Multiple lines of evidence, including studies of discordance among monozygotic twins, suggest that both genetic and environmental factors contribute to the development and clinical expression of Tourette’s syndrome
(1 –
5) . In addition to motor system abnormalities, Tourette’s syndrome is highly comorbid with several psychiatric syndromes, most commonly obsessive-compulsive disorder (OCD), attention deficit hyperactivity disorder (ADHD), and self-injurious behavior, which increase impairment and may be etiologically related to Tourette’s syndrome
(6 –
8) . Investigation into the genetic underpinnings of Tourette’s syndrome is ongoing, and genetic studies are plentiful
(1) . The potential role of environmental factors has been less studied, and the findings across studies have been inconsistent
(2,
4,
5,
9 –13) . These studies have generally indicated that children with tics or Tourette’s syndrome have higher rates of maternal/obstetric complications than do comparison subjects
(4,
9 –14) . Increased risk of Tourette’s syndrome has been associated with low birth weight
(4), increased rates of maternal complications
(11), increased parental age
(10), and lower Apgar scores
(10) . Increased tic severity among those with Tourette’s syndrome has been associated with low birth weight
(2,
4,
5), increased maternal stress and nausea
(9), and birth complications
(9,
11) . Similarly, forceps delivery and maternal use of coffee, alcohol, and tobacco have been associated with increased risk of OCD among Tourette’s syndrome patients
(12) .
In this study, we examined the relationship between prenatal and perinatal adverse events and clinical expression in 180 Tourette’s syndrome subjects. We aimed to identify specific environmental risk factors for increased tic severity and presence of comorbid OCD, ADHD, and self-injurious behavior. We hypothesized that perinatal hypoxia and factors associated with a risk of decreased fetal oxygenation (e.g., perinatal distress, emergency/urgent cesarean section) would be associated with increased severity. We also hypothesized that male Tourette’s syndrome subjects would have higher rates of adverse events and that there would be an interaction between adverse perinatal factors and a family history of tics or OCD, leading to increased symptom severity.
Method
Subjects
The study group consisted of 180 individuals with Tourette’s syndrome (ages 3 to 59) recruited for three genetic studies between 1996 and 2001: a genetic study in Costa Rica (N=53), a genetic study among individuals of Ashkenazi Jewish descent in the United States (N=99), and an affected sibling pair study (N=28) in the United States. Costa Rican subjects were ethnically Hispanic; the affected sibling pair and Ashkenazi subjects were Caucasian. Seventy-two percent of subjects were under 18 at the time of interview. Subjects in the United States were recruited primarily from Tourette’s syndrome specialty clinics and the Tourette Syndrome Association. Subjects in Costa Rica were recruited through health care professionals, media advertisements, elementary schools, and friends or family members. Informed consent (and assent, for children older than 5) was obtained for all subjects, and the studies were approved by the relevant institutional review boards.
Diagnostic Assessments
Diagnostic information was systematically gathered from structured instruments administered by two psychiatrists (C.A.M. and L.D.H.). Lifetime symptom prevalence and worst ever symptom severity were assessed in all cases. Interviews were videotaped for confirmation of tics. Information about motor and vocal tics, obsessive-compulsive symptoms, ADHD, and self-injurious behavior was elicited by using the Yale Self-Report Form
(15) . The Yale Global Tic Severity Scale was used to assess worst ever lifetime tic severity
(16) . Tic severity as measured by the Yale Global Tic Severity Scale is correlated with clinical impairment, including impaired learning and problems with self-esteem
(17,
18) . Because of the possibility that the total Yale Global Tic Severity Scale score, which includes a measure of global impairment, could be confounded by the impact of comorbid disorders such as OCD, we examined both the global score and total tic severity without the global measure of impairment. Except where noted, Yale Global Tic Severity Scale total scores are tic severity scores only, since the results for both were similar.
Environmental factors and family history of tics and obsessive-compulsive symptoms were assessed with a semistructured clinical interview. Medical records were obtained when available (N=58). In the vast majority of cases, parents were present during the interview, allowing confirmation of childhood symptoms and providing detailed information on prenatal and perinatal complications. Diagnoses of Tourette’s syndrome, OCD, and ADHD were made according to DSM-IV criteria by experienced clinicians (C.A.M., V.I.R., T.L.L.). The interrater agreement was 95% for Tourette’s syndrome (kappa=0.62), 94% for OCD (kappa=0.88), and 91% for ADHD (kappa=0.82).
Outcome and Predictor Variables
The outcome measures included lifetime overall worst tic severity and presence of comorbid OCD, ADHD, or clinically significant self-injurious behavior. Because of the low rates of DSM-IV OCD in the Costa Rican sample
(19), subclinical OCD and obsessive-compulsive symptoms were also examined. Environmental factors were divided into three categories: prenatal problems, perinatal problems, and in utero medication exposure. Information was obtained on history of traumatic delivery; fetal respiratory distress; nuchal cord; forceps or suction delivery; hypoxia at birth; jaundice; in utero exposure to medication, tobacco, regular alcohol (≥5 glasses of wine or equivalent during the pregnancy) or any illicit drug; gestational diabetes; preeclampsia; emergency or unplanned cesarean section; delivery greater than 2 weeks postterm; premature delivery (greater than 2 weeks preterm); hyperemesis; threatened abortion; multiple births; use of fertility drugs; and birth weight. Other problems (e.g., bleeding or maternal physical abuse during pregnancy, dystocia, seizures) were also noted. Maternal and paternal ages were also examined.
Statistics
Statistical analyses were generated by using Stata 6.0. Predictor variables (prenatal problems, perinatal problems, in utero medication exposure, birth weight, paternal age, and maternal age) were entered into a linear or logistic regression as appropriate. Categorical variables describing the interaction between sex or family history and the predictor variables were created and also were entered into the models. Potentially confounding variables such as sex, group (Costa Rican, Ashkenazi, or affected sibling pair), age at interview, referral source, and family history were also included. Variables with p values ≥0.15 were sequentially removed by using a backward stepwise regression until the model parameters were maximized.
Results
Group Characteristics
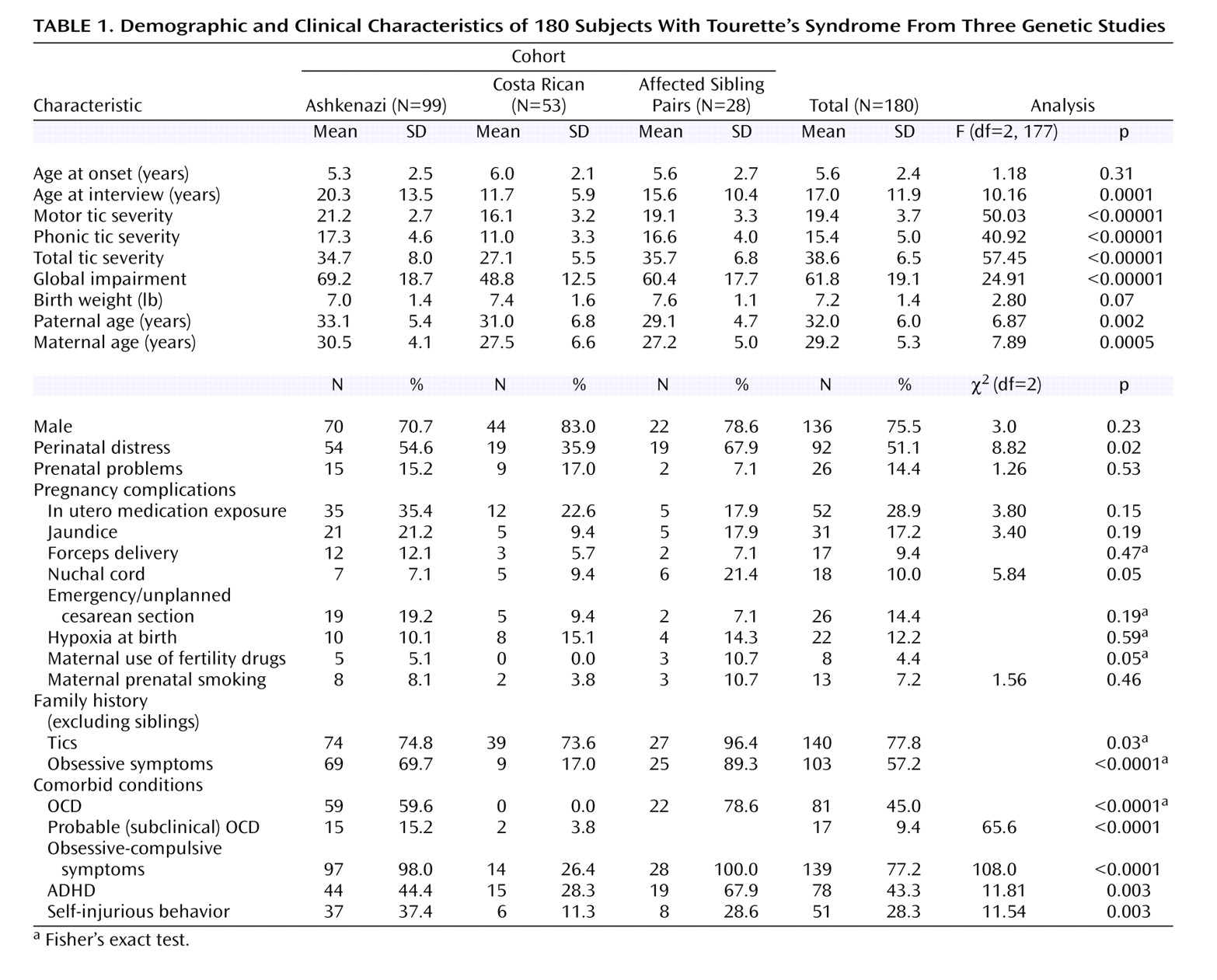
The three groups were significantly different in terms of clinical severity and in prevalence of prenatal and perinatal problems (
Table 1 ). Overall, the Costa Rican subjects were less severely affected than the subjects in the Ashkenazi or the affected sibling pair cohorts, with lower rates of OCD, ADHD, and self-injurious behavior, and lower tic severity scores. The Costa Rican subjects also reported fewer perinatal events than did the Ashkenazi or affected sibling pair subjects, while the Ashkenazi subjects had more in utero medication exposure. These disparities are most likely due to ascertainment differences: 51% of Costa Rican subjects were recruited through media advertisements, family members, or school referrals, whereas 97% of the Ashkenazi subjects and 100% of the affected sibling pair subjects were recruited through health care professionals and the Tourette Syndrome Association (χ
2 =138.9, df=2, p<0.0001). Because of the differences in symptom severity and exposure rates, subject group and referral source were included as confounding variables in all regression models. There were no significant gender differences in motor, phonic, or total tic severity scores or in rates of OCD, ADHD, or self-injurious behavior.
Symptom Severity
Subjects in our study generally had moderate to severe symptoms. The mean tic severity score was 38.6 of a possible 50 (range=14–50), and the mean global severity score was 61 of a possible 100 (range=27–100) (
Table 1 ). Motor tic severity scores were higher than phonic tic severity scores. With the exception of OCD in the Costa Rican subjects, the rates of OCD and ADHD in our study subjects were also comparable to rates seen in other studies (
Table 1 )
(4,
5,
9,
12) .
The presence of OCD was highly correlated with increased motor tic (F=23.97, df=1, 177, p<0.00001), phonic tic (F=24.81, df=1, 176, p<0.00001), and total tic (F=29.46, df=1, 176, p<0.00001) severity. Comorbid self-injurious behavior was also associated with increased tic severity (motor: F=42.19, df=1, 177, p<0.00001; phonic: F=14.86, df=1, 176, p=0.0002; total: F=29.18, df=1, 176, p<0.00001), as was comorbid ADHD, although weakly (phonic: F=3.93, df=1, 176, p=0.049; motor: F=3.87, df=1, 177, p=0.051; total: F=4.53, df=1, 176, p=0.035).
Prevalence of Prenatal/Perinatal Adverse Events
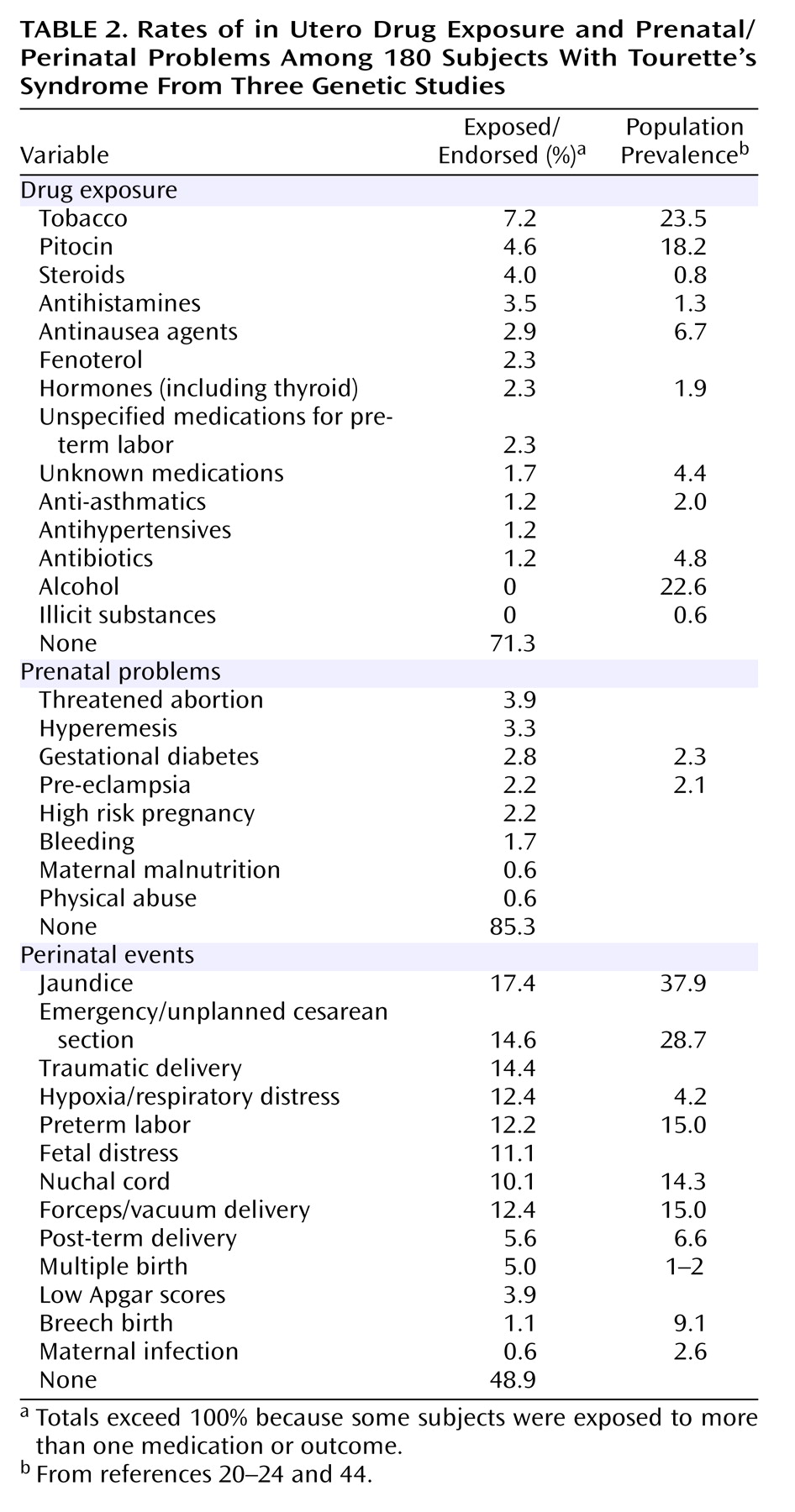
Over 50% of subjects reported at least one adverse perinatal event. The rates of medication exposure, prenatal problems, and perinatal complications in our study groups were generally similar to or lower than rates reported in the general population (
Table 1 and
Table 2 )
(20 –
24) . Subjects from the Costa Rican sample reported the fewest events (36%), while subjects in the affected sibling pair sample reported the most (70%) (
Table 1 ). Jaundice was the most frequent perinatal event, followed by emergency/urgent cesarean section and traumatic delivery (unspecified type) (
Table 2 ). Five percent of subjects were the product of multiple births (e.g., twins or triplets) (
Table 2 ). Female subjects were involved in significantly more unplanned or emergency cesarean sections (25.6%) than were male subjects (11.1%) (χ
2 =5.47, df=1, p<0.02). There were no significant gender differences in the rates of other perinatal events.
Rates of in utero medication exposure ranged from 18% in the sibling pair group to 35% in the Ashkenazi group (
Table 1 ). Tobacco was the most common substance, followed by pitocin and steroids (
Table 2 ). Eight percent of the Costa Rican sample had in utero exposure to fenoterol, a beta adrenergic agonist used in Europe and Latin America for preterm labor
(25) . There were no significant gender differences in rates of in utero exposure to medications, nor were there significant differences in rates of prenatal problems between study groups or by gender. Approximately 15% of subjects were exposed to prenatal problems, with threatened abortion being the most common, followed by hyperemesis during pregnancy (
Table 2 ).
Tic Severity
Medication exposure in utero was the only environmental factor that was significantly associated with increased global tic severity (average increase of 6 points on the Yale Global Tic Severity Scale global score) (F=8.31, df=9, p<0.00001). Other contributing factors were family history of obsessive-compulsive symptoms (6-point increase), male gender (5-point increase), and age at interview (one half-point increase in global score per year increase in age). Contrary to expectation, we found no interactions between gender or family history plus an adverse perinatal event (including in utero medication exposure) and tic severity. Birth weight, perinatal distress, prenatal problems, and parental age did not contribute significantly to the model, nor did number of medications to which the subject was exposed. In utero medication exposure was not significantly associated with total tic severity score.
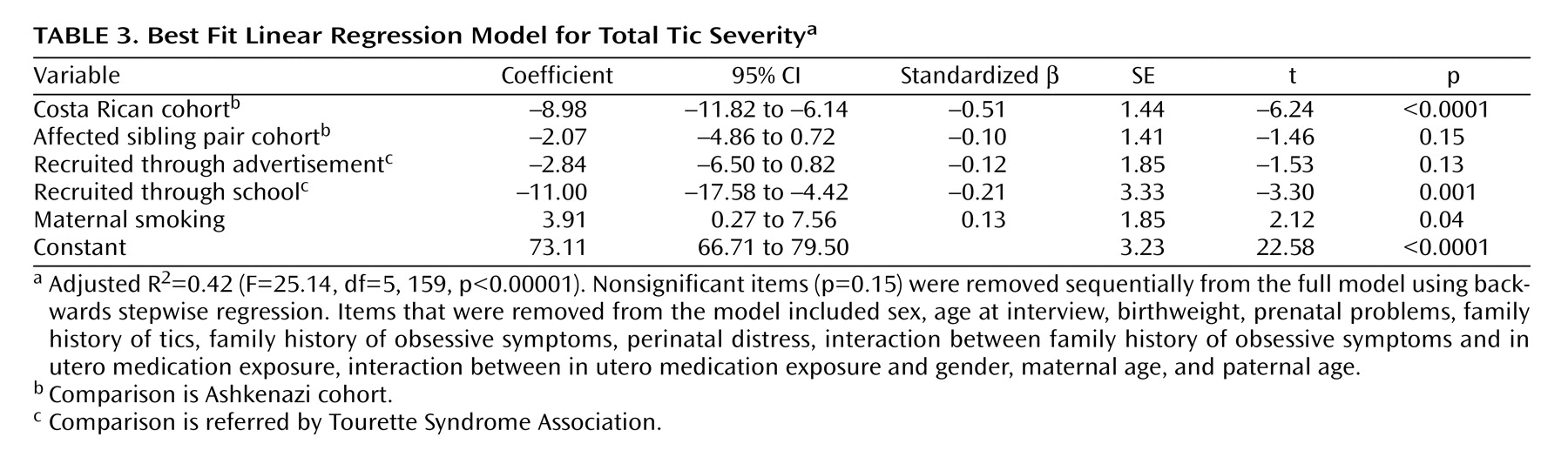
Because exposure to tobacco/nicotine was the most common in utero exposure, we examined separately the relationship between maternal smoking and symptom severity. When subject group, gender, and family history were controlled, maternal smoking was significantly associated with an increase in Yale Global Tic Severity Scale global score (F=9.27, df=6, 172, p<0.00001), in total tic severity (F=9.27, df=6, 172, p<0.00001), and in phonic tic severity (F=25.84, df=6, 172, p<0.00001), although not motor tic severity. Maternal smoking was associated with a 4-point increase in total tic severity and with a 3-point increase in phonic tic severity. There was no evidence of an interaction between maternal smoking and gender or family history in relation to tic severity. For Yale Global Tic Severity Scale global score, the model that included maternal smoking accounted for 26% of the variance among subjects, compared with 29% of the variance for the more general model for in utero medication exposure, suggesting that nicotine exposure was the primary contributor to tic severity. The model including maternal smoking accounted for 42% of the variance in total tic severity (
Table 3 ).
Comorbid Disorders
OCD
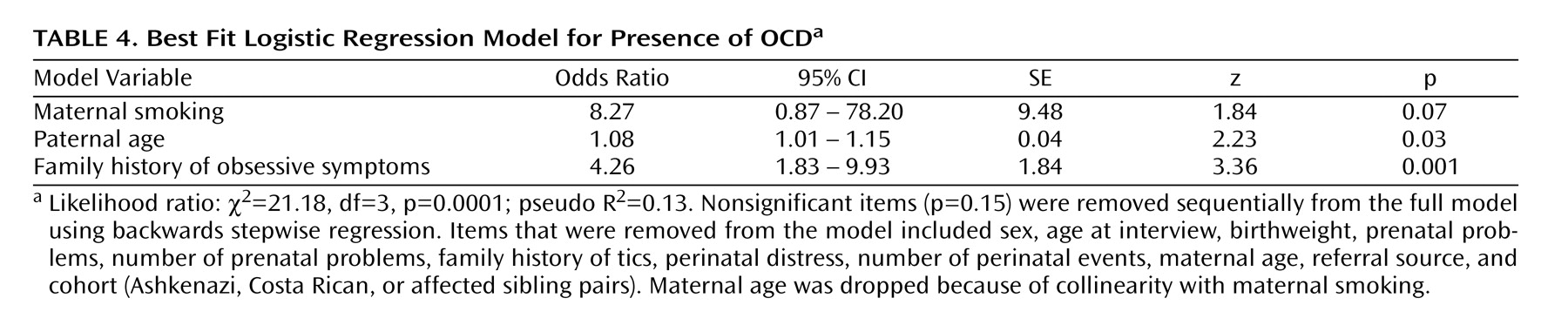
Maternal smoking was the strongest predictor of comorbid OCD, and was associated with an eightfold increase in risk (
Table 4 ). Increased paternal age was also associated with an increased risk of comorbid OCD, with an 8% higher risk for each year of the father’s age. Also included in the final model was family history of obsessive-compulsive symptoms, which was associated with a fourfold increase in the risk of comorbid OCD. No relationship between rates of OCD and other prenatal/perinatal variables, gender, study group, or age at interview was seen. A comparison of the best-fit model with and without maternal smoking using a likelihood ratio test showed that the two models were significantly different (χ
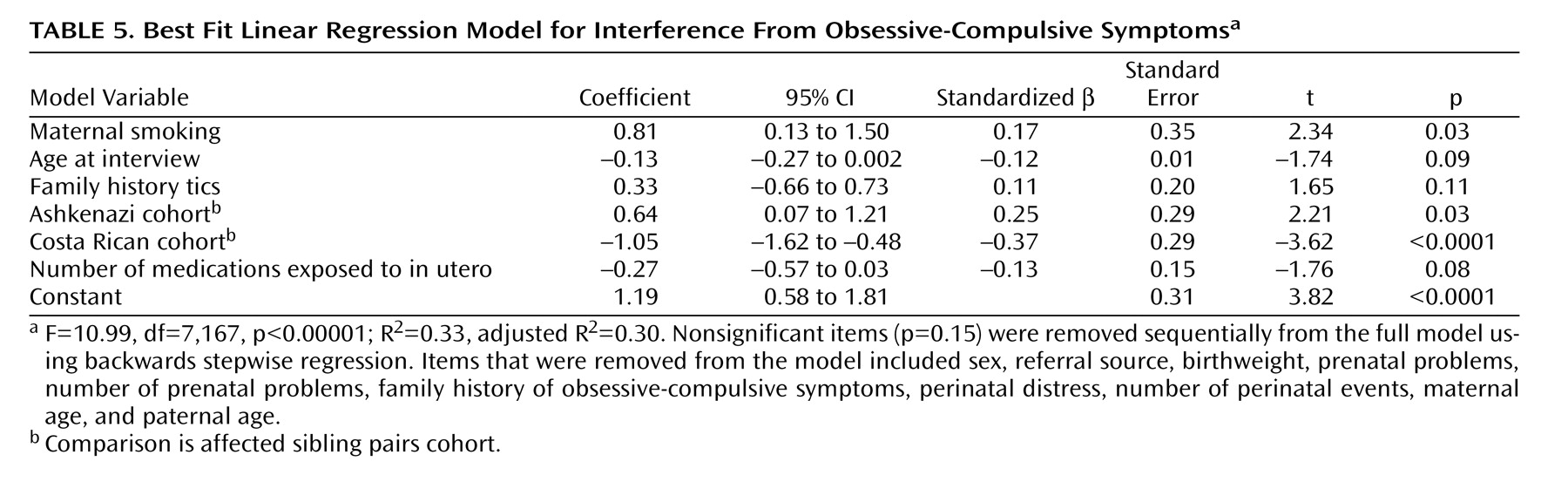
2 =4.78, df=1, p<0.03), suggesting that although not independently significant within the model, maternal smoking did significantly contribute to the overall model. Univariate analysis also showed a significant association between presence of comorbid OCD and maternal smoking (p=0.047, Fisher’s exact test). Maternal smoking was also significantly associated with interference from obsessive-compulsive symptoms, with a 0.8-point increase in Yale-Brown Obsessive Compulsive Scale
(26) interference scores (
Table 5 ). There was no association between maternal smoking and rates of subclinical obsessive-compulsive symptoms, distress caused by obsessive-compulsive symptoms, or time spent engaging in obsessive-compulsive symptoms.
ADHD and self-injurious behavior
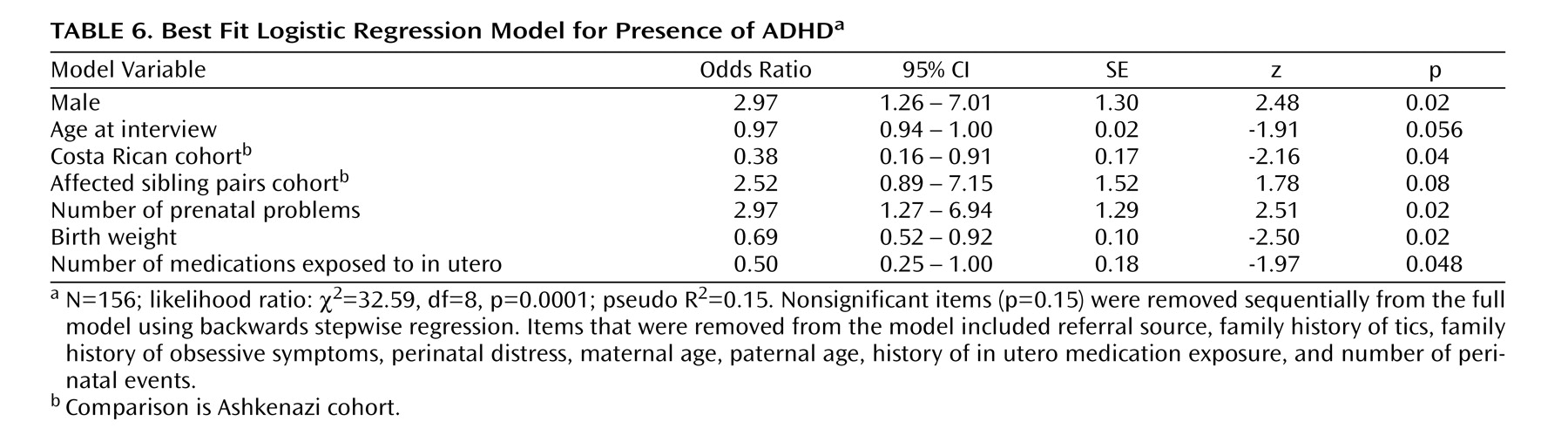
Birth weight and number of prenatal problems were both significantly associated with an increased risk of comorbid ADHD in Tourette’s syndrome (
Table 6 ). Additional risk factors included male gender, age at interview, and study group. It is surprising that in utero medication exposure was associated with a reduced risk of comorbid ADHD in our study groups. No relationship between pre- and perinatal factors and self-injurious behavior was found. There was no significant association between exposure to tobacco and presence of either ADHD or self-injurious behavior.
Discussion
This study identified maternal smoking as a strong risk factor for increased severity of clinical expression in individuals with Tourette’s syndrome, specifically for increased tic severity and risk of comorbid OCD. In utero medication exposure was also associated with increased tic severity, and increased paternal age was associated with risk of comorbid OCD. Additionally, number (but not type) of prenatal problems and lower birth weight were associated with an increased risk of comorbid ADHD.
Previous studies have suggested a range of prenatal/perinatal risk factors for increased symptom severity in Tourette’s syndrome, including chronic intermittent maternal stress, severe maternal nausea, in utero exposure to caffeine, alcohol, and tobacco, and lower birth weight
(4,
9,
12) . We hypothesized that events associated with transient fetal hypoxia such as emergency cesarean section, fetal distress, or nuchal cord would be associated with increased symptom severity, particularly with increased tic severity. The basal ganglia have been strongly implicated in the pathology and pathogenesis of Tourette’s syndrome, along with the cerebral cortex and the thalamus
(27,
28) . The basal ganglia are particularly sensitive to hypoxic injury, which has been postulated to play a role in the development of a number of movement disorders
(29 –
32) . Although there is no evidence of overt or gross damage to the basal ganglia in Tourette’s syndrome, it is possible that transient or mild hypoxia could alter gene expression and increase the predisposition to developing Tourette’s syndrome in those with a genetic vulnerability.
We found no evidence for a relationship between acute hypoxia at birth and tic severity. However, we did find evidence for a possible role of chronic fetal hypoxia secondary to nicotine exposure in increased tic severity and risk of developing comorbid OCD. Both chronic and acute nicotine exposure in utero have been consistently shown to lead to fetal hypoxia in mammals, including humans
(33 –
36) . Some effects of maternal smoking are well-known and can be seen even in infants whose mothers smoked as few as five cigarettes a day: lower birth weight, lower Apgar scores, higher risk of sudden infant death syndrome, and increase in perinatal complications such as cardio-respiratory difficulties and need for cesarean section
(34 –
37) . Effects of maternal smoking on the developing brain are less clear, although increases in perinatal neurological complications and increases in conduct, attention, and cognitive problems in children have been reported
(34,
36,
37) . As far as we know, there have been no reports of increased rates of Tourette’s syndrome among children who were exposed to nicotine in utero. However, this topic has not actively been explored. Only one of the currently published studies on environmental risk factors for Tourette’s syndrome specifically examined maternal smoking, and this study also found an increased risk for comorbid OCD
(4,
5,
9,
10,
12,
14) .
It is important to note that, although unlikely, it is possible that maternal smoking is not truly associated with increased symptom severity in Tourette’s syndrome but rather is a proxy for an associated variable that was not assessed in our study (e.g., maternal socioeconomic status, educational level, ADHD status, or maternal postnatal smoking). Maternal smoking during pregnancy is strongly associated with both lower socioeconomic status and with fewer years of education in the United States, and there are also increased rates of smoking reported in individuals with ADHD
(38 –
40) . We do not have socioeconomic or educational data on our entire dataset, but we do have these data on approximately one-third of subjects from each group (total N=66) in the form of Hollingshead scores
(41) . In these subjects, there was no association between maternal smoking and Hollingshead scores, nor between Hollingshead scores and tic severity or risk of OCD, ADHD, or self-injurious behavior, which suggests that socioeconomic status or maternal education are not likely to be risk factors for increased symptom severity in our subjects. Similarly, we have data on parental ADHD status for a small subgroup of subjects (N=25). In this group, there was no significant association between parental ADHD status and maternal smoking nor between parental ADHD status and tic severity or risk of OCD, ADHD, or self-injurious behavior. Unfortunately, we do not have data on postnatal smoking.
We also found that paternal age was associated with the risk of comorbid OCD, although not with tic severity. This finding, although unexpected, is not unprecedented; Burd et al.
(10) previously identified paternal age as a risk factor for developing Tourette’s syndrome in a large epidemiological sample. The data are equivocal, however, since two other studies found no relationship between paternal age and development of Tourette’s syndrome
(13,
42) . The mechanism of how increased paternal age might contribute to increased risk of Tourette’s syndrome or increased symptom severity is unclear. Increased paternal age is associated with decreased birth weight and increased rates of multiple births in population samples and may act as a proxy for either or both
(10,
43) . Although we did find an increase in the rate of multiple births (5% in our cohort versus 1%–2% average incidence in the United States), we found no association between multiple births and any of our outcome measures
(44) . Similarly, we did not find a relationship between tic severity and decreased birth weight, although we did find a relationship between increased risk of comorbid ADHD and decreased birth weight
(4,
5) . In light of the equivocal evidence for increased paternal age or decreased birth weight as risk factors for either the development of Tourette’s syndrome or increased symptom severity, further study is needed before any conclusions can be drawn.
Relationship Between Gender and Adverse Perinatal Events
We also hypothesized that male subjects in our cohort would have an increased rate of adverse prenatal/perinatal events. This has been seen previously, and studies have suggested an interaction between gender and environmental factors in Tourette’s syndrome expression
(9,
12) . Instead, we found that female subjects had higher rates of adverse perinatal events, specifically rates of unplanned/emergency cesarean section, although this finding was not statistically significant when corrections were made for multiple testing. We also found no evidence for an interaction between gender and any prenatal/perinatal event and symptom severity, although male gender was an independent risk factor for both increased tic severity and risk of comorbid ADHD but not for risk of comorbid OCD. Male and female subjects in our study were, in fact, remarkably similar in clinical expression, with no significant differences in tic severity or rates of OCD, ADHD, or self-injurious behavior. This finding is also unexplained and requires replication.
Limitations
Because this was an exploratory study, with retrospective data collection, the findings require replication, preferably in a prospectively collected cohort of Tourette’s syndrome patients and a comparable group of subjects without Tourette’s syndrome. The primary limitation for this study is the possibility of recall and ascertainment bias. In particular, because of increased knowledge about Tourette’s syndrome, subjects in the United States may have been more likely to look for environmental risk factors in their histories than were those from Costa Rica, where awareness of Tourette’s syndrome is not as high
(19) . Although ascertainment and recall bias are risks in all retrospective studies, our method of data collection was rigorous and comparable to those used in other studies
(4,
5,
9,
12) . In addition, epidemiological studies have shown that maternal recall for pregnancy-related events is quite good, even after 30 years. In particular, maternal recall for smoking has a sensitivity of 0.86 and a specificity of 0.94 when compared to obstetric chart data
(45) .
We also controlled for bias in our data analysis. Differences in ascertainment most likely accounted for differences in symptom severity and exposure to pre- and perinatal adverse events between subject groups. We controlled for these differences by including both subject group and referral source as covariates in all analyses. In addition, our statistical approaches ensured that variables that did not contribute significantly to the model, including potential confounding variables, were removed as appropriate.
The age range of our subjects is another potential limitation. Sixty percent of our subjects were <14 at the time of interview and may have been too young to exhibit clinically significant obsessive-compulsive symptoms. The fact that we found a significant association between maternal smoking and comorbid OCD is even more striking in this context, however, and suggests that there may be a stronger relationship than we were able to identify. The age range for our subjects was less of an issue for comorbid ADHD, since only 5% of our subjects were <7 at the time of interview.