Cognitive behavior therapy (CBT) is a common empirically supported intervention
(1) that is effective in 40%–60% of patients with unipolar depression
(2) . Knowing which patients are likely to benefit from CBT could increase the response rate and, through targeted referrals, decrease costs. CBT involves, among other skills, learning to interrupt automatic sustained emotional processing (e.g., elaboration, rumination) with controlled processing. As a preliminary step toward prediction, this study examined the association of the neural substrates of sustained emotional processes pretreatment with posttreatment recovery. Sustained emotional reactivity was examined because it is specifically addressed in CBT and because depressed individuals display increased and sustained reactivity in brain regions that subserve emotional processing, particularly the amygdala
(3 –
5) . Unmedicated patients with unipolar depression underwent functional magnetic resonance imaging during an emotional information processing task before initiating CBT. Analyses identified brain regions in which sustained reactivity to emotional information was associated with symptom change. Activity in these regions was then compared with that of healthy subjects.
Method
Study participants were 14 individuals (seven men and seven women; 79% Caucasian [N=11]) with unipolar major depressive disorder (mean age=45.2 years [SD=9.3, range=23–55]; mean Beck Depression Inventory score=24 [SD=11.7]) and a comparison group of 21 healthy subjects (nine men and 12 women; 57% Caucasian [N=12]) with no current or lifetime axis I disorder (mean age=31.3 [SD=8.6]; mean Beck Depression Inventory score=3.7). Participants passed a cognitive screen, had a verbal IQ score equivalent >90, and described no history of psychosis, manic or hypomanic episodes, or antidepressant use within 2 weeks of testing (6 weeks for those receiving fluoxetine). Participants also reported no health problems, eye problems, or psychoactive drug or alcohol abuse in the preceding 6 months.
After signing consent forms approved by an institutional review board, participants underwent an examination that included a diagnostic interview
(6), vision test, and psychophysiological measures. Upon completion of this examination, participants underwent fMRI in which a 3-T scanner (GE Medical Systems, Milwaukee) acquired T
2 *-weighted images depicting BOLD contrast using a reverse spiral pulse sequence (TR=1500 msec, TE=5 msec, field of view=24 cm, flip angle=60°). Thirty or 34 3.2-mm slices parallel to the anterior commissure-posterior commissure line were obtained, at a rate of 8 volumes per 12-second trial. In the scanner, participants rated as quickly and accurately as possible the personal relevance of 60 emotional words by pushing buttons on a response box according to whether each word was relevant, somewhat relevant, or not relevant to them. As previously described
(3), the emotional valences of the 60 words were positive (N=20), negative (N=20), or neutral (N=20); half of the words were normed, and half were idiosyncratically generated. Normed words were balanced for affective intensity, arousal, word length, and word frequency. Trials entailed a 1-second fixation cue followed by a word (200 msec), followed by a mask of 13 x’s (10.8 seconds). Stimuli were displayed in black on a white background via a back-projection screen (0.88
o visual angle). Mappings of buttons to responses were counterbalanced across participants.
Depressed participants then received 16 sessions of CBT over 12 weeks following the guidelines of Beck
(1) . At each session, participants completed the Beck Depression Inventory II to assess depressive severity.
To examine change in severity not confounded by initial severity, residual change in depressive severity was computed from a regression of initial Beck Depression Inventory scores on final Beck Depression Inventory scores.
fMRI data were preprocessed via motion and outlier-correction, linear trend removal, temporal smoothing (5-point filter), linear cross-registration to a reference brain, and 6-mm full width at half maximum spatial smoothing. Whole-brain voxelwise regressions of residual severity on mean fMRI signal 6–10.5 seconds after presentation of negative words minus a prestimulus baseline were used to detect regions in which activity was associated with recovery. Type I error was controlled by selecting only large clusters of significant voxels. To test a priori hypotheses, significant clusters in the amygdala (boundaries as described in our previous study
[3] ; small-volume correction) were examined. Group differences were tested in identified regions via a priori contrasts on sustained activity and exploratory group-by-valence-by-scan mixed effects analyses using an AR1 covariance structure to account for temporal autocorrelation. Type I error was controlled for simple-effects tests via Bonferroni correction.
Results
For those who completed CBT, response as determined by change in Beck Depression Inventory scores was variable but generally successful (pretreatment: mean=24.5, SD=12.0; posttreatment: mean=9.4, SD=8.1; change: mean=15.1, SD=11.8 [t=4.8, df=13, p<0.0005]). Initial severity accounted for 13.7% of variation in final severity.
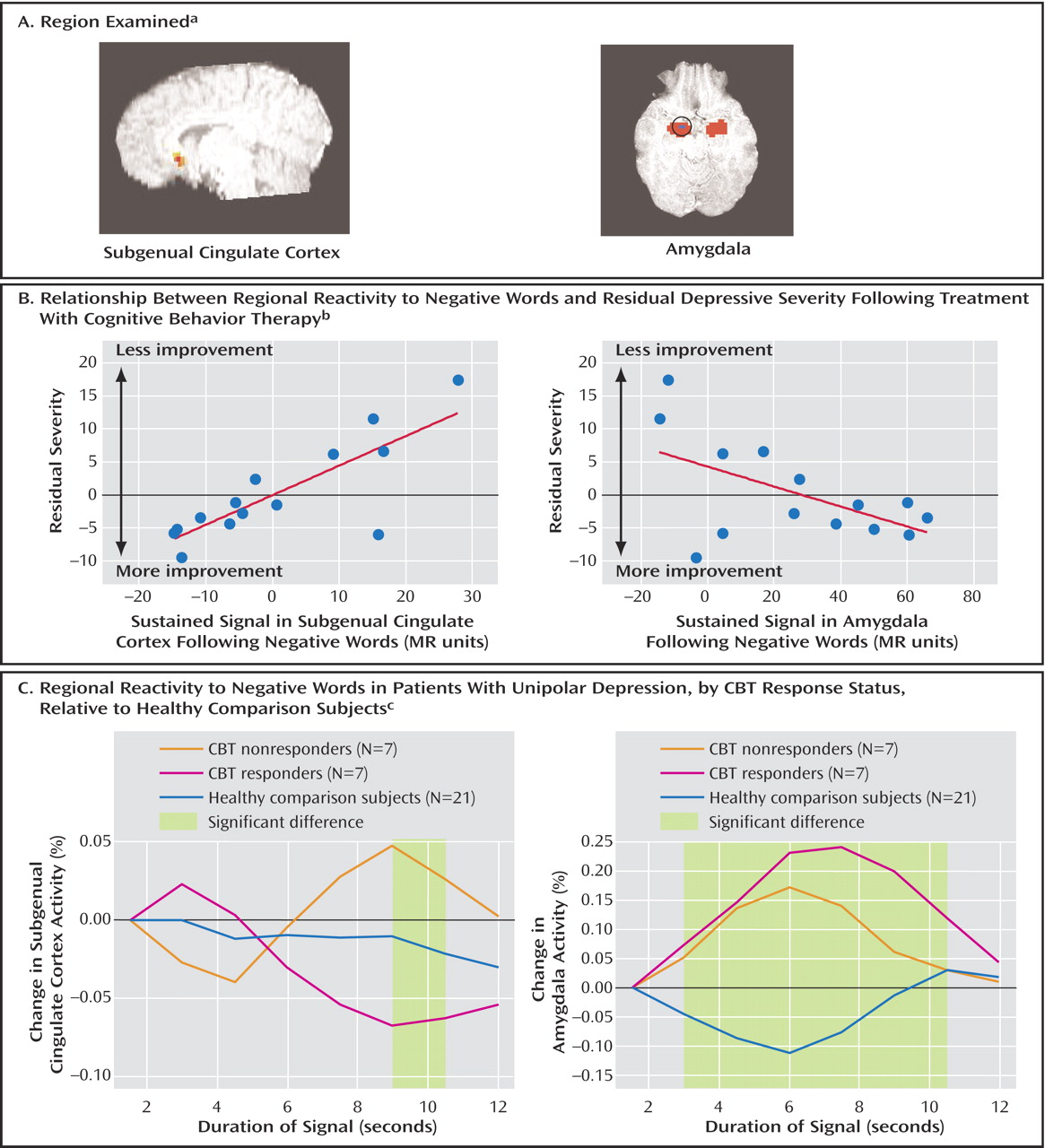
Whole-brain analyses revealed only that low sustained reactivity to negative words in the subgenual cingulate cortex (Brodmann’s area 25) was strongly associated with reduced depression severity following CBT (
Figure 1 ). Subgenual cingulate cortex activity accounted for 56.7% of variation above and beyond initial severity (total R
2 =0.65; F=22.4, df=1, 12, p<0.0005) and was unrelated to initial severity (R
2 =0.001, p=0.79). Logistic regression further revealed that subgenual cingulate cortex activity predicted recovery defined as final Beck Depression Inventory score <8: recovery was correctly predicted in seven of nine patients, and lack of recovery was correctly predicted in four of five patients (χ
2 =5.3, df=1, p=0.02). When the one outlier was removed, pretreatment subgenual cingulate cortex activity accounted for nearly all variation in CBT response (R
2 =0.91; F=124.9, df=1, 11, p<0.0005).
An a priori analysis of amygdala voxels exclusively revealed a region of the right amygdala (circled in
Figure 1 ) for which high sustained reactivity to negative words was associated with improved treatment response above and beyond initial severity (R
2 =0.30; F=5.24, df=1, 12, p=0.04) and unrelated to initial severity (R
2 <0.001, p=0.98). Amygdala activity marginally predicted recovery status (χ
2 =2.8, df=1, p=0.10).
A median-split divided participants with low and high residual Beck Depression Inventory scores following CBT. Low scorers were effectively asymptomatic (scores <7) after treatment.
A priori contrasts revealed that during the period 9–10.5 seconds after exposure to negative words, those who eventually responded to CBT had low subgenual cingulate cortex activity relative to nonresponders; the difference was marginally significant (t=2.03, df=12, p=0.06; d=1.10). Exploratory group-by-scan-by-valence mixed-model analysis suggested that group differences were apparent for all valences (group-by-scan: F=1.78, df=14, 423.3, p=0.04) and were not qualified by valence.
A priori contrasts revealed that during the period 3–10.5 seconds after exposure to negative words depressed individuals had significantly higher amygdala activity than did healthy subjects (t=3.42, df=33, p<0.005; D=0.18, d=1.18). Exploratory analysis confirmed group differences (group-by-scan: F=2.0, df=14, 456.3, p<0.02). Exaggerated responses were present for negative words (t=3.3, df=25, p=0.003) but not positive or neutral words in responders; follow-up tests were not significant for nonresponders (group-by-valence: F=6.65, df=4, 704, p<0.0005).
No tested effects were diminished with age as a covariate.
Discussion
Stronger recovery with CBT was associated with decreased pretreatment reactivity to negative words in the subgenual cingulate cortex (Brodmann’s area 25) and increased pretreatment reactivity in the amygdala. Both the amygdala and subgenual cingulate cortex display abnormal activity in depression
(3 –
5), and their activity normalizes upon treatment, particularly with antidepressants
(5,
7,
8) . The subgenual cingulate cortex has been implicated in regulating limbic activity
(9) . Sustained amygdala activity occurred in all depressed individuals, consistent with increased emotional reactivity. Decreased pretreatment reactivity in the subgenual cingulate cortex was specific to CBT responders, which suggests deficient regulation. These data could suggest that CBT is most useful to those who demonstrate increased emotional reactivity and who cannot engage regulatory structures. CBT may potentially help these individuals regain emotional control. Those who have neither sustained amygdala reactivity nor disrupted emotion regulation (especially subgenual cingulate cortex function) may not benefit as much from CBT.
Sustained amygdala and subgenual cingulate cortex reactivity to emotional stimuli were hypothesized to reflect an elaborative or ruminative coping style. Indeed, although patients’ percent change in sustained amygdala activity was not related to initial severity, it was correlated with a self-report rumination scale
(10) that assesses a tendency to think repetitively about one’s symptoms of depression (for depressed subjects: r=0.58, p=0.03; for the depressed and comparison subjects together [N=32]: r=0.51, p=0.003). This relationship was also present in our previous study
(3) . Rumination was also related to percent change in sustained subgenual cingulate cortex activity in the depressed participants (r=0.54, p=0.04) but not to residual symptoms (r=–0.24, p=0.40). Thus, sustained amygdala and subgenual cingulate cortex reactivity potentially reflect clinically relevant substrates of rumination.
The small study group size and use of a strongly hypothesis-guided task and analysis path could limit the generalizability of these results and may underestimate the potential predictive strength of imaging emotional information processing. Upon larger replications, imaging of emotional information processing could aid in recommending CBT to individuals for whom it appears most appropriate or for recommending other interventions to individuals for whom benefit is less strongly predicted.