The pathogenesis of depression may involve the circuit from the prefrontal cortex, to the striatum, to the globus pallidus and substantia nigra, to the mediodorsal thalamus, and back to the prefrontal cortex
(1). Disturbances in this circuit could cause mood disorders. Studies of neurodegenerative diseases
(2), striatal lesions
(3), and functional neuroimaging
(4) suggest striatal involvement in mood disorders. Using structural magnetic resonance imaging (MRI), a group of researchers found lower than normal caudate
(5) and putamen
(6) volumes in subjects with unipolar depression. The same group
(7) replicated these findings. However, three studies by different groups
(8–
10) did not find that caudate volume was significantly lower in subjects with unipolar depression. A study of patients with bipolar disorder
(11) showed no caudate or putamen volume differences in women and significantly higher volumes in men. Subject differences could partly account for this variability, as could different measurement methodologies or insufficient power in the negative studies.
In the current study we measured striatal volumes in subjects with major depression and matched comparison subjects, who, in contrast to previous studies, had been screened to exclude major cerebrovascular disease risk factors.
METHOD
Subjects were recruited from the outpatient psychiatry services of Washington University. Using the Diagnostic Interview for Genetic Studies
(12), a psychiatrist (Y.I.S.) confirmed the diagnosis of recurrent nonpsychotic major depression. Subjects were screened by questionnaire, medical history, medical records, and physical examination and excluded if they had other psychiatric conditions or conditions potentially affecting the central nervous system
(13). Subjects with acute worsening of depression within 4 months were excluded. All subjects gave written informed consent. To decrease the risk of including subjects with cerebrovascular disease risk in the study, we chose all female subjects. Female comparison subjects, recruited from the community, had no history of major depression. They were similarly medically screened and case-matched by age and education.
MRI scans used a magnetization-prepared rapid-gradient echo sequence to acquire images. T
1 image parameters were 256 by 256 pixel matrix, 1 by 1 mm voxel size, and 1.25 mm slice thickness. Images were processed with ANALYZE software
(14).
Scans were reviewed with a neuroradiologist to determine measurement rules (available on request). Volumes were determined stereologically. A rater who was blind to subject identity measured caudate and putamen volumes twice to ensure reliability; the mean was used in data analysis. Another rater measured 10 of each structure twice to check interrater reliability. Intraclass correlation coefficients were 0.97 or greater for both structures.
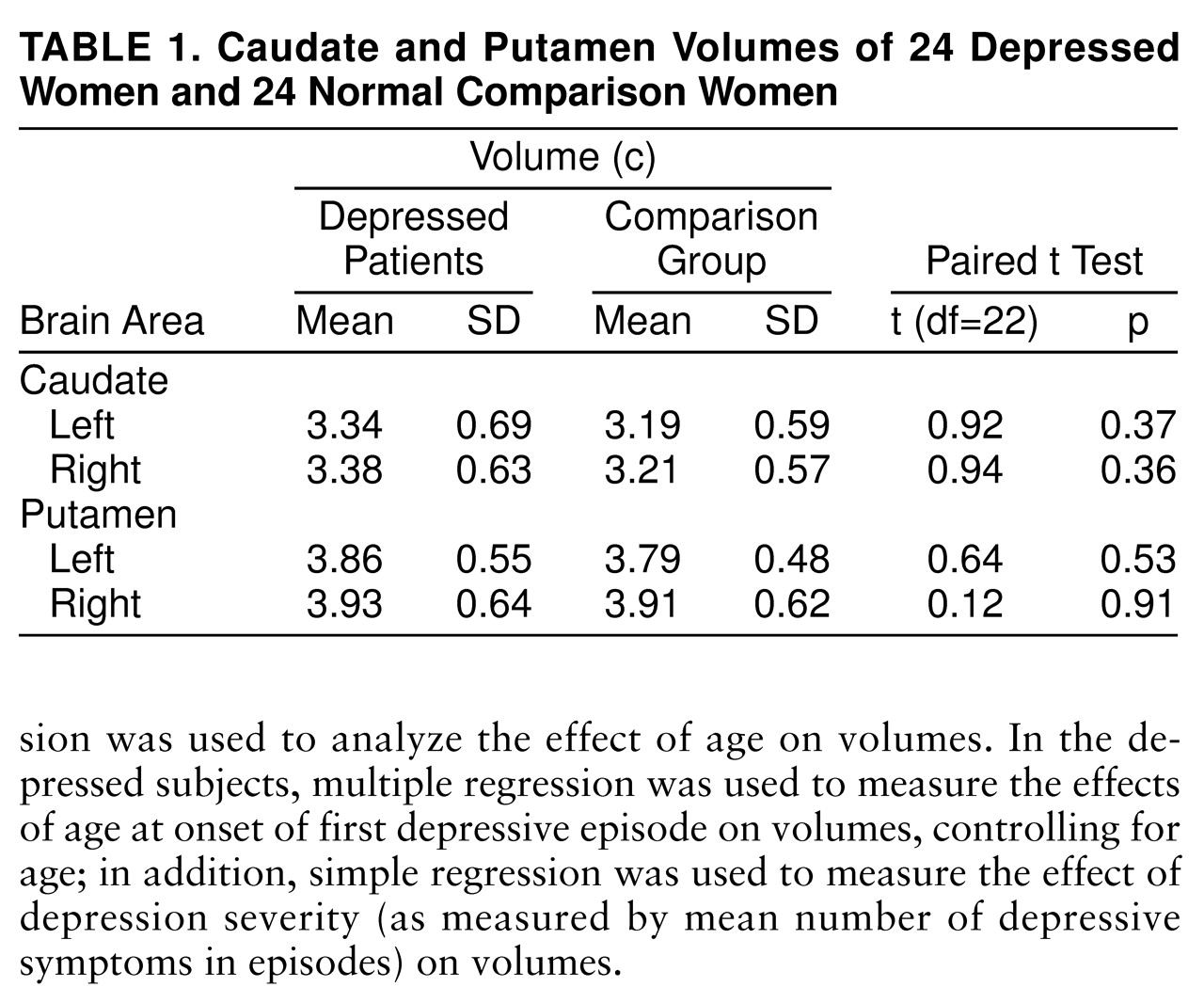
Data were compiled for left and right caudate and putamen volumes. Paired t tests were used to compare the groups. Linear regression was used to analyze the effect of age on volumes. In the depressed subjects, multiple regression was used to measure the effects of age at onset of first depressive episode on volumes, controlling for age; in addition, simple regression was used to measure the effect of depression severity (as measured by mean number of depressive symptoms in episodes) on volumes.
RESULTS
Subjects ranged in age from 24 to 86 years (mean=53 for each group). All of the depressed women had received psychiatric treatment, half had previous psychiatric hospitalizations, most were currently taking antidepressant medication, and nearly all had past suicidal ideation.
There were no significant differences between the depressed and nondepressed women in caudate or putamen volumes (
table 1).
There was no effect of age on total caudate volume (standard coefficient=0.10, t=0.66, df=46, p=0.51) and a small positive effect of age on total putamen volume (standard coefficient=0.36, t=2.64, df=46, p=0.01). In the depressed women, there was no effect of age at onset, controlling for age, on either caudate (standard coefficient=0.27, t=0.88, df=21, p=0.39) or putamen (standard coefficient=0.19, t=0.19, df=21, p=0.53) volumes. In addition, there was no effect of depression severity on either caudate (standard coefficient=0.14, t=0.65, df=22, p=0.53) or putamen (standard coefficient=0.17, t=0.81, df=22, p=0.43) volumes.
DISCUSSION
This study found no volumetric differences in caudate and putamen in depressed women compared with nondepressed women. In addition, there was no effect of age, age at onset, or depression severity on volumes except for a putamen volume increase with age.
These findings contrast with those of earlier reports
(5–
7), which showed smaller striatal structures in depressed subjects and decreased caudate volume with age. This study has 80% power to find an 8% difference in caudate or putamen volumes
(15) and more than 99% power to find differences on the magnitude of previous studies
(5,
6). Therefore, this study’s negative result was not likely due to insufficient power. It is unlikely that methodological problems explain earlier positive results because they have been replicated; all studies used the same stereological measurement methodologies; and the structures are relatively unambiguous to measure.
Differences in inclusion criteria may account for differences in findings between this study and previous studies. Our subjects, unlike those in previous studies, were extensively screened to exclude major cerebrovascular disease risk factors. Although some subjects had white matter hyperintensities, possible evidence of small vessel disease, none had cerebrovascular disease by history, physical examination, or MRI findings. This may explain the absence of an age effect on caudate size in this study. Subjects in previous studies may have had substantial cerebrovascular disease and consequent atrophy of brain structures, which may explain smaller whole brain volumes and various cortical and subcortical volumes in depressed subjects
(5,
7). Thus, greater cerebrovascular disease load in depressed subjects may have accounted for previous findings.
Another possibility is difference in depression severity; possibly, subjects with more severe depression would be more likely to have smaller striatal volumes. However, depression severity in this study was not a significant predictor of volumes and appears similar to that in previous reports
(5).
In our study, none of the women had a history of psychosis, although two had past neuroleptic exposure (less than 1 week). In contrast, one previous study
(5) described 18 of 50 subjects as having previous neuroleptic exposure. Neuroleptic exposure is unlikely to cause smaller striatal volumes; it may increase caudate volume
(16). However, possible inclusion of subjects with psychotic depression in previous reports could contribute to differences in results.
Longitudinal imaging studies will be valuable in ascertaining what, if any, striatal changes occur in mood disorders. Ultimately, neuropathological studies are needed to determine striatal pathology and help define its role in mood regulation.