Illicit anabolic-androgenic steroid (AAS) use is a public health problem in many countries
(1,
2) . AAS use—especially if prolonged—may cause medical morbidity
(2,
3), including atherogenesis
(4), gynecomastia
(5), hepatotoxicity
(6), and suppressed neuroendocrine function
(7) . AAS may also cause adverse psychiatric effects
(2,
8), including aggression and violence during AAS use
(9), depression during AAS withdrawal
(10), AAS dependence
(3), and progression to opioid abuse
(11) . In the United States, probably at least 1 million boys and men have used AAS at some time
(2,
12), including 3%–11% of American male high school students
(2), many of whom used these drugs not for athletic purposes but simply to improve personal appearance
(1,
2,
13,
14) . AAS use is uncommon among girls and women; in the 1994 National Household Survey on Drug Abuse (the most recent to collect AAS data), men were 13 times more likely than women to report AAS use in the past 3 years
(12) . Accordingly, the discussion below is confined to male users.
Male AAS users often report body-image concerns
(1) . For example, Brower et al.
(15) evaluated 35 male weight lifters who answered “yes” when asked if they might use AAS in the future; 25 (71.4%) of these men reported that they felt “not big enough.” Elliot and Goldberg
(16) found that 279 of 1,000 high school football players showed “high intent” to use AAS, based on questionnaire responses, and this group reported significantly less satisfaction with their physiques than the low-intent group. Blouin and Goldfield
(17), using a modified version of the Eating Disorders Inventory
(18), found significantly higher scores on a “drive for bulk” scale among 19 AAS-using bodybuilders, compared to 24 nonusing bodybuilders. Schwerin et al.
(19) found slightly, although not significantly, higher scores on a body dissatisfaction scale among 35 AAS users, compared to three non-AAS-using groups. Our group
(20) compared 48 AAS users and 45 nonusers on their responses to the following Likert-type scale item: “At the time that you first started lifting weights, how confident were you about your body appearance?” For each 10% increase on this scale, the estimated incidence of AAS use
decreased by 23%.
It is interesting to note that AAS users sometimes report a syndrome called “reverse anorexia nervosa”
(21) or “muscle dysmorphia”
(22,
23), characterized by 1) preoccupations that they look small when they are actually muscular; 2) giving up social and occupational opportunities because of the need to work out; and 3) avoiding situations where their bodies might be seen in public. In a 1994 study, we found that 16 (18.2%) of 88 male AAS users reported a history of “reverse anorexia nervosa” (as it was then called), compared to none of the 66 comparison weight lifters
(24) . In our study described earlier in this section
(20), eight (16.7%) of 48 AAS users versus three (6.7%) of 45 nonusers met the criteria for muscle dysmorphia
(14) . In both studies, many AAS users first developed the full syndrome of muscle dysmorphia after their first AAS use, which suggests that using AAS and gaining muscle did not necessarily resolve these men’s insecurities about their size.
Similar impressions arise from a recent study comparing 50 aerobic exercisers, 39 non-AAS-using bodybuilders, 29 current AAS users, and 19 former AAS users
(25) . On the Eating Disorders Inventory (slightly modified for male respondents), both current and ex-AAS users scored significantly higher than the other two groups on total score and on virtually all of the individual subscales, with ex-AAS users typically producing even higher scores than current users. Current users also showed a strong correlation (r=0.58, p=0.001) between Eating Disorders Inventory scores and a scale measuring severity of drug dependence. On the basis of these findings, the authors suggested that reverse anorexia was associated with AAS use in general and AAS dependence in particular.
To add to these findings, we examined data from our study
(20) of 48 AAS users and 45 nonusers to 1) augment previous data suggesting that AAS use is associated with poor body image and 2) test the hypothesis that “heavy users” reporting prolonged, repeated AAS use would demonstrate greater body-image concerns than “experimenters” who had used AAS only briefly.
Method
We evaluated 93 men experienced with lifting weights, comprising 48 current or past AAS users and 45 nonusers, recruited during an earlier study through advertisements in gymnasiums and sports supplement stores in Massachusetts and Florida
(20) . All subjects provided written informed consent for the study after the procedures had been fully explained. All 48 AAS users and 41 (91%) of the nonusers identified themselves as heterosexual; four (9%) nonusers described themselves as homosexual or bisexual. Because we were assessing body-image measures and because homosexual or bisexual orientation may itself be associated with body-image disorders
(26 –
29), we excluded these latter four subjects from the analysis to avoid possible confounding effects due to sexual orientation. Thus, the final study group comprised 48 AAS users and 41 nonusers. These groups were similar in age (mean for users=29.3 years, SD=6.5; mean for nonusers=30.1 years, SD=10.5) (t=0.44, df=87, p=0.66, two-tailed), ethnic distribution (N=9 [19%] versus N=8 [20%] nonwhite) (p=1.00, Fisher’s exact test, two-tailed), marital status (14 [29%] versus 14 [34%] ever married; p=0.65, Fisher’s exact test, two-tailed, and education (17 [35%] versus 21 [51%] college graduates; p=0.20, Fisher’s exact test, two-tailed). All subjects were administered a verbal interview and a package of questionnaires covering demographic information, athletic history, psychiatric history, history of licit and illicit drug use, and various psychological ratings.
Many of the study instruments were used to assess subjects’ attributes in childhood and early adolescence, before AAS use. These results have been presented previously
(20) . The current article presents findings from four instruments used to inquire about subjects’
current (adult) attitudes and behaviors. The first instrument was the Rosenberg Self-Esteem Scale
(30), a 10-item measure of general self-esteem generating scores from 10 (lowest self-esteem) to 40 (highest). Second, we administered the Eating Disorders Inventory
(18), a 64-item scale used in previous studies of AAS users described earlier. Normally used to assess features of eating disorders in women, the Eating Disorders Inventory generates eight subscale scores: bulimia, interoceptive awareness, maturity fears, perfectionism, interpersonal distrust, ineffectiveness, drive for thinness, and body dissatisfaction. We used only the first six of these scales, however, because the last two were based on questions unsuited for male athletes (e.g., “I think my thighs are too big,” or “If I gain a pound, I worry that I will keep gaining”). Therefore, the total Eating Disorders Inventory score, as reported in the Results section, represents the sum of only six scales rather than the usual eight. The third instrument was the Male Role Attitudes Scale
(31), an eight-item measure of masculine ideology, with scores ranging from 8 to 32. Men scoring high on the Male Role Attitudes Scale were those who most strongly endorsed conventional attitudes about male roles (e.g., “A guy will lose respect if he talks about his problems,” “It bothers me when a guy acts like a girl,” and “Men are always ready for sex”). Fourth, we used three yes-no items from an unpublished “muscle dysmorphia questionnaire”; this questionnaire was of our own design and not formally validated. The first question was “Are you sometimes preoccupied that you are too small and that you need to get bigger?” If the answer to question 1 was yes, the respondent was then asked to answer the following questions: 2) “Have you ever worn heavy sweatshirts in the summer or refused to take your shirt off in public for fear that someone may think that you are too small?” and 3) “Do you find yourself giving up enjoyable activities because of this preoccupation?”
We first compared AAS users and nonusers on these measures using linear or logistic regression, for continuous and binary outcome variables, respectively, while adjusting for subjects’ age and for the geographic location where the subject was interviewed (Florida versus Massachusetts). We found no significant interactions between AAS user status and either of these covariates. There were no significant differences between the Massachusetts and Florida groups in subjects’ mean age, education, or income (p>0.05, t test) and no significant differences in the proportion of subjects who were nonwhite or who were married (p>0.05, Fisher’s exact test).
Next, to test the hypothesis that body-image concerns were primarily related to heavy AAS use, we grouped the AAS users by median split, resulting in 1) a group of 24 “experimenters” who reported lifetime use of AAS for 2–5 months (median=3.4) and 2) a group of 24 “heavy users” who reported AAS use for 6–150 months (median=15.5). It should be noted that these figures represent total months rather than consecutive months of use, because AAS are typically taken in repeated courses (“cycles”) of varying duration
(2,
3) . We compared the experimenters and heavy users with the nonusers, using the same statistical methods. Finally, because some previous studies have contrasted current AAS users with past users
(19,
25), we compared the 31 current AAS users (defined as those reporting AAS use within the past year) and the 17 past AAS users with the nonusers, again using the same statistical methods.
Because many of the measures were correlated, it was difficult to calculate an appropriate correction for multiple comparisons. Thus, the results are presented without correction, with alpha set at 0.05, two-tailed; the reader should therefore recognize that some findings may represent chance associations. We address this issue further in the Discussion section.
Results
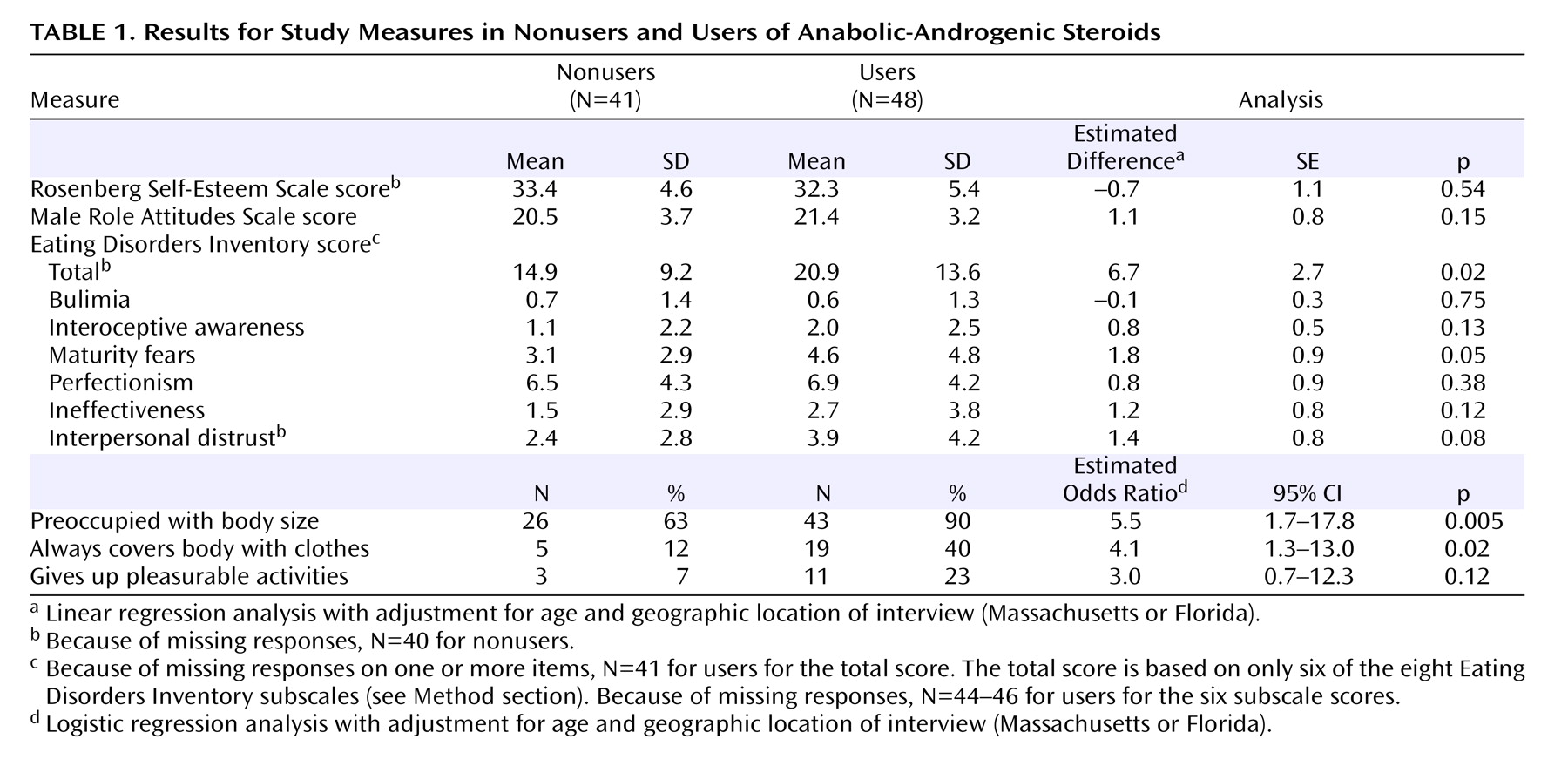
Overall, AAS users showed no significant differences from nonusers on the Rosenberg Self-Esteem Scale, the Male Role Attitudes Scale, and most of the Eating Disorders Inventory subscales (
Table 1 ), although users did show a modestly elevated total score on the combined six subscales of the Eating Disorders Inventory used in this study. On our body-image measures, however, differences were more marked: AAS users were particularly more likely to report preoccupations that they were too small and needed to get bigger.
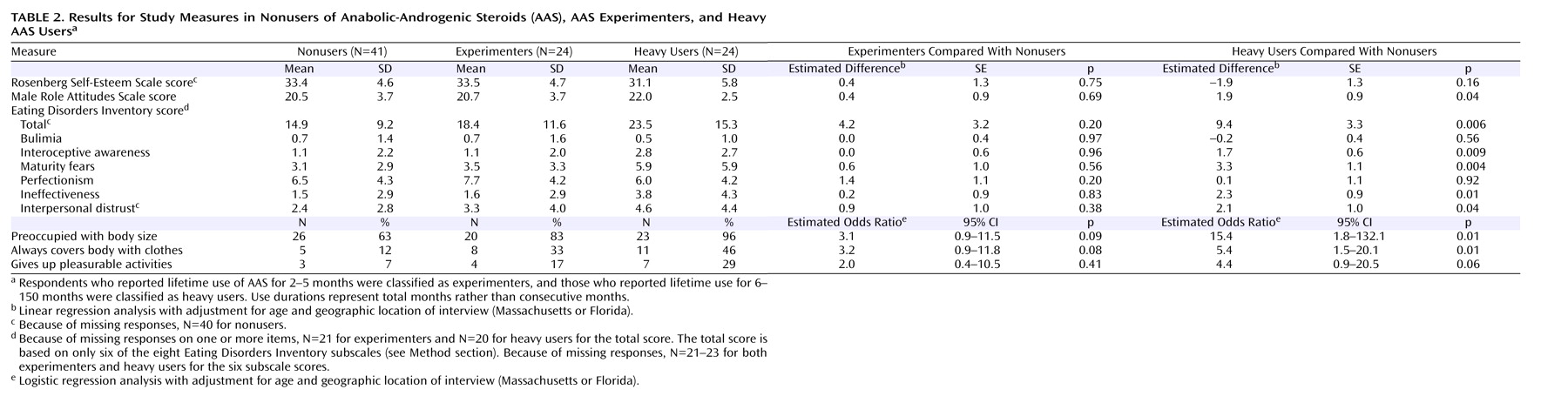
When we divided the AAS users into short-term “experimenter” and long-term “heavy user” groups, however, a more striking pattern emerged (
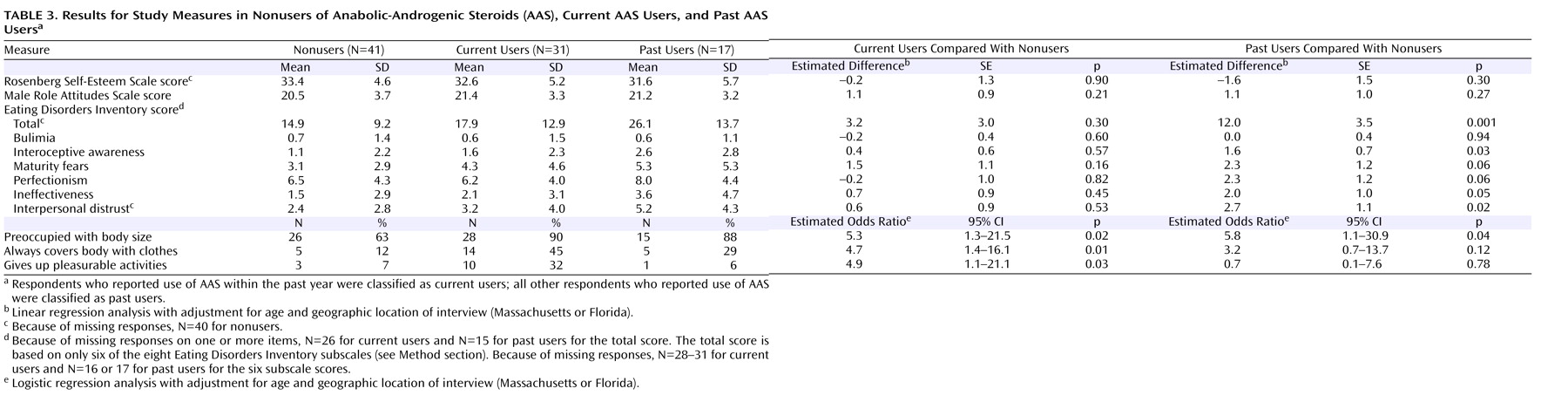
Table 2 ): the experimenters showed no significant differences from the nonusers on any of the measures, whereas the heavy AAS users exhibited marked differences almost across the board, with the exception of the Rosenberg Self-Esteem Scale score. It is interesting to note that the heavy users differed from the nonusers not only on the body-image measures but also in Male Role Attitudes Scale score–suggesting that heavy users were more likely to endorse stereotypic male roles. By contrast, the division between current and past AAS users produced fewer differences (
Table 3 ): both current and past users differed somewhat from nonusers, with past users scoring higher on attitude measures as reflected on the Eating Disorders Inventory and current users tending to score higher on behavioral measures as reflected on the muscle dysmorphia questionnaire.
Discussion
In a study of 48 male AAS users and 41 nonusers, we explored the association between AAS use and various measures of self-esteem, male role attitudes, and body image. Because the 41 nonusers were themselves experienced with lifting weights and were recruited by using the same methods used to recruit the AAS users
(20), our findings likely reflect attributes associated with AAS use in particular rather than weight lifting in general.
Overall, in agreement with previous studies
(15 –
17,
20,
23 –25), we found that AAS use was associated with body-image pathology, as suggested by elevated scores on the Eating Disorders Inventory, as well as by responses suggesting muscle dysmorphia (reverse anorexia nervosa) on our muscle dysmorphia questionnaire. Also in general agreement with previous research
(25), we found evidence of pathology in both current and past AAS users, with behavioral measures tending to distinguish the current users and attitude measures tending to distinguish the past users. These findings suggest that body-image concerns, in one form or another, may be a stable trait in AAS users rather than a state associated exclusively with initial or recent use of AAS. Notably, we were unable to demonstrate differences among study groups on the Rosenberg Self-Esteem Scale, suggesting that AAS use may not be strongly associated with low self-esteem in general but rather with poor body image in particular. However, this observation differs from the findings of a previous comparable study that included the Rosenberg scale; in that study, modestly but significantly lower scores were found for 19 AAS versus 24 comparison bodybuilders
(17) .
In addition, the study produced two novel findings that may extend our understanding of the associations between AAS use and body-image concerns. First, we found that short-term AAS “experimenters” exhibited little evidence of body-image pathology, compared to non-AAS-users, whereas “heavy users,” who reported a median of 15.5 months of AAS use, displayed prominent pathology. This finding appears congruent with the impressions of both Brower
(3) and Cole et al.
(25) that body-image pathology is associated with AAS dependence—although we caution the reader that we did not formally assess AAS dependence but rather assessed duration of use. In any case, this observation has direct clinical implications, because brief AAS experimentation likely poses much less danger to individual and public health than does long-term AAS use or dependence
(2 –
4,
7,
8) . If body-image disorders—which are potentially treatable with pharmacological
(22,
32) and cognitive behavior therapies
(33) —help to cause or perpetuate heavy AAS use or dependence, it would seem important to focus treatment and prevention resources primarily on this group. Second, our analysis tentatively suggested that in addition to body-image pathology, strong endorsement of conventional male roles may be also associated with heavy AAS use.
Several limitations of our study should be considered. First, our sampling method limited our conclusions, in that we lacked a group of athletes who did not lift weights or a group of nonathletes available for comparison. It would also follow that our conclusions apply only to AAS users who lift weights. However, virtually all AAS users
are in fact experienced with lifting weights
(34,
35) ; thus, our sampling method would seem unlikely to have produced a limited or atypical sample of AAS users. Second, our study is limited by the modest number of subjects and the possibilities of selection or differential response bias, as discussed in our previous report
(20) . Third, as noted earlier, it is difficult to calculate an appropriate correction for multiple comparisons in the present study, because many of the measures were very closely correlated with one another. For example, individuals responding positively to one of the muscle dysmorphia questionnaire items were likely to respond positively to the others and also likely to display higher scores on scales of the Eating Disorders Inventory associated with body image. Therefore, a simple Bonferroni correction, dividing the alpha level by the total number of comparisons, would tend to produce overcorrection, possibly causing many type II errors (failure to reject the null hypothesis when in fact a genuine difference exists). Given these considerations, and given that this was partially a hypothesis-generating study, we presented the findings without correction for multiple comparisons; readers should therefore recognize that some findings of modest significance (e.g., p values between 0.01 and 0.05) may represent chance associations. Fourth, our most striking findings—in the comparison of long-term AAS users and short-term “experimenters”—were based on an a posteriori median split of AAS users by duration of use. These findings need to be replicated in a study using an a priori definition of heavy AAS use. Finally, our cross-sectional design did not permit causal inferences. To establish that body-image pathology and endorsement of conventional male roles play a causal role in heavy AAS use, one would require a longitudinal design in which the temporal sequence of these and other candidate risk factors and the outcomes of AAS use and dependence could be evaluated.
Despite these reservations, a causal hypothesis would nevertheless seem intuitively plausible: if an individual combines a narrow and stereotypic view of masculinity (men must be tough, command respect, etc.) with insecurity about his body image (the belief that he does not look big and strong enough), this mixture would seem very likely to contribute to long-term AAS use or dependence. If this causal model is supported by longitudinal studies, it would follow that cognitive behavior approaches might deter or treat AAS dependence by simultaneously taking aim at both of these categories of maladaptive beliefs.