Most neuroimaging studies of adult posttraumatic stress disorder (PTSD) have sought to reduce possible alcoholism-related confounders but have ultimately relied on comparisons in which the PTSD groups reported more alcohol exposure than the comparison subjects
(1 –
7) . Conversely, studies that have rigorously excluded comorbid alcohol abuse/dependence have usually not found smaller hippocampal volumes
(8 –
12, but see
13 ). Smaller hippocampal volumes have also been reported in individuals with primary alcohol abuse/dependence
(14 –
17), and although this effect rarely persists after adjustment for global tissue volume
(18 –
21), there is a consensus that comorbid alcohol abuse/dependence is relevant to a complete understanding of the neurobiology of PTSD. A common approach to the problem of comorbid alcoholism has been to adjust brain volumes for lifetime consumption
(3 –
6) ; however, the alcohol literature shows a scarcity of linear relationships between consumption and indices of brain structure or function
(22 –
27) . This scarcity could derive from the low reliability of retrospective self-reports
(28 –
30) and/or the possibility that binge/withdrawal episodes, rather than “typical” drinking, account disproportionately for alcohol-related brain damage
(31) . To overcome these limitations, we recruited subjects from two large VA catchments with the aim of accruing a substantial number of participants diagnosed free of lifetime alcohol abuse/dependence
(32) .
One proposed explanation for the absence of smaller hippocampal volumes in groups that did not confounding PTSD and alcoholism is that their subjects have often been children and adolescents. To provide a partial test of this hypothesis, we compared Vietnam and Gulf War veterans with mean ages of 56 and 38 years and mean years since military trauma of approximately 36 and 9 years, respectively. Numerous effects of aging on brain morphometry have been documented
(33 –
37) . Because aging was confounded with other factors known to influence PTSD, including trauma severity and socioeconomic status, the term “cohort” was used.
Results
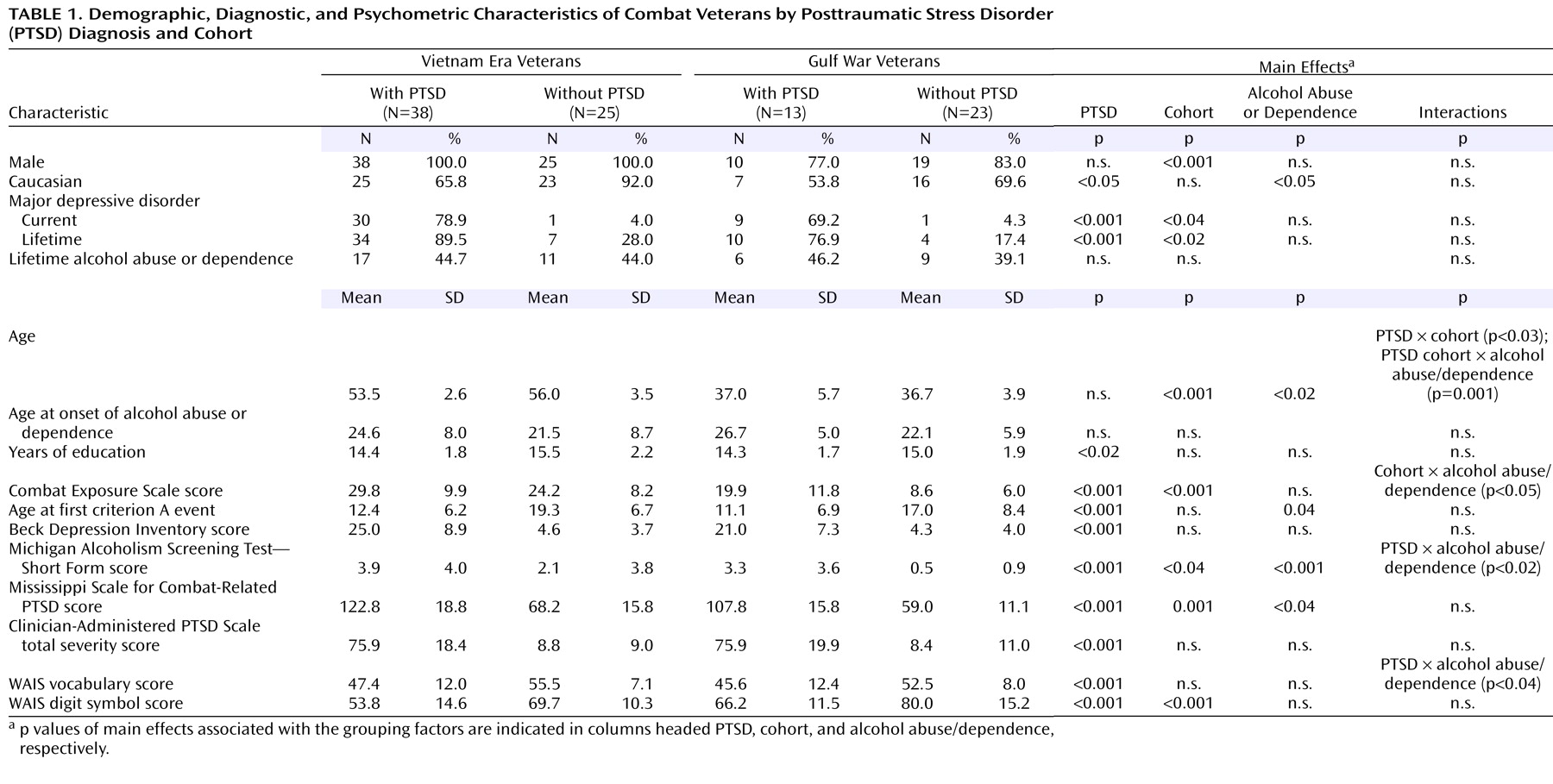
Combat-related PTSD was strongly associated with comorbid major depression, elevated Beck Depression Inventory scores, and reduced WAIS vocabulary scores. PTSD-positive subjects also performed much worse on the WAIS digit symbol substitution subtest (F=25.5, df=1, 91, p<0.001). Because of oversampling, PTSD was not associated with an elevated frequency of alcohol abuse/dependence; nevertheless, Michigan Alcoholism Screening Test—Short Form scores exhibited both a main effect of PTSD and a PTSD-by-alcohol abuse/dependence interaction deriving from especially high scores in PTSD-positive, alcohol abuse/dependence-positive subjects. Even within the alcohol abuse/dependence-negative subgroup, PTSD was associated with a small but significant elevation of Michigan Alcoholism Screening Test—Short Form scores (PTSD-positive subjects: 1.19, PTSD-negative subjects: 0.18). Generally speaking, the alcohol abuse/dependence-positive and alcohol abuse/dependence-negative subgroups were closely matched, and PTSD and alcohol abuse/dependence did not interact to influence psychometric indices. Being alcohol abuse/dependence-positive was not associated with an elevated incidence of major depressive disorder and did not interact with other factors to influence a diagnosis of major depressive disorder. Being alcohol abuse/dependence-positive was also not associated with an elevated Beck Depression Inventory score or an elevated Combat Exposure Scale score. Alcohol abuse/dependence-positive subjects did not differ in years of education and did not exhibit worse performance on the WAIS digit symbol substitution subtest. In contrast, Gulf War and Vietnam cohorts exhibited large differences in combat exposure, current PTSD severity, and digit symbol substitution performance. The former were consistent with the differing conditions of the two conflicts and the known impact of trauma severity on PTSD
(53) and the latter with normal aging
(54) . The Vietnam cohort also exhibited more lifetime major depressive disorder and higher scores on the Michigan Alcoholism Screening Test—Short Form.
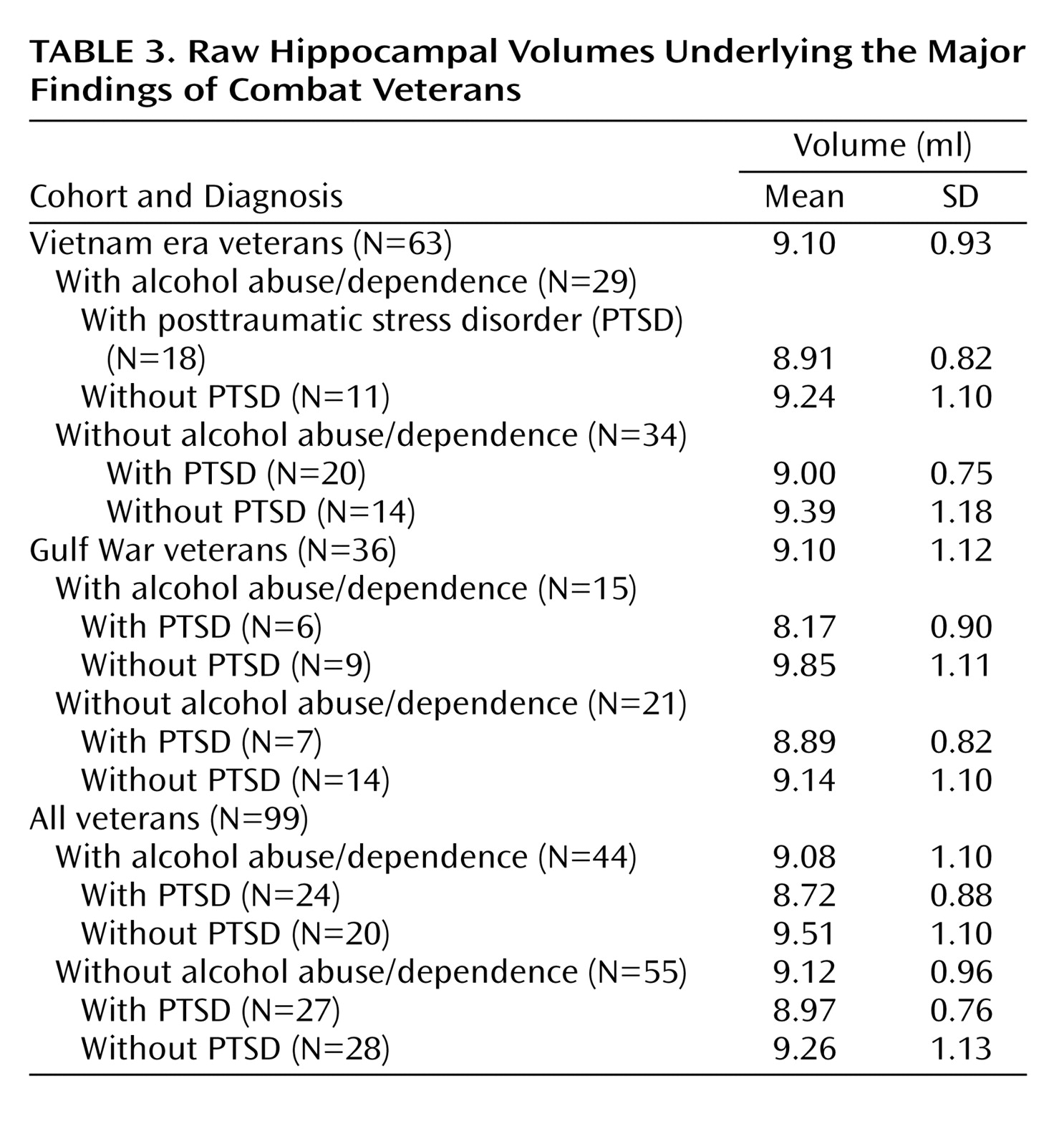
A three-factor multiple analysis of variance (MANOVA) (PTSD × cohort × alcohol abuse/dependence) performed on left and right hippocampal volumes found a significant multivariate F value for PTSD (F=4.89, df=2, 90, p=0.01). As well, the hippocampus was slightly larger in the right hemisphere (4.67 ml versus 4.44 ml; t=7.30, df=98, p<0.001), but this difference exhibited no interactions with grouping factors. Hence, group effects and interactions were reestimated on total hippocampal volume. (Although prior findings of smaller hippocampal volumes in PTSD have often been unilateral, no systematic directionality has emerged.) Mean unadjusted total hippocampal volumes are presented for all comparisons and for selected contrasts in
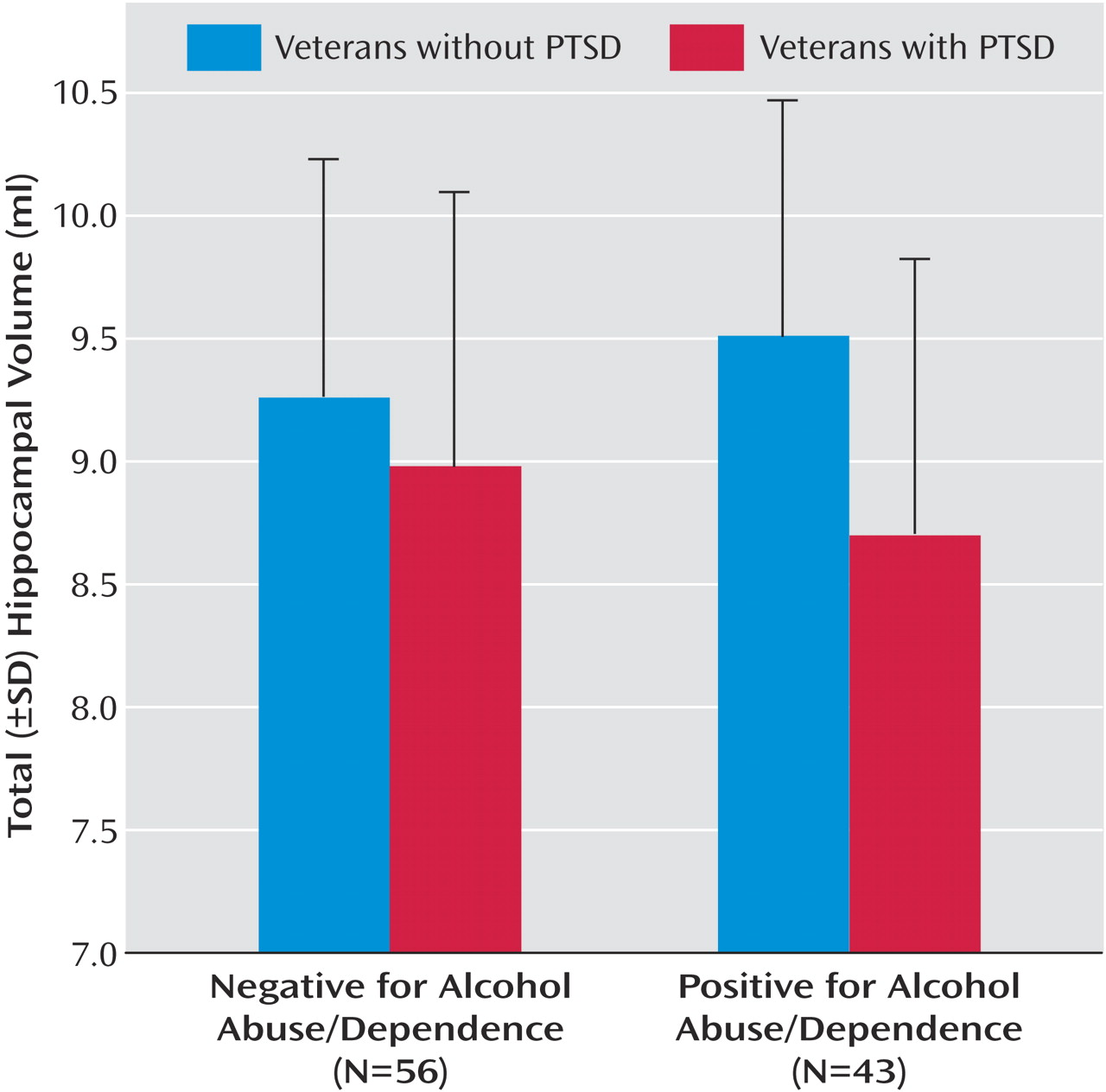
Table 3 . The main effect of PTSD on total hippocampal volume (F=9.83, df=1, 91, p=0.002) was accompanied by a near-significant two-way interaction of PTSD and alcohol abuse/dependence (F=2.69, df=1, 91, p=0.11) and a near-significant three-way interaction of PTSD, cohort, and alcohol abuse/dependence (F=2.87, df=1, 91, p<0.09). To account for the three-way interaction, PTSD and cohort interacted significantly in the alcohol abuse/dependence-positive subjects (F=4.63, df=1, 40, p<0.04) but not the alcohol abuse/dependence-negative subgroup. In the former, PTSD was associated with smaller hippocampal volume in the Gulf War cohort (9.85 ml versus 8.17 ml) but not in the Vietnam cohort (9.24 versus 8.91 ml). To account for the two-way interaction, the effects of PTSD on hippocampal volume varied in the alcohol abuse/dependence-positive and alcohol-dependence-negative subgroups. In the former, the hippocampal volumes of PTSD patients were 9% smaller than those of veterans without PTSD (8.72 versus 9.51 ml; F=10.44, df=1, 40, p=0.002). In the alcohol abuse/dependence-negative subgroup, hippocampal volume did not differ significantly between subjects with and without PTSD (8.97 ml versus 9.26 ml; F=1.25, df=1, 51, p=0.27) (
Figure 1 ), although the tendency (3%) was in the expected direction. Effect sizes were also estimated with pooled d+
(55) to accommodate the different numbers of Gulf War and Vietnam cohort members across PTSD-positive and PTSD-negative groups. In the alcohol abuse/dependence-positive subgroup, pooled d+ for the effect of PTSD on hippocampal volume was –0.69, with a two-tailed 95% confidence interval (CI) of –0.06 to –1.33. In the alcohol abuse/dependence-negative subgroup, d+ was –0.34, with a 95% CI of –0.89 to 0.21. (These values correspond to a PTSD-positive minus PTSD-negative contrast.)
There were no main effects of alcohol abuse/dependence or cohort on hippocampal volume. Adjustment for cranial volume, total cerebral tissue volume, and WAIS vocabulary score all failed to reinstate an effect of PTSD on hippocampal volume in the alcohol abuse/dependence-negative subgroup. Rather, adjustment for cranial volume eliminated the effect of PTSD on hippocampal volume in the alcohol abuse/dependence-positive subgroup (F=1.97, df=1, 38, p=0.17) and in the group as a whole (F=1.34, df=1, 90, p=0.25). None of these results was modified by the exclusion of women or of PTSD-positive subjects with CAPS total severity scores below 65.
Hippocampal volume was not correlated with combat trauma exposure as indexed by Combat Exposure Scale scores (r=–0.12, df=99, p=0.23) in the whole group; however, because the Vietnam and Gulf War veterans had experienced different distributions of combat exposure, these relationships were reestimated for each cohort. In the Vietnam cohort only, there was a moderately significant inverse correlation between hippocampal volume and Combat Exposure Scale score (r=–0.28, df=61, p<0.03). In the whole group, after prior entry of age and vocabulary scores, both cerebral tissue volume (β=0.303, t=2.04, df=94, p<0.05) and cranial volume (β=0.356, t=2.29, df=94, p<0.03) accounted for unique variance in hippocampal volume.
Discussion
The subjects with PTSD and histories of comorbid alcoholism exhibited effects on hippocampal volume similar in direction and magnitude to those reported in studies in which PTSD-positive subjects had greater lifetime exposure to alcohol than comparison subjects. Nonalcoholic PTSD-positive subjects exhibited a nonsignificant tendency (3%) toward a smaller hippocampus. Adjustment for cranial volume, total cerebral tissue volume, or vocabulary failed to uncover an effect of PTSD on hippocampal volume in nonalcoholic veterans. A comparison of PTSD effect sizes in alcoholics and nonalcoholics confirmed the possible role of alcoholism as a facilitator of the effect of PTSD on the hippocampus but introduced important caveats. The observed confidence intervals surrounding these effects are large and overlapping. The CI in the alcoholic subgroup includes small effects, whereas the CI in the nonalcoholic subgroup includes large effects. The absence of a statistically significant effect in nonalcoholics could represent a type II error.
Acknowledging these caveats, the present results raise doubts regarding certain explanations that have been advanced to explain earlier failures to find smaller hippocampal volumes in nonalcoholic PTSD-positive groups. A 27-year differential in chronicity did not result in a PTSD × cohort interaction, and although power was limited by the small size of the Gulf War PTSD comparison, the observed tendencies were contrary to a chronicity effect. Exclusion of PTSD-positive subjects with CAPS total severity scores below 65 also did not influence the results. The alcoholic and nonalcoholic subgroups had similar Combat Exposure Scale scores, CAPS total severity scores, and Beck Depression Inventory scores. Statistical power for comparisons performed within the nonalcoholic subgroup was comparable to multiple studies reporting positive findings.
A role for comorbid alcohol abuse/dependence in prior observations of smaller hippocampal volume in PTSD is tentatively supported in these data. At the same time, lifetime alcoholism was not independently associated with smaller hippocampal volume even before adjustment for total cerebral tissue volume. Deployed U.S. military veterans who do and do not meet criteria for lifetime alcoholism may have less contrastive alcohol histories than groups sampled from civilian populations. Nevertheless, the observed reversal of the aging-alcohol interaction could arise only if the effects of alcoholism on the hippocampus were accentuated in the Gulf War cohort, attenuated in the Vietnam cohort, or both. It is possible that biased attrition-attenuated selected group effects involved Vietnam-era PTSD-positive alcoholic subjects in this study. Drescher et al.
(56) demonstrated that a contemporaneous Vietnam-era sample drawn from the VA Palo Alto Healthcare System PTSD inpatient population exhibited excess age-adjusted mortality in association with alcohol and substance abuse. The survivor population would be expected to exhibit attenuated versions of neurobiological concomitants of alcohol and substance abuse preferentially associated with premature mortality. The possibility that a smaller hippocampus participates with alcohol/substance abuse to confer a predisposition to premature mortality cannot be ruled out, particularly if a smaller hippocampus is predispositional to PTSD
(2), itself a consequence of exposure to life threat. This study found modest support for an inverse relationship between hippocampal volume and exposure to potentially traumatic combat events, as reported by Gurvits et al.
(3) .
The current observation of normal hippocampal volume in PTSD uncomplicated by alcoholism appears to contradict the findings of Gilbertson et al.
(2) . In a study of monozygotic twins, these authors obtained evidence that a smaller hippocampus represents an inherited predisposition to develop PTSD after trauma rather than being a consequence of trauma. These findings are not incompatible if the data of Gilbertson et al. are interpreted to indicate that a smaller hippocampus is predispositional to PTSD with comorbid alcohol abuse/dependence. Eighty-two percent of the PTSD-positive subjects of Gilbertson et al. met criteria for comorbid alcoholism. As well, the unexposed twins of their PTSD-positive alcohol abuse/dependence-positive subjects tended to exhibit higher rates of alcohol abuse/dependence (47% versus 30%) and higher scores on the Michigan Alcoholism Screening Test (6.8 versus 2.5; p=0.09; reference
44 ) than the unexposed twins of PTSD-negative subjects, both observations compatible with an elevated risk for primary alcoholism. Evidence of shared genetic vulnerability to combat exposure/PTSD and alcoholism
(57) has been obtained from other samples drawn from the Vietnam Era Twin Registry
(58) .
Among the covariates used to increase the power of group comparisons of hippocampal volume, an estimate of cranial volume had the opposite effect, eliminating PTSD effects even in the alcoholic subgroup. This result might have been achieved if adjustment for cranial volume had simply added a random variate to hippocampal volume; however, cranial volume accounted for a significant unique variance in hippocampal volume. This observation is remarkable in light of the fact that the cranium expands little after age 5 or 6
(49,
59) . Systematic effects on cranial volume noted in this group are considered in a separate article (unpublished study by Woodward et al.).