Twenty-five years of empirical research have established that assaults on health care staff by patients are an ongoing workplace risk (
1—
9) that may result in human suffering, medical expense, and lost productivity (
2—
6,
8,
9).
The Assaulted Staff Action Program (ASAP) is a voluntary, systemwide, peer-help, crisis intervention approach for addressing the psychological sequelae of patients' assaults on staff (4-6). The program is based on the dynamics of victimology, especially disruptions in the victim's mastery, attachments, and meaning. Mastery is viewed as one's ability to reasonably shape one's environment, attachments as the caring and support of others, and meaning as the ability to make understandable sense out of what has happened.
When an assault occurs, the charge nurse calls the hospital switchboard. The ASAP staff member on call is beeped, and he or she goes directly to the site and offers crisis counseling or defusing to the employee victim. If the employee accepts the intervention, the ASAP staff member monitors the victim for symptoms associated with psychological trauma and helps restore the victim's mastery, attachments, and ability to make meaningful sense of the event immediately on site and over the next ten days. The program also offers debriefing of ward or unit staff where assaults occur, a victims' support group, family counseling for victims, and referrals for professional help when indicated.
The original program, which was established in 1990 at a state hospital, provided needed support to employees (
5). It was also found to be associated with a sharp decline in violence within six months after its implementation. However, because only one hospital was involved, the first study was inconclusive about the associations between ASAP and the decline in violence.
Guided by the principle of program evaluation to ensure high-quality, cost-effective care, the Massachusetts Department of Mental Health decided to implement ASAP in three additional state hospitals. The purpose of the study reported here was to examine the effects of the program on the number of assaults in three public-sector hospitals over a one-year period.
Methods
After ASAP was established in 1990 in a state hospital, it was next implemented in a staggered start-up in three state mental hospitals during 1994 and 1995. The staggered start-up permitted the use of a multiple-baseline design in this phased-in approach. In this design each hospital served as its own control group. ASAP was started at the three hospitals at three-month intervals to assess any possible declines in the frequency of assaults in each facility after ASAP was implemented.
Hospital A was a 175-bed facility with 261 direct care staff on five units. Hospital B was a 175-bed facility with 295 direct care staff on ten units. Hospital C was a 190-bed site with 384 direct care staff on eight units. Patients were primarily white (87 percent). They ranged in age from 22 to 77 years old, and most were between 30 and 40 years old.
Most patients (85 percent) were diagnosed as having a thought disorder (85 percent). Others had an affective disorder (10 percent) or another diagnosis (5 percent). The patients were primarily continuing care patients, with a mean length of inpatient stay of 180 days. Nearly all patients (90 percent) were involuntarily committed, and 90 percent were uninsured. There were no acute care or incarcerated forensic patients at these facilities. Patient characteristics were similar in each hospital. During the study, no statistically significant changes were noted at any of the three facilities in patients' age, diagnosis, and length of stay or in the number of admissions and discharges, the daily census, and the patient mix.
Before ASAP was implemented, each facility provided employees with access to clinical services for patients who were assaultive, including conferences on patients at risk of being assaultive; medication, behavioral, and forensic consultations; and ongoing staff development programs in clinical skills. All staff were routinely trained in the same systems of nonviolent self-defense, restraint and seclusion procedures, and effective communication with patients. Before ASAP was implemented, no formal support was provided to employee victims to address psychological sequelae of assaults.
This study focused only on physical assaults, which can be the most dangerous type of assault and the most disruptive to staff. Assaults were defined as unwanted physical contact with intent to harm, including punching, kicking, slapping, biting, spitting, and throwing objects at persons. The unit of analysis for the study was each assault. Each incident of assault was either directly observed by a staff member, or if it was not observed, the victim was assessed by a staff member shortly after the incident. The severity of the assault was not rated.
Baseline data on assaults in each facility were compiled for the three months before ASAP was implemented. For two of those months, data were gathered from administrative reports. To assess the validity of the data in the administrative reports, incident report forms with specific operational definitions and examples of assaults were distributed to each unit for use during a third month. Staff were instructed to record all episodes of assault. Data from this period did not differ from data obtained from the administrative reports, and data for the three months were combined to calculate a base rate. To safeguard against underreporting of assaults after ASAP was implemented (
10), the charge nurse on each unit was required to notify ASAP staff after every assault, file a written report, and discuss the assault at hospitalwide nursing rounds.
ASAP team leaders and staff were recruited from volunteers. Each team was trained in the standardized ASAP format of materials on psychological trauma and intervention procedures (
4).
Results
Between April 1994 and August 1995, ASAP teams in the three facilities responded to 125 episodes of assault. Victims accepted assistance in 109 cases (80 percent). No differences were found in the types or amounts of clinical support services for assaultive behavior, such as patient-at-risk conferences and medication consultations, before and after program implementation.
In hospital A in April 1994 a total of 168 patients committed 21 assaults, for an average of 5.25 assaults per week and a rate of .13 assaults per 100 patients per month. In March 1995 a total of 165 patients committed one assault, for an average of .2 assaults per week and a rate of .01 assaults per 100 patients per month. The patient-staff nursing ratio was 1 to 1.55 in April 1994 and 1 to 1.33 in March 1995.
In hospital B in May 1994 a total of 173 patients committed 39 assaults, for an average of 7.8 assaults per week and a rate of .23 assaults per 100 patients per month. In April 1995 a total of 155 patients committed five assaults, for an average of 1.25 assaults per week and a rate of .03 assaults per 100 patients per month. The patient-staff nursing ratio was 1 to 1.71 in May 1994 and 1 to 1.67 in April 1995.
In hospital C in August 1994 a total of 186 patients committed 33 assaults for an average of 6.6 assaults per week and a rate of .18 assaults per 100 patients per month. In July 1995 a total of 187 patients committed three assaults for an average of .75 assaults per week and a rate of .02 assaults per 100 patients per month. The patient-staff nursing ratio was 1 to 2.05 in August 1994 and 1 to 1.92 in July 1995.
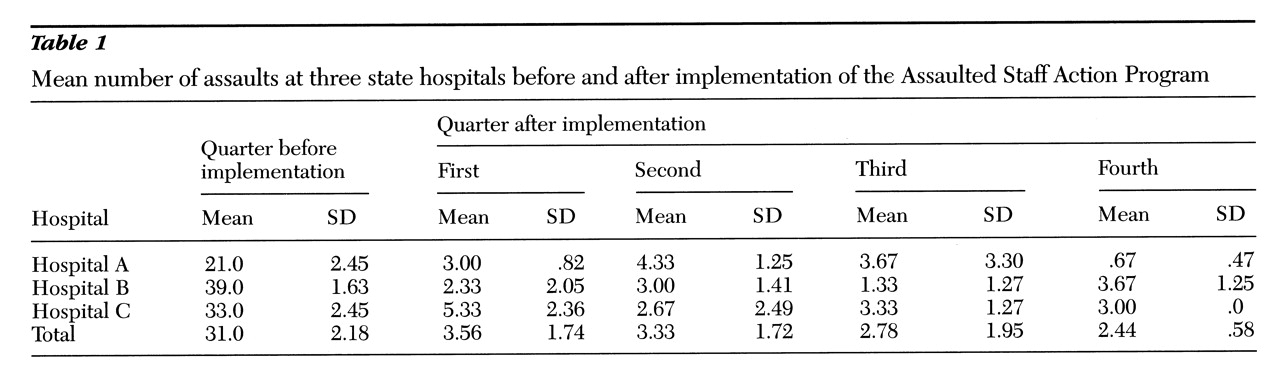
Table 1 presents the mean number of patient assaults on staff per quarter before and after implementation. The rate of assaults did not vary by hospital and declined in each facility after implementation of ASAP. A repeated-measures analysis of variance showed a statistically significant difference in the number of assaults between the quarters before and after implementation (F=80.85, df=4,40, p<.001). Post hoc Dunnett's tests revealed no significant differences in the number of assaults between the first and other quarters after the program was implemented.
Discussion and conclusions
This exploratory study demonstrated replications of declines in violence after the Assaulted Staff Action Program (ASAP) (
4,
5) was implemented in three additional facilities. Although the multiple-baseline design provided some control for frequency of assaults, formally controlled experimental studies are needed to identify possible factors accounting for declines in violence.
In addition to examining the effects of the program and its components, future studies should examine the possible contributions of halo effects, staffing factors, and medication and management consultations. The severity of assaults, the extent of injuries sustained, and the continuing problem of underreporting (
10) also require additional assessment.
Growing evidence suggests that ASAP may be associated with declines in the frequency of assault. The findings reported here provide three additional replications of the original findings (
5) of a decline in assault rates; however, this study did not address the possible mechanisms for these declines. Therefore, we can only speculate on what program factors may be associated with assault reduction. For example, a prompt hospitalwide response by program staff may restore a sense of mastery and attachment in employee victims or transform the meaning of the work environment from indifference to support. Similarly, the existence of the program may reduce staff members' anxiety and therefore patients' anxiety, a process that may raise the threshold for violence. The program may also improve staff's attention to early warning signs of loss of control and result in preventive de-escalation interventions. These hypotheses are the focus of ongoing inquiry.