An increased risk of violence among patients with schizophrenia has been repeatedly confirmed by evaluation of criminal records (
1,
2,
3,
4), a twin study (
5), and recently in a large sample of persons who committed homicide (
6). In all Western countries, the increased risk of violent crimes among patients with schizophrenia is demonstrated by the fact that they account for about half of all patients in forensic detention because of insanity (
7).
The studies cited so far were all based on criminal records. However, many aggressive acts among patients with schizophrenia take place within the family (
8,
9) or during inpatient treatment and therefore do not appear in the criminal statistics, as long as the acts of violence are not severe. Ten to 45 percent of patients with schizophrenia exhibit aggressive or threatening behavior during hospitalization (
10,
11,
12,
13). According to several studies, aggressive behavior among inpatients with schizophrenia seems to be more frequent than among inpatients with other diagnoses (
14,
15,
16,
17,
18,
19). However, the samples in these studies were highly selected groups of patients that were not well defined diagnostically. In addition, there is some evidence that self-directed violence and suicidality are frequent complications among patients with schizophrenia (
20). No study of the frequency of aggressive behavior against self and others has been carried out on a representative and well-defined clinical sample of patients with schizophrenia.
Results of studies of gender differences in aggressive behavior among patients with schizophrenia are contradictory. Males with schizophrenia commit severe acts of violence more frequently than females (
1,
2,
3,
4). However, the difference does not appear as pronounced with acts of minor severity. Some researchers have reported that less severe aggression is more frequent among women with schizophrenia than among men with the disorder (
19,
21,
22,
23), whereas others have found no gender differences in aggression among patients with schizophrenia (
11,
14,
16,
24,
25). Studies that have categorized the violent acts of these patients based on severity have found no significant gender differences (
26,
27).
The significance of substance abuse as an independent risk factor for violence among patients with schizophrenia has been confirmed in several studies (
28,
29). However, in most of the studies, no differentiation between alcohol and drug abuse was made.
Some authors have concluded that aggressive patients with schizophrenia are younger than nonaggressive patients(
8,
11,
13,
16,
30,
31); however, others have found contradictory evidence(
5,
24,
25).
Little research has focused on the question of whether patients with schizoaffective psychoses exhibit aggressive behavior more often than patients with schizophrenia. Only Grossman and associates (
32) have focused on this problem. They found that patients with schizoaffective disorder were significantly more likely than those in the other diagnostic groups (schizophrenia, bipolar affective disorder, and unipolar affective disorder) to have been arrested for a violent crime.
Furthermore, some evidence indicates that aggressive behavior by patients with schizophrenia predicts longer and more frequent hospitalizations (
9,
27,
33). However, these results were found only in selected groups of patients.
Thus answers to many questions about violence among patients with schizophrenia are inconsistent, mainly because of selected samples. On the basis of the studies reviewed, some hypotheses were established for testing in a diagnostically well-defined clinical sample of first-episode patients. The first hypothesis is that aggressive behavior against others occurs frequently among patients with schizophrenia. However, such behavior is not severe, for the most part, and only rarely leads to legal prosecution. The second hypothesis is that no gender differences exist in the frequency or severity of aggressive behavior among these patients.
The third hypothesis is that patients with schizoaffective disorder behave aggressively more often than those with purely schizophrenic psychoses. Fourth, it was hypothesized that a negative association would be found between age and the tendency to violence among patients with schizophrenia. The fifth hypothesis is that substance abuse is a predictor of violence in patients with schizophrenia. The sixth is that aggressive behavior against others correlates with more frequent and longer hospitalization.
In addition to these hypotheses, the study examined predictors of violent behavior and of the number and duration of hospitalizations.
Methods
Sample
This retrospective study was carried out at the Weissenau Center for Psychiatry, a university-affiliated hospital in southern Germany with a catchment area of about 460,000 inhabitants. No other psychiatric inpatient services exist in this predominantly rural area. Hospitals in the Federal State of Germany (Baden-Württemberg) are not allowed to provide outpatient services. The center is closely connected with all complementary outpatient services. Patients with psychotic disorders are admitted to one of four similar units. For subsequent admissions, most patients are treated on the same unit. The hospital also has a forensic unit. Patients under 18 years old are treated in a child and adolescent unit.
For inclusion in the study, an individual had to have received inpatient treatment of a first episode of schizophrenia or schizoaffective disorder (ICD-9 code 295.x) at the hospital between January 1, 1990, and December 31, 1993. A total of 471 patients met this criterion. In each case, a chart review was conducted to re-evaluate the diagnosis based on ICD-10 criteria. Doubtful cases were excluded. Most of the excluded cases did not meet criteria related to duration of illness (for example, continuous signs of the disturbance for at least one month). Other patients were excluded because they lived outside of the catchment area, had had previous psychiatric or psychotherapeutic treatment in other inpatient services, were under 14 years old or over age 60, or had an additional diagnosis of a progressive organic brain disease.
After strict application of the exclusion criteria, a sample of 138 patients was obtained (77 men and 61 women).
Instruments
Primary and secondary diagnoses were re-evaluated based on ICD-10 criteria according to information documented in patients' charts. Although alcohol and drug abuse and dependence were evaluated separately, no distinction was made in the analyses between abuse and dependence.
Aggressive behavior as documented in the charts was recorded, including all staff documentation in handwriting, ranging from one to five notes a day. Seven different areas of possible manifestations of violence were noted: threats of violence in connection with the first admission (that is, as a reason for admission), violence in connection with the first admission, violence against persons during the first hospitalization, violence against objects during the first hospitalization, threats against others during subsequent hospitalizations in the next two years, violence against persons during subsequent hospitalizations, and violence against objects during subsequent hospitalizations. Furthermore, reactions to patients' aggressive or agitated behavior were divided into four categories—involvement of the police, seclusion, restraint, or involuntary medication.
To calculate statistical associations, the use of a dimensional measure of violence was necessary. A simple subdivision into violent and nonviolent patients is methodologically unsatisfactory and does not correspond to clinical reality (
34). We used the Modified Overt Aggression Scale (MOAS) (
35), a modified version of the Overt Aggression Scale developed by Yudofsky and colleagues (
36). For all 138 patients, chart reviewers obtained information about the most severe acts of aggression during the first admission in four categories: verbal aggression, aggression against objects, aggression against self, and aggression against persons. The same information was obtained for the 83 patients who were rehospitalized during the next two years.
The MOAS rates the most severe act in each of these categories. A score from 1 to 4 is assigned to each act; higher scores indicate greater severity. The score in each category is multiplied by a factor assigned to each category: 1 for verbal aggression, 2 for aggression against objects, 3 for aggression against self, and 4 for aggression against other people. Thus the maximum total score is 40. We examined self-directed aggression separately. Therefore, the maximum score was 28.
The number of hospitalizations (counting the index hospitalization) and the total number of hospital days during the two years (including the index hospitalization) were calculated from hospital records.
Statistical methods
Contingency tests were carried out using t tests for continuous variables and the chi square test for categorical variables. For data on an ordinal scale, the Mann-Whitney U test was employed. Correlations between continuous variables were tested using Pearson's correlation coefficient. When different predictor variables had to be checked against a dependent variable, stepwise multiple regression was used. The term "predictor" is used here in a mathematical sense and does not imply any conclusions about causal correlations. The significance level was set at .05.
Results
Sample characteristics
Of the 138 patients in the sample, 109 patients (79 percent) were diagnosed as having a paranoid type of schizophrenia (ICD-10 F 20.00 through F 20.09). Two patients had a disorganized type (F 20.10, F 20.13), and five had an undifferentiated type (F 20.31 through F 20.39). Twenty-two patients received a diagnosis of schizoaffective disorder; six had a schizomanic form of the disorder (F 25.0), ten had a schizodepressive form (F 25.1), four had a mixed form (F 25.2), and two had a form classified as "without further description" (F 25.9).
Forty-one patients (28 percent) had secondary psychiatric diagnoses, especially substance abuse. An accompanying somatic disease was diagnosed for 29 patients (21 percent). The mean±SD age at first admission was 32.4±12.7 years. The men were significantly younger than the women (30.2±11.3 years versus 35.3±13.7 years; t=2.405, df=136, p=.018).
A total of 117 patients were Germans, three were Germans raised in Eastern Europe who had immigrated to Germany, and 18 were from foreign countries. Ninety-two patients (67 percent) were single, 31 (23 percent) were married, 14 (10 percent) were divorced, and one was widowed.
Forty of the patients (29 percent) did not have professional training, 72 (52 percent) had completed an apprenticeship, seven (5 percent) had a university degree, and nine (7 percent) were still in training; for ten patients this information was missing. However, at the time of first admission, only 40 of the patients were working, 34 were in training or occupied as housewives, and 57 did not have an occupation.
For the 138 patients, the mean±SD number of hospital admissions during the two years (including the first admission) was 1.88±1.1, with a range from one to five admissions. The mean±SD number of hospital days was 130.4±138.2, with a range from three to 722 days. There were no gender differences in these variables.
Frequency of aggressive behavior
Reports of some form of aggressive behavior were made in the charts of 96 patients (70 percent). Ninety patients (65 percent) exhibited aggression against others—58 of the men (75 percent) and 32 of the women (53 percent) χ2=7.845, df=1, p=.005). No patient was involved in a violent offense leading to forensic detention.
Twenty-nine patients (21 percent) attempted suicide during the two-year study period—17 percent of the men and 26 percent of the women. Thirty-six patients (26 percent) made suicide threats—22 percent of the men and 31 percent of the women. Neither of the gender differences were significant.
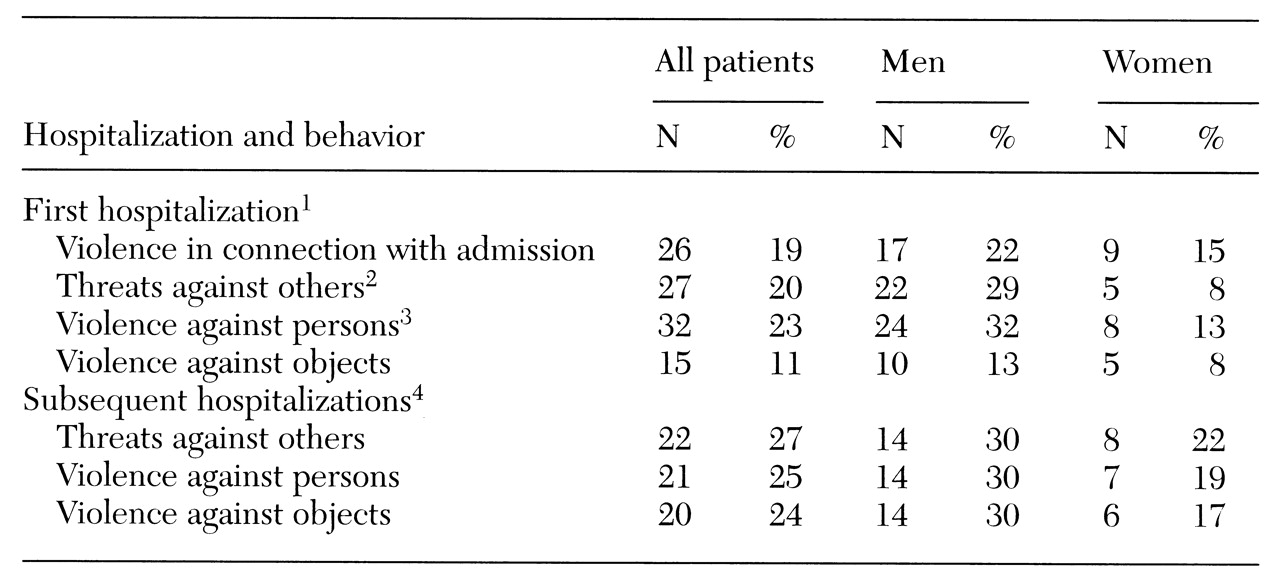
Table 1 gives an overview of the various manifestations of aggressive behavior as documented during the first hospitalization and during any hospitalizations in the following two years. During or just before the first hospitalization, about a fifth of the patients acted aggressively, either threatening violence or becoming involved in aggression against others.
Eighty-three of the patients (60 percent) were rehospitalized in the two years after the first admission; 47 men were rehospitalized and 36 women. For about a fourth of the rehospitalized patients, aggressive acts were documented in the charts. As
Table 1 shows, both threats and violence against persons were significantly more frequent among men.
Aggressive behavior against others documented during the first hospitalization predicted the behavior during the subsequent two years. Patients who exhibited this behavior during the first hospitalization were significantly more likely than other patients to have such behavior documented in their charts during subsequent hospitalizations χ2=4.294, df=1, p=.038). This association was even stronger for threats of violence χ2=3.765, df=1, p=.003).
Several responses occurred in reaction to patients' behavior either in the community or during hospitalization. Fifty-seven patients (41 percent) were involuntarily hospitalized as a result of aggressive behavior. In 51 cases (37 percent) police were contacted. Among hospitalized patients, 30 (22 percent) were placed in seclusion, seven (5 percent) were restrained, and 26 (19 percent) were involuntarily medicated. The only significant gender difference was in the area of legal prosecution; 13 of the 77 men (17 percent) and two of the 61 women (3 percent) were prosecuted for aggressive behavior χ2=6.502, df=1, p=.011).
Severity
Most of the aggressive behavior was not severe. Only one patient was involved in an assault against a person that resulted in severe injuries (MOAS category 4d). However, 15 men (20 percent) and four women (7 percent) were involved in aggressive behavior that resulted in minor injuries (MOAS category 4c). The gender difference was significant χ2= 4.788, df=1, p=.029).
Seventeen men (22 percent) and seven women (12 percent) made murder threats (MOAS 1d). Eight men (10 percent) and five women (8 percent) were involved in severe aggression against objects (MOAS 2d). None of the patients committed suicide, despite the high frequency of attempts. Mean±SD total scores on the three MOAS categories measuring aggression against others (verbal aggression, aggression against objects, and aggression against persons) were 8.69±8.02 for men and 4.47±6.27 for women (t=3.365, df=136, p<.001).
Aggression against self or suicidal behavior (the other MOAS category) was not significantly correlated with any of the three MOAS measures of aggression against others.
Predictors
The number of hospitalizations was significantly predicted by three variables: the total number of hospital days (beta=.35, p<.001), a correlation that is obvious; aggressive behavior against others (beta=.16, p=.03); and aggressive behavior against self (beta= .19, p=.01). Age, gender, a diagnosis of schizophrenia or schizoaffective disorder, alcohol abuse, drug abuse, marital status, employment, and social status did not predict hospitalization.
Significant predictors of the total number of hospital days were the number of hospitalizations (beta=.36, p<.001), never having been married (beta=.23, p=.005), and alcohol abuse (beta=-.24, p=.007). The other variables were not associated with the duration of hospitalization.
Finally, we determined predictors of aggression against others as measured by scores on three of the four MOAS categories (self-directed aggression was not included). Significant predictors were male gender (beta=.22, p=.009), number of hospitalizations (beta=.20, p=.014), and alcohol abuse (beta=.19, p=.026). However, these variables explained only 16 percent of the variance in aggression against others. The other variables examined did not predict aggression against others, including a diagnosis of schizophrenia or schizoaffective disorder, marital status, professional training, employment at the time of first admission, drug abuse, age, and aggressive behavior against self or suicidal behavior.
Discussion and conclusions
The results of this study contribute to an understanding of the epidemiology of aggressive behavior among patients with schizophrenia. For the first time, a clearly defined first-episode sample was examined in terms of violent and aggressive behavior against others and self.
This study addressed several hypotheses. The first was that aggressive behavior against others occurs frequently among patients with schizophrenia, but that it is for the most part not severe and only rarely leads to legal prosecution. Nearly two-thirds of the patients in this two-year study exhibited some form of aggressive behavior. Although some authors have recently postulated that comorbid factors such as personality disorders and substance abuse, rather than the illness itself, are the cause of violent behavior among patients with schizophrenia (
37), the high frequency of aggressive behavior against self and others in our sample supports the assumption of an illness-related cause.
Most of the recorded aggressive behavior was not severe. About one in six patients made murder threats, and one in five men and one in 16 women committed assaults that resulted in minor injuries. No patient was held in forensic detention. Forensic detention of patients with schizophrenia typically occurs only after a course of illness of several years, with increasing social disintegration (
38). The families of the patients in our study appeared to be exceptionally tolerant of their behavior. Because of such tolerance, evaluations of criminal records give a very incomplete picture of violent behavior.
The second hypothesis was that no gender differences would be observed in the frequency or severity of aggressive behavior. This hypothesis must be rejected. During the two-year study, 75 percent of the men in this sample but only 53 percent of the women exhibited aggressive behavior. Two forms of violence associated with the first hospitalization were significantly more frequent in men—verbal threats (29 percent of men and 13 percent of women) and aggressive behavior as a reason for admission (32 percent of men and 13 percent of women). Severity scores on the four MOAS types of aggression also indicated highly significant gender differences. It is likely that earlier studies that found no gender differences in violence among these patients or that found women to be more aggressive (
11,
14,
16,
19,
21,
22,
23,
24,
25) were biased by highly selected samples.
The third hypothesis was that patients with a schizoaffective disorder would exhibit aggressive behavior more often than those with purely schizophrenic psychoses. This hypothesis was not supported by the data, which may be due to the small number of patients with schizoaffective disorder in the study.
The fourth hypothesis was that a negative association would be found between age and the tendency to violence among patients with schizophrenia. This hypothesis also was not supported by the findings. Age at admission did not predict violence; however, a tendency in this direction was noted (p=.15). Although an association between younger age and violence exists in the general public, this association seems to be weaker for patients with schizophrenia (
5,
24,
25).
The fifth hypothesis was that substance abuse would be a predictor of violence in this patient group. This hypothesis was partly supported by our findings. Alcohol abuse was significantly associated with violence during the two years after first admission. However, this association applied only to men. An association between violence and drug abuse could not be found in our sample. One reason could be the relatively low prevalence rates of drug abuse among psychotic patients in our region (11 percent in the study sample).
The final hypothesis was that aggressive behavior against others would correlate with more frequent and longer hospitalization. Our results provided some evidence that aggressive behavior against others may well be associated with more frequent rehospitalizations, but no association with the duration of hospitalization was found. It may be a case of two tendencies neutralizing each other: on the one hand, aggressive behavior obviously leads to an increased likelihood of hospitalization, but on the other hand, these patients may have stronger tendencies to be noncompliant and to leave the hospital against medical advice.
A piece of circumstantial evidence supporting this speculation is the role of alcohol abuse, which was found to be associated with violence, on the one hand, and with significantly shorter stays, on the other. In this respect, patients with dual diagnoses seem to have some of the characteristics of patients in treatment for substance abuse—short stays, frequent relapses, poor compliance, and a revolving-door pattern of care (
39). Thus the association found between the number of hospitalizations and the total number of hospital days is not trivial or simply obvious, but reveals characteristic associations in particular groups of patients.
Furthermore, use of multiple regression allowed us to examine which of the other variables besides rehospitalization contributed to the total number of hospital days. It is remarkable that in the two years after the first episode of illness, the only variables associated with rehospitalization were aggressive behavior against self and others. These results add further details to the associations between violent behavior and hospitalization suspected in previous studies (
9,
27,
33).
The limitations of the study reported here are mainly related to its retrospective design. Although chart documentation at the hospital is generally good, the frequency of aggressive behavior, especially of minor severity, may have been underestimated. On the other hand, because violent patients are frequently uncooperative or unreliable in answering questions in prospective studies, chart review allowed us to use an unselected sample. To the extent that prospective clinical studies exclude violent patients, they will also underestimate the problem.
Further limitations are related to the sampling procedure. The study was carried out at a single facility. Specific hospital practices and regional characteristics, such as the lack of large cities, may have influenced the results. Excluding subjects without a confirmed diagnosis of schizophrenia, especially those who failed to meet diagnostic criteria for duration of illness, may have resulted in a sample of patients with more severe courses of illness. Therefore, the results should not be generalized without caution. However, given the methodological limitations, it is more likely that the results underestimate rather than overestimate the frequency of violence among patients with schizophrenia.
Despite the study's limitations, the results provide evidence that aggressive behavior against self and others is a frequent and often dangerous symptom of schizophrenia and that it plays a major role in rehospitalization.