Although considerable research focuses on the effect of particular antipsychotic drugs on patient outcomes, less attention is paid to public policy decisions that may change access to particular medications. The limited evidence suggests that prior authorization requirements do not reduce pharmacy expenditures or overall costs (
1,
2 ) and may increase discontinuities in treatment (
2,
3 ). This study aimed to further develop the policy research agenda by studying the short-term impacts of the removal of injectable risperidone long-acting therapy from the Florida Medicaid preferred drug list (PDL) in April 2006, although it remained available when providers requested prior authorization from the Medicaid program. Risperidone long-acting therapy is a parenteral use extended-release microsphere formulation (injection plus diluent) second-generation antipsychotic that was released to the market in 2003, targeted to patients with significant medication adherence problems, and shown to be effective in clinical trials (
4 ).
The impacts of the policy change were studied by contrasting the effects on health care utilization, costs, and outcomes for two groups of recipients aged 18–64 with diagnoses of schizophrenia or schizoaffective, bipolar, or other psychotic disorders who received risperidone long-acting therapy—Medicaid beneficiaries continuously enrolled when the policy was changed (PDL group) and those who received risperidone long-acting therapy in April 2005 (non-PDL group). Although some recipients in both groups discontinued their medication treatment for clinical reasons, we anticipated that the discontinuations in April 2006 would include some individuals who had been stable on risperidone long-acting therapy for whom providers did not seek prior authorization. We hypothesized that this group would experience more acute care events and poorer short-term outcomes than the 2005 group, which was unaffected by the policy change. Short-term impacts were studied because issues of adherence and high utilization with this population made longer-term attribution to the policy change questionable.
Methods
Medicaid pharmacy claims were analyzed to identify episodes of risperidone long-acting therapy. A treatment episode was defined as a series of at least three injections, with the third injection occurring within 42 days of the first, as indicated in Medicaid pharmacy claims. The discontinuation date for the episode was 28 days after the last injection. These criteria are based on the Risperdal Consta package insert and on reviews of multidose studies indicating that injections should be given on a 14-day schedule (
5,
6 ). Stable plasma concentrations generally are not achieved until after the third or fourth injection and, once reached, are maintained for four to five weeks after the last injection.
We examined Medicaid behavioral health inpatient, outpatient, physician, and pharmacy expenditures for 60-day pre- and postperiods. Specifically, for individuals who did not discontinue risperidone long-acting therapy, we examined the 60 days before and after the policy change for the PDL group and pre-post April 2005 for the non-PDL group. For individuals who discontinued risperidone long-acting therapy, we examined the periods 60 days before and after the discontinuation date, which was 28 days after the last injection. Measures of acute care utilization included whether the individual had behavioral health-related emergency visits, inpatient stays, and involuntary psychiatric evaluations (an indicator of psychiatric instability) during each of the 60-day periods. The number of events was also examined, as was an overall measure of acute care use that indicated whether the individual experienced any of these events during the two comparison periods.
Propensity score matching was used to match individuals in the PDL and non-PDL groups on the basis of demographic characteristics (age, race, and gender), diagnosis, and preperiod utilization. We used nearest-neighbor matching with global optimal matching methods (
7 ). A difference-in-difference approach was used for the matched samples to examine health care use and expenditures for the treatment and comparison groups:
Image (m_kj18e1.jpeg) is missing or otherwise invalid. The pre-post difference for the PDL group was compared with the pre-post difference for the non-PDL group. The effect of the policy change is the difference in the pre-post differences. Changes in categorical outcomes were examined via logistic regression analysis, and changes in continuous measures were examined with nonparametric Mann-Whitney U tests. Exact p values were used with both methods to determine whether the difference-in-difference results were statistically significant. The nonparametric Mann-Whitney U test was appropriate, given the skewed distribution of the changes in the number of events and expenditures. This project was approved by the University of South Florida Institutional Review Board.
Results
There were 247 risperidone long-acting therapy users when the policy change was implemented in April 2006. Fifty-one percent of the PDL sample was female (N=126), 41% were white (N=101), and 31% were black (N=77). The mean±SD age of recipients was 43.7±12.3, and 61% (N=151) had a diagnosis of schizophrenia. Differences between the matched samples did not achieve statistical significance. Thirty-six percent (N=89) of risperidone long-acting therapy users discontinued the medication in the 30 days after implementation of the PDL restriction. For comparison, 15% (N=37) of the matched sample of users of risperidone long-acting therapy in April 2005 discontinued use; thus the discontinuation rate more than doubled with the PDL restriction.
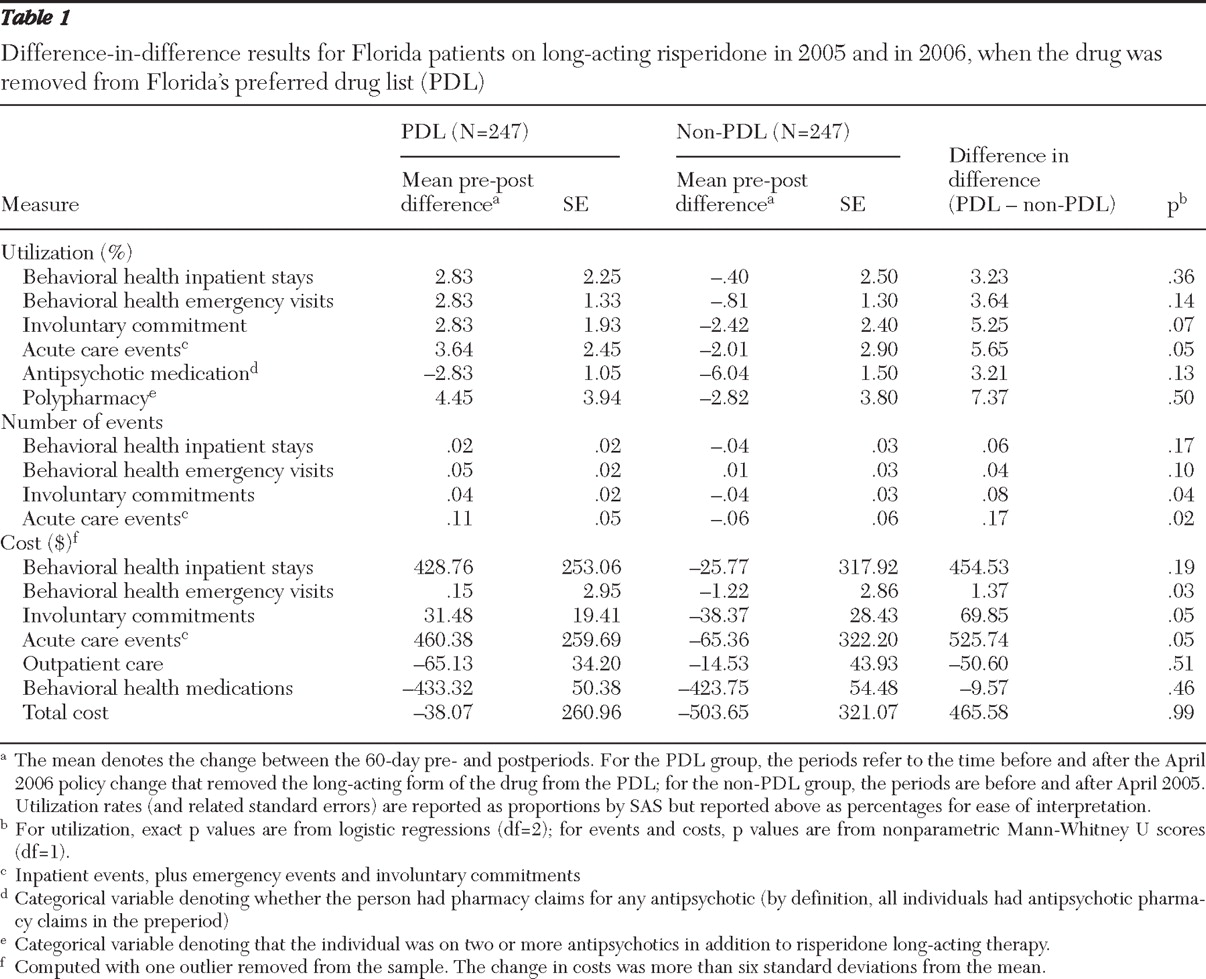
Table 1 shows the difference-in-difference results. PDL users tended to have increased acute care events after the policy change, whereas acute care events declined for non-PDL users. The results were significant (at p<.05) for the number of involuntary commitments and acute care events. The results for costs were significant for emergency visits, involuntary commitments, and overall acute care events. Pharmacy costs fell for both groups as patients switched to less expensive medications and because some risperidone long-acting therapy users discontinued all antipsychotics (3%, N=7, of the PDL users and 6%, N=15, of the non-PDL users). Because of the policy change, discontinuation rates were much greater in the PDL sample. In addition, the logistic regression used to estimate the propensity scores showed that the average number of days on risperidone long-acting therapy was significantly less for the non-PDL sample (137 versus 256 days,
χ 2 =63.9, df=1, p<.01).
Discussion
The greater discontinuation rates in the PDL group and the significantly fewer days on long-acting risperidone therapy in the non-PDL sample suggest that some individuals in the PDL group were stable on the medication and may not have switched or ceased use in the absence of the PDL restriction. Prior research has suggested that patients who are stable and switch medications are at risk of acute care outcomes (
8 ). As hypothesized, relative to individuals who received risperidone long-acting therapy in the prior year, those who received the same therapy at the time of the policy change had an increase in acute care events, including emergency room visits and involuntary commitments. Overall the policy change did not reduce total expenditures for the Medicaid program.
This study examined 60-day periods before and after the policy change. Studying short-term impacts is important because additional support may be provided for individuals particularly at risk of negative consequences when a policy change is implemented. Among individuals who discontinued risperidone long-acting therapy at the time of the policy change, deterioration of outcomes was most evident among individuals with schizophrenia. Hospitalizations, involuntary commitments, and overall acute care events increased among individuals with schizophrenia. Hospitalizations also increased among blacks, and the number of emergency visits increased among women and younger individuals. Future work should address whether such interventions are cost-effective.
Risperidone long-acting therapy is not the first second-generation antipsychotic to be removed from Florida's PDL. Removal of olanzapine from the PDL for two months in 2005 was associated with increased hospitalization and emergency visits. Reductions in pharmacy expenditures were offset by increased expenditures for acute care events (
3 ). Thus the findings with change in PDL status for risperidone long-acting therapy are consistent with other research examining the removal of a single antipsychotic from the Florida Medicaid PDL.
There were several limitations to this study, such as lack of data from the Medicare Part D program and for Medicaid beneficiaries enrolled in health maintenance organizations. Also, this study focused on a single antipsychotic medication and may not generalize to other antipsychotics or classes of medications.
Conclusions
Florida Medicaid implemented a policy change that removed risperidone long-acting therapy from the PDL in 2006. Risperidone long-acting therapy remains available to recipients if providers seek prior authorization. In this study the PDL restriction was associated with increased acute care events and did not result in significant savings to the Medicaid program.
Acknowledgments and disclosures
This research was supported by funding from Ortho-McNeil Janssen Scientific Affairs, L.L.C. Dr. Robst, Dr. Constantine, and Dr. Teague received funding from Ortho-McNeil-Janssen, where Dr. Howe is an employee. Dr. Howe also owns shares of Johnson & Johnson stock. The other authors report no competing interests.