluated on an individual basis, with special emphasis on appropriate treatment results. During the past two decades the number of psychiatric and psychogeriatric beds has been reduced in Finland without proper resourcing of outpatient care. This has led to shorter hospital stays, which may have diminished the efficacy of suicide risk recognition and treatment of patients with depression. The growing number of elderly people should be taken into account in the allocation of treatment resources, because elderly persons require extensive evaluation periods and more time for the various treatment interventions to reach their goals.
Suicides are frequently committed under the influence of alcohol, and alcohol dependence considerably increases suicide risk in the general population (
12 ). However, among elderly persons, alcohol dependence has less commonly been reported to be a risk factor (
13 ). Our results are in line with this and show that elderly victims are very seldom under the influence of alcohol when the suicide occurs within one month after hospitalization. However, a study by O'Connell and colleagues (
12 ) showed that after more time elapses after hospitalization (one to three months), prevalence of alcohol use among elderly persons at the time of the suicide increased almost threefold. Thus loss of control as a result of alcohol intoxication may not contribute to suicide immediately after discharge from a hospital among people aged 65 years or older, although it seems to link with suicide risk in later periods from hospitalization. This is also in line with findings from our previous study, in which we showed that elderly suicide victims experienced fewer hospitalizations as a result of alcohol-related disorders, suggesting that history of alcohol abuse cannot be effectively used in identifying suicide risk among elderly persons (
14 ).
Even though the proportion of violent suicide methods among elderly persons was extremely high, no association with suicide timing was apparent. A disproportionately high number of violent suicides has been noted among elderly persons (
4,
15 ), and previously we have reported that violent suicides were especially common among elderly men, reaching higher rates than those seen for the whole general population of Finland (almost 90% for elderly males versus 70% for the whole population) (
14 ).
The strength of this study was that all suicides committed in the province of Oulu during the study period were included and evaluated. The study was based on reliable national register information on deaths and hospital admissions, and thus the timing of suicide in relation to hospital admissions could be defined with high precision. However, because this study was based on register information on hospital admissions, lack of chart data on individual psychiatric diagnoses is a limitation. Some suicide victims may have been treated in outpatient settings and would then have become cases without coded diagnoses. Unfortunately, there are no common national registers for outpatient treatment in Finland. Finally, although the main findings are statistically robust, some degree of type II error may have occurred and some risk of spurious findings (that is, type I error) also exists.
Conclusions
We found that in our suicide database, elderly women were more likely than elderly men to commit suicide within one month after discharge from a hospital. Because suicide risk in this particular subgroup is, however, a low-incidence problem, it would be helpful if screening specifically targeted elderly women (and men) with depression or multiple general medical conditions, because these factors have been shown to be related to an increased suicide risk (
3 ). In addition, use of a combination of effective psychotherapy and antidepressant medication may result in better outcomes even with shorter hospitalization periods (
7 ). We also highlight the importance of organizing proper outpatient treatment immediately after discharge from a hospital, especially in cases that involve elderly patients with a history of a psychiatric disorder.
Acknowledgments and disclosures
This study was funded by grant 113 760 from the Finnish Academy.
The authors report no competing interests.