Patients experiencing a first episode of psychosis have a better therapeutic response to antipsychotic medications than do chronic, multiepisode patients
(1,
2) . Despite this good clinical response, however, the majority of first-episode patients discontinue their initial antipsychotic medication, often not continuing treatment with another medication
(1 –
3), which places them at high risk of psychotic relapse and clinical deterioration
(4) .
Comparative studies of atypical versus conventional antipsychotics in patients with first-episode psychosis demonstrate reduced extrapyramidal side effects and equal or slightly superior efficacy for the atypical antipsychotics
(5 –
10) . First-episode patients respond to lower doses and demonstrate a greater sensitivity to antipsychotic treatment-related side effects
(6,
7,
11) than do multiepisode patients.
Few studies have compared atypical antipsychotics to determine their relative effectiveness in a first-episode population. Studies comparing olanzapine and risperidone in first-episode patients suggest similar efficacy for the two treatments, with few extrapyramidal side effects, although olanzapine is associated with more weight gain
(12,
13) . Preliminary noncomparative studies suggest that quetiapine is efficacious and well-tolerated in first-episode patients
(14 –
16) . The purpose of this study was to determine the overall effectiveness of quetiapine relative to two established standards, olanzapine and risperidone, in patients early in the course of psychotic illness. The primary outcome measure was the percentage of patients discontinuing their assigned antipsychotic (all-cause treatment discontinuation) during the 52 weeks of treatment. This measure integrates the efficacy and tolerability of each drug over time. The primary hypothesis was that quetiapine was not inferior to olanzapine or risperidone in the rate of all-cause treatment discontinuation in early-psychosis patients. No prior data suggested that superiority for quetiapine was a likely outcome.
Previous studies suggested that first-episode patients receive good therapeutic benefit from olanzapine with doses in the range of 10–15 mg/day
(6) and that the effectiveness of risperidone may be reduced by extrapyramidal side effects if doses exceed 2–4 mg/day
(3,
5,
9) . Given quetiapine’s low liability for extrapyramidal side effects, we speculated that doses up to 800 mg/day would be tolerable in our study population.
Secondary measures of psychopathology, quality of life, and side effects were obtained to delineate differential effects of each drug on efficacy, tolerability, and safety.
Method
Study Design
This was a 52-week randomized, double-blind, flexible-dose, multicenter study of patients early in the course of schizophrenia, schizoaffective disorder, or schizophreniform disorder assigned to treatment with olanzapine, quetiapine, or risperidone.
Study Population
Participants were recruited from inpatient, outpatient, and emergency department services for the evaluation and treatment of psychosis. The study was approved by the institutional review board at each site, and written informed consent was obtained from the patients or their legally authorized representatives. Patients had to be able to participate in the informed consent process or have a legal guardian available to provide informed consent. Consenting patients 16–40 years of age were eligible for the study if they met DSM-IV criteria for schizophrenia, schizophreniform disorder, or schizoaffective disorder. Patients had to be in the first episode of their psychotic illness and had to have been continuously ill for at least 1 month and no more than 5 years. Patients were excluded if a prior psychotic episode had remitted for 3 months or more or if they had prior antipsychotic drug treatment for more than 16 cumulative weeks. All patients had a score ≥4 on at least one Positive and Negative Syndrome Scale (PANSS;
17 ) psychosis item (delusions, conceptual disorganization, hallucinatory behavior, grandiosity, or suspiciousness/persecution) and a score ≥4 (moderately ill) on the severity item of the Clinical Global Impression scale (CGI;
19 ) at the point of maximum severity of illness to date. Female participants of childbearing potential had to be using a medically acceptable form of contraception.
We excluded patients who did not speak English; had a history of mental retardation; were pregnant or nursing; had a serious, unstable medical illness; had a known allergy to one of the study medications; were at serious risk of suicide; or had participated in an investigational drug trial within 30 days before the first treatment visit.
Study Treatments
Patients were randomly assigned to treatment with olanzapine (2.5–20 mg/day), quetiapine (100–800 mg/day), or risperidone (0.5–4 mg/day). On days 1 and 2, each patient received one capsule of olanzapine (2.5 mg), quetiapine (100 mg), or risperidone (0.5 mg) in the evening. At the treating physician’s discretion, the dose could be increased by one capsule every other day—i.e., on days 3 and 4, one capsule in the morning and one in the evening; on days 5 and 6, one capsule in the morning and two in the evening; and so on, up to a maximum of four capsules twice daily.
Any previous antipsychotic therapy was tapered and discontinued during the first 2 weeks of double-blind treatment, and no subsequent use of an additional antipsychotic was permitted. Treatment with an adjunctive antidepressant or mood stabilizer during the first 8 weeks of treatment was not allowed unless approved by the project medical officer. Anticholinergic medications for acute extrapyramidal side effects were permitted for up to a total of 2 weeks over the course of the trial. Clinicians were encouraged to lower the dose of antipsychotic to relieve extrapyramidal side effects. Otherwise, adjunctive medications (prescribed to address an aspect of psychopathology inadequately controlled by the assigned antipsychotic) and concomitant medications (prescribed to treat a side effect or a comorbid medical illness) could be used without restriction. When an adjunctive or concomitant medication was prescribed, its name, modal dose, and indication (selected from forced-choice lists) were recorded.
Assessments
The screening evaluation included a diagnostic interview (the Structured Clinical Interview for DSM-IV
[18] ), medical history, physical examination, measurement of vital signs, and laboratory tests. Confirmation that the illness met clinical severity criteria was established by a modified, abbreviated version of the PANSS that included items P1–P6 and rated symptom severity at the point of maximum severity of illness.
Study visits occurred at baseline, at weekly intervals for the first 6 weeks, every other week for the next 6 weeks, and monthly thereafter. All clinical and laboratory assessments were obtained at baseline, week 12, and week 52 or when the patient terminated the study before week 52. Measures of psychopathology, function, tolerability, and safety were completed at intermediate visits as specified in a schedule of events for the study.
The primary outcome measure was the proportion of patients who withdrew from the study prior to 52 weeks of treatment (“all-cause pharmacological treatment discontinuation”). The reason for discontinuation was recorded according to a predetermined algorithm: 1) administrative discontinuation due to an independent external event (e.g., moving with family to another state); 2) a clinician decision to discontinue treatment because of inadequate therapeutic effect or intolerable side effects whether or not the patient wanted to discontinue; or 3) a patient decision to discontinue although the clinician believed the treatment to be adequately efficacious, tolerable, and safe.
Efficacy was measured in two domains: 1) psychopathology and 2) social and occupational functioning. Psychopathology was assessed by the PANSS, the CGI, and the Calgary Depression Scale for Schizophrenia
(20) . Social and occupational functioning was assessed with the Heinrichs-Carpenter Quality of Life Scale
(21) . Clinical response was defined as a score ≤3 on all PANSS items and ≤3 on the CGI severity item at any time during the trial.
The number of pills taken was determined by pill counts, and use of concomitant or adjunctive medication was recorded at each study visit. The modal dose for each patient within a treatment group was the dose prescribed for that patient on the maximum number of days during the trial. The mean modal dose for each treatment group was defined as the mean of the modal doses prescribed for the patients assigned to that treatment.
Clinicians rated the severity of 19 medication-related elicited adverse events on a checklist at each visit. Severity of akathisia was determined with the Barnes Akathisia Rating Scale
(23), parkinsonian signs with the Simpson-Angus Scale
(22), and dyskinetic movements with the Abnormal Involuntary Movement Scale
(19) . The most severe scores recorded at any time during the study period are reported.
Laboratory tests evaluated glucose, lipids, and prolactin levels. At each blood draw, the patient’s report of the number of hours since consumption of any food or caloric drink was recorded. Fasting was defined as no caloric consumption for 8 or more hours prior to the blood draw. Weight and waist circumference were recorded.
Statistical Analysis
The protocol-designated primary hypothesis was that quetiapine was not inferior to olanzapine or risperidone in the rate of all-cause treatment discontinuation in early-psychosis patients. The primary hypothesis was tested with the protocol-designated statistical analysis of Blackwelder’s
(24) noninferiority normal approximation method with a noninferiority margin of 0.20 (20%), using a significance level of 0.025 for each of the two pairwise comparisons. All analyses were specified in a statistical analysis plan that was finalized before the blind was broken. Kaplan-Meier survival curves and a log-rank test were used to assess time to discontinuation. Pairwise comparisons of time to discontinuation between treatments were performed using the log-rank test.
Baseline measures of demographic and clinical characteristics were compared using Fisher’s exact test for categorical variables or a Kruskal-Wallis test for continuous variables. Efficacy measures (PANSS, Calgary Depression Scale for Schizophrenia, CGI, and Heinrichs-Carpenter Quality of Life Scale) were tested using a mixed random coefficients model with fixed effects for treatment, baseline, and center and with random effects for the intercept and log (time).
Efficacy analyses used a modified intent-to-treat population, defined as patients who were randomly assigned to a treatment and returned for at least one postrandomization assessment. Baseline descriptive statistics are presented using the intent-to-treat population, which contained all patients who underwent random assignment to a treatment.
Postbaseline rates of elicited adverse events were compared using Fisher’s exact test. Between-groups differences that met the significance threshold of p≤0.05 are reported without adjustment for multiple comparisons. Because extrapyramidal side effects were minimized by reducing the antipsychotic dose as soon as possible when symptoms appeared, the scores reported for the Simpson-Angus Scale, the Abnormal Involuntary Movement Scale, and the Barnes Akathisia Rating Scale represent worst-case postbaseline values. These were compared using Fisher’s exact test for categorical variables and the Kruskal-Wallis test for continuous variables. Changes in continuous measures of weight, body mass index (BMI), waist circumference, and metabolic parameters were analyzed using a mixed model similar to that used for the efficacy measures, while changes in categorized measures of these parameters were analyzed using logistic regression with treatment as the predictor.
Sensitivity analyses for secondary variables were performed using last observation carried forward and observed case analyses to investigate whether the results of the mixed models were similar to those obtained using the observed case and last observation carried forward methods. All analyses of efficacy, weight, and metabolic measures were tested at the nominal significance threshold of p≤0.05, without adjustment for multiple comparisons.
Results
Baseline Characteristics
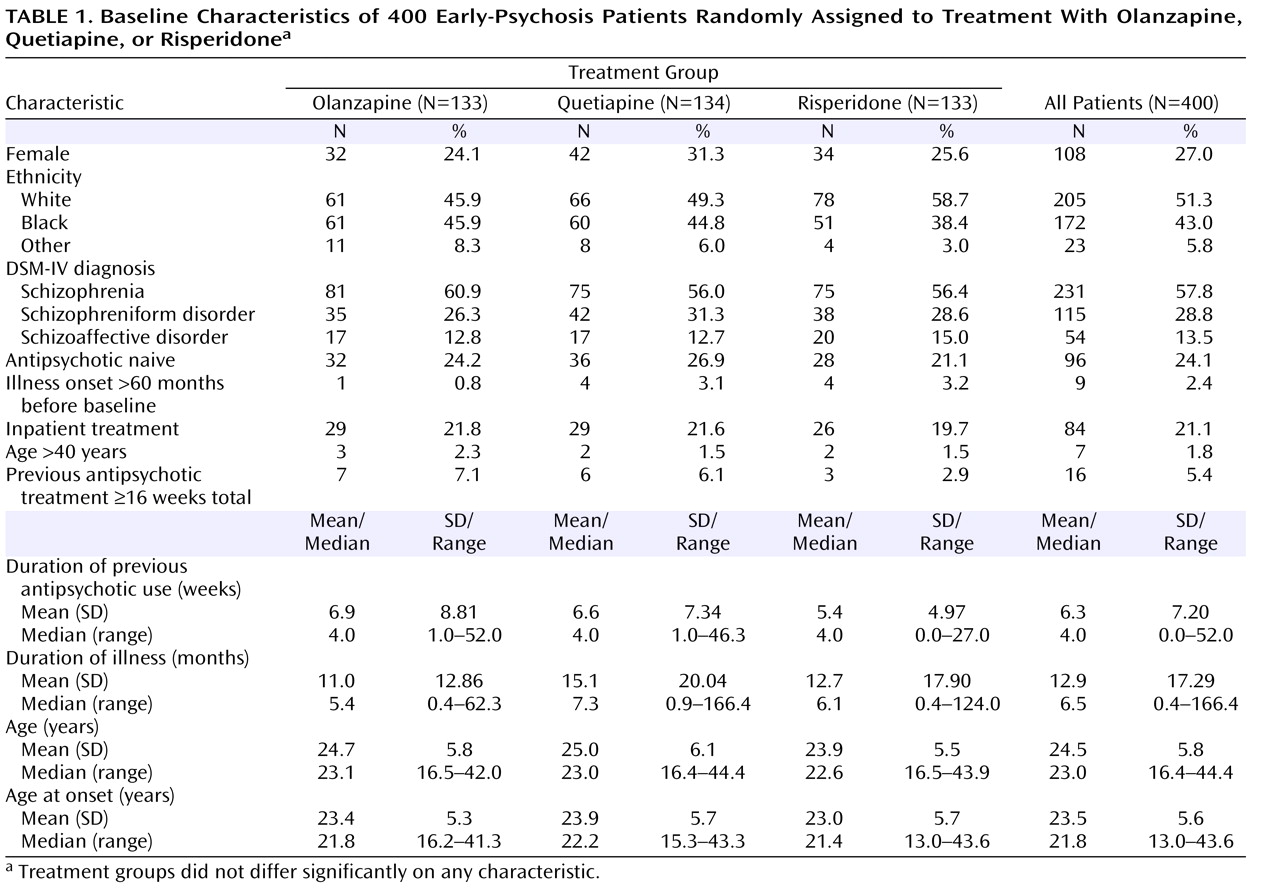
Table 1 presents demographic and clinical characteristics for the three treatment groups and the whole cohort. There were no significant differences between treatment groups. Patients showed moderate levels of psychopathology at baseline, with a mean total score of 73.8 (SD=15.8) on the PANSS, a mean score of 4.3 (SD=0.8) on the CGI severity item, and a mean total score of 13.0 (SD=4.2) on the Calgary Depression Scale for Schizophrenia. After case-by-case discussions with site investigators, the project medical officer (J.P.M.) allowed the enrollment of nine patients who had been ill for more than 60 months, seven patients who were over 40 years of age, and 16 patients who had taken antipsychotics for more than 16 weeks.
Pharmacological Treatments
The mean modal number of capsules prescribed per day was 4.7 (SD=2.1) for olanzapine, 5.1 (SD=2.2) for quetiapine, and 4.7 (SD=2.0) for risperidone, which resulted in a mean modal prescribed daily dose of 11.7 mg (SD=5.3) for olanzapine, 506 mg (SD=215) for quetiapine, and 2.4 mg (SD=1.0) for risperidone. Over the course of the trial, 19% of patients in the olanzapine group, 20% of patients in the quetiapine group, and 11% of patients in the risperidone group were brought to the maximum allowed dose of four capsules twice daily.
During the study, patients received adjunctive medications mainly for dysphoria/depression (25.7%), anxiety (16.5%), insomnia (15.2%), and agitation/excitement (9.9%). There were no significant differences in postbaseline adjunctive medication use between treatment groups.
Primary Outcome Measure
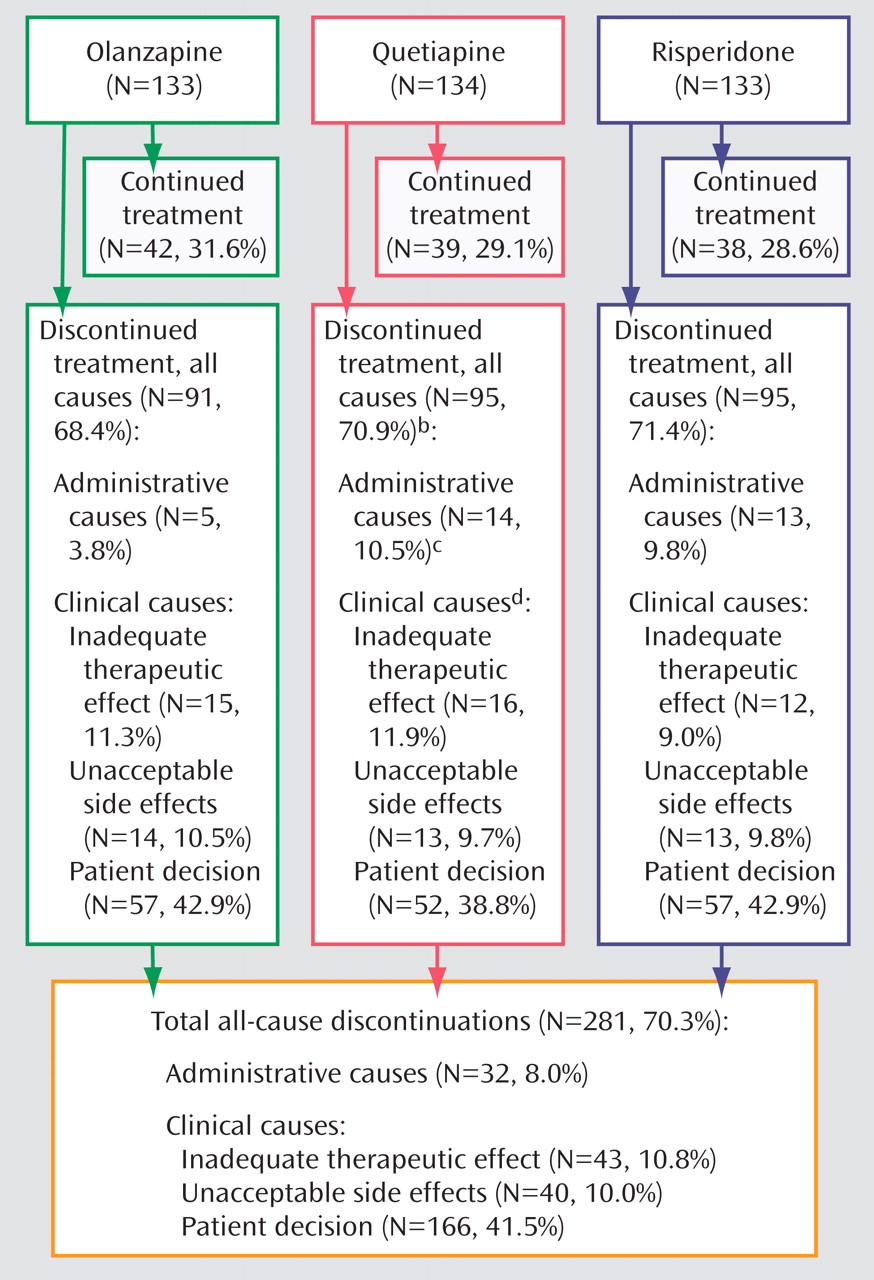
Figure 1 shows rates of all-cause treatment discontinuation across the three treatment groups. Overall, 70% of patients discontinued treatment before 52 weeks: 68.4% of those assigned to olanzapine, 70.9% of those assigned to quetiapine, and 71.4% of those assigned to risperidone. Based on the prespecified primary outcome measure of a 20% margin for clinically significant inferiority, quetiapine proved noninferior to olanzapine or risperidone. The absolute difference between quetiapine and olanzapine was 2.5%, with an upper-bound one-sided 97.5% confidence interval (CI) of 13.5%, while the absolute difference between quetiapine and risperidone was 0.5%, with an upper-bound one-sided 97.5% CI of 10.3%. Patients receiving olanzapine had fewer administrative discontinuations (3.8%) than those receiving quetiapine (10.5%) or risperidone (9.8%), but there were no other notable differences across the treatment groups in reasons for discontinuation. The most frequent reason for discontinuation across the entire study population was patient decision despite the recommendations of the treating clinician to continue treatment (41.5%). Only 10.8% discontinued because of inadequate therapeutic effect, and only 10.0% because of intolerable side effects.
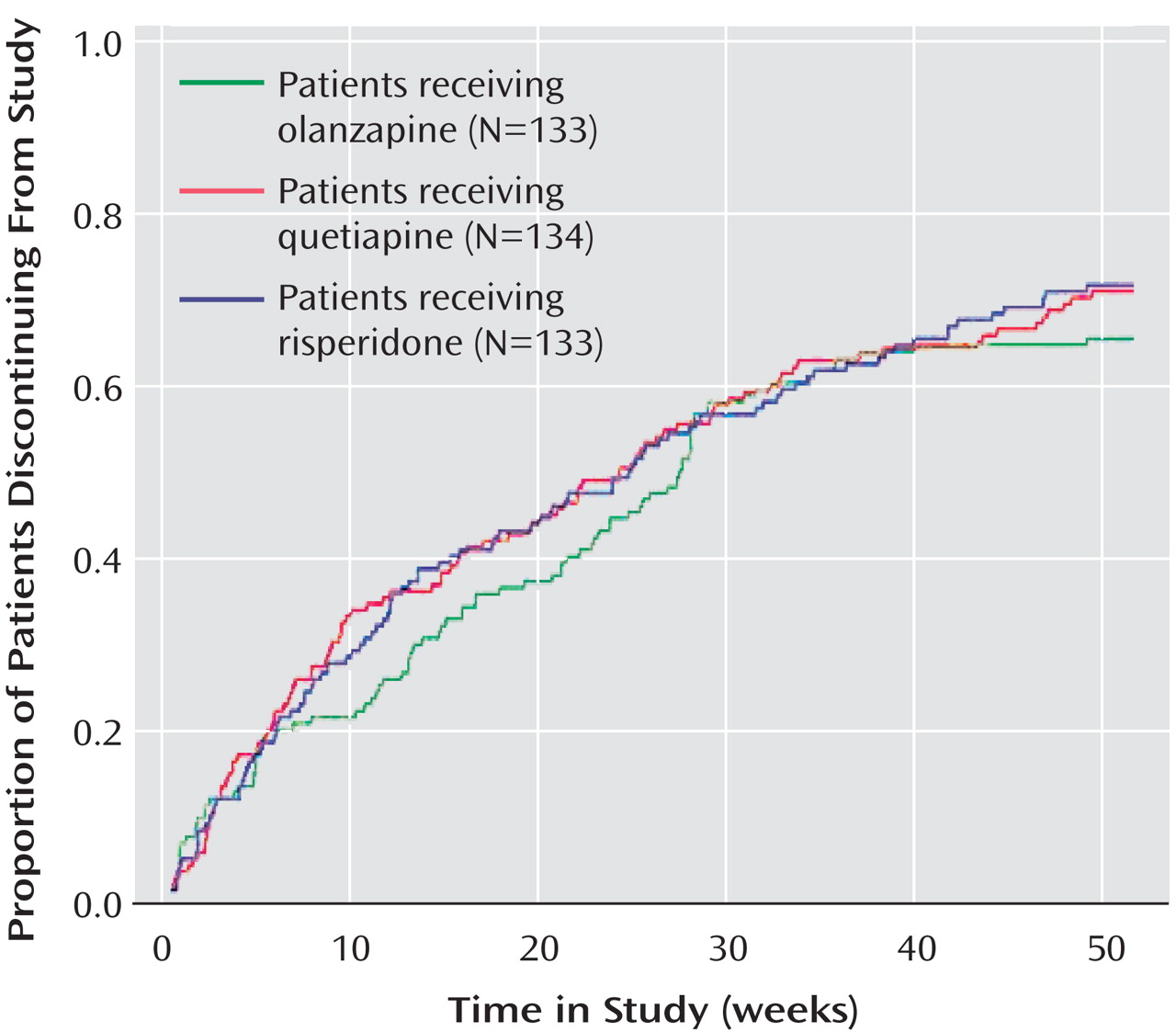
Figure 2 displays the survival curves to all-cause treatment discontinuation. The median times to all-cause discontinuation for olanzapine (28 weeks), quetiapine (25 weeks), and risperidone (25 weeks) did not differ significantly.
Secondary Outcome Measures
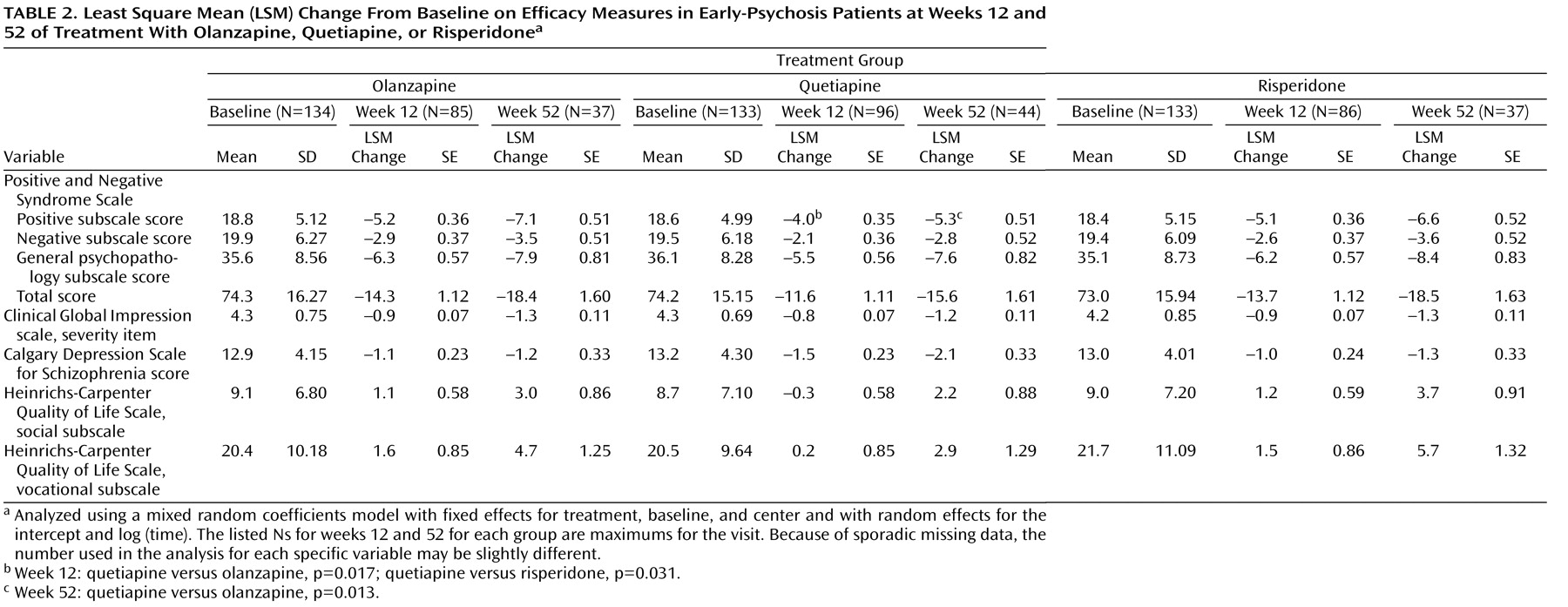
Table 2 presents the least square mean change from baseline scores on efficacy measures at 12 and 52 weeks. All treatment groups showed improvements in symptoms, with no significant differences across groups in PANSS total scores. At 12 weeks, the mean change from baseline in the PANSS positive subscale scores showed greater reductions for olanzapine (–5.2) and risperidone (–5.1) than for quetiapine (–4.0; quetiapine versus olanzapine, p=0.017; quetiapine versus risperidone, p=0.031), but this significant difference persisted only with olanzapine at week 52 (–5.3 for quetiapine versus –7.1 for olanzapine, p=0.013). On all other measures, the three treatment groups did not differ significantly.
Sixty-four percent of patients in the olanzapine group, 58% of patients in the quetiapine group, and 65% of patients in the risperidone group met the treatment response criteria (≤3 for all PANSS items and ≤3 for the CGI severity item) at some point during the study. The rates of response were not significantly different between the treatment groups.
Safety and Tolerability
Adverse Events
A total of 18 serious adverse events occurred, four in the olanzapine group and seven each in the quetiapine and risperidone groups. These events included two suicide attempts and one alleged homicide in the olanzapine group, two completed suicides and one case of suicidal ideation in the quetiapine group, and one suicide attempt in the risperidone group.
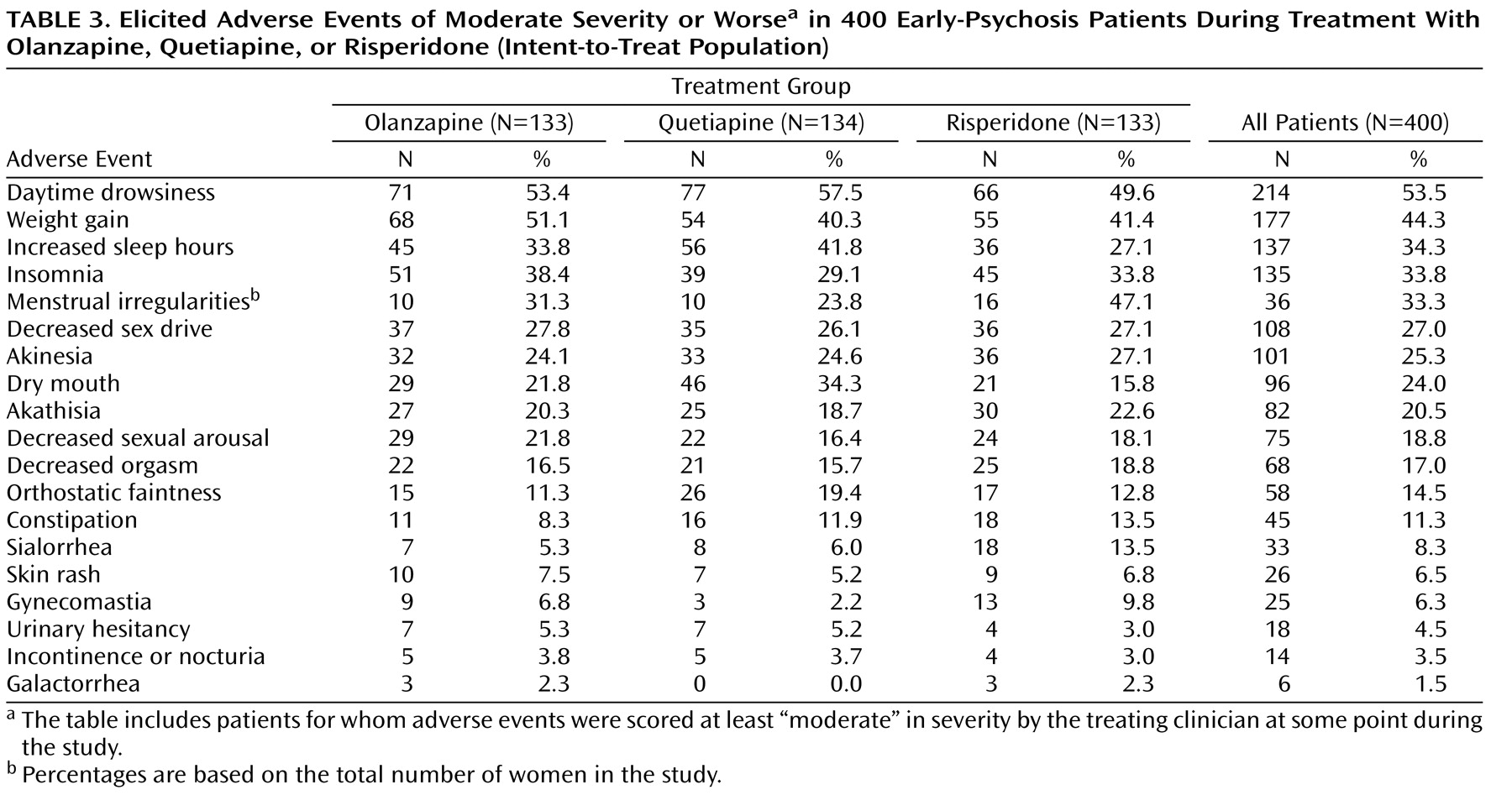
The rates of elicited adverse events that clinicians scored as moderate or severe are presented in
Table 3 . The most frequent adverse events in the olanzapine group were daytime drowsiness (53%), weight gain (51%), and insomnia (38%); in the quetiapine group, daytime drowsiness (58%), increased sleep hours (42%), and weight gain (40%); in the risperidone group, daytime drowsiness (50%), menstrual irregularities in women (47%), and weight gain (41%). Dry mouth was more common in the quetiapine group than in the other two groups. Sialorrhea was more common in the risperidone group than in the other two groups. Gynecomastia was more common in the risperidone group than in the quetiapine group. Hypersomnia was more common in the quetiapine group than in the risperidone group.
Extrapyramidal Symptoms
Over the course of the trial, only 16% of patients had a rating >1 (mild) on any Simpson-Angus Scale item, only 7% had a rating >2 (mild) on the global severity item of the Barnes Akathisia Rating Scale, and only 1% had a score >2 (mild) on the global severity item of the Abnormal Involuntary Movement Scale. There were no significant differences across treatment groups. The proportion of patients receiving concomitant medications for parkinsonism or akathisia was lower in the quetiapine group (4%) than in the olanzapine group (11%, p=0.021).
Physical Measures and Laboratory Tests
Weight and BMI
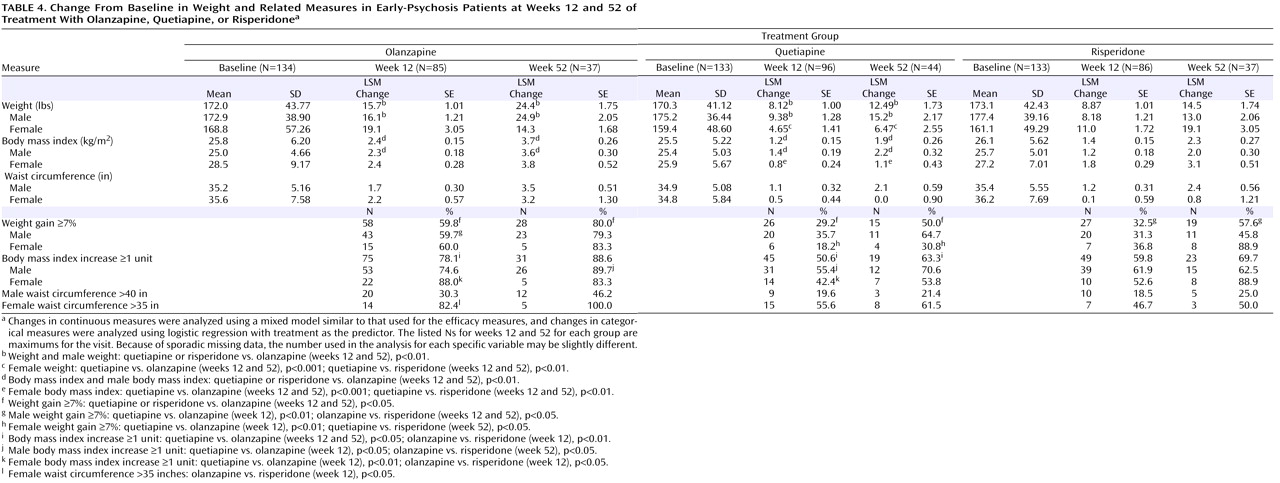
Olanzapine was associated with the greatest increases in body weight and related measures (
Table 4 ). At week 12, the olanzapine group had more weight gain, a greater increase in BMI, and a higher proportion of patients with a BMI increase of at least 1 unit compared with the quetiapine and risperidone groups. Similar differences between olanzapine and quetiapine or risperidone were also observed at week 52 except in the proportion of patients with a BMI increase of at least 1 unit in the risperidone group. Furthermore, 80% of patients in the olanzapine group had gained ≥7% of their baseline weight at week 52, compared with 50% and 58% of the quetiapine and risperidone groups, respectively (observed cases). Risperidone was associated with greater increases than quetiapine in weight and BMI in women (p<0.01).
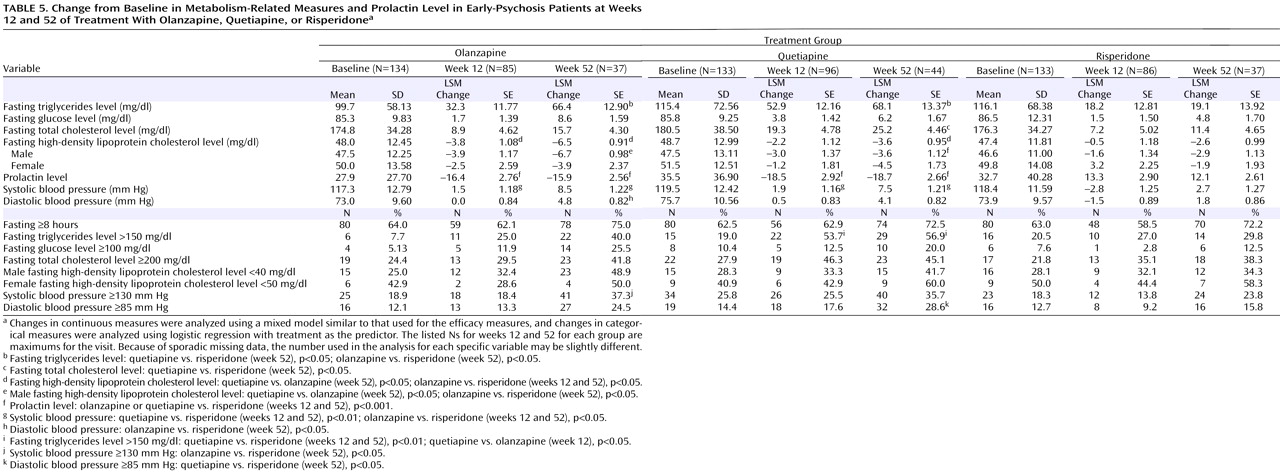
Metabolic Measures
Of the three drugs, risperidone was associated with the smallest elevations in fasting levels of triglycerides and cholesterol and the smallest reduction in high-density lipoprotein cholesterol level (
Table 5 ).
Prolactin
Patients in the risperidone group had greater increases in prolactin levels than those in the olanzapine and quetiapine groups at weeks 12 and 52 (
Table 5 ).
Discussion
This is the first double-blind randomized clinical trial comparing three atypical antipsychotics in patients early in the course of psychotic illness. We evaluated the overall effectiveness of olanzapine, quetiapine, and risperidone in 400 patients over a 52-week period, with the rate of all-cause treatment discontinuation as the primary outcome measure. All-cause discontinuation rates were comparable for all three drugs, and quetiapine was noninferior to olanzapine and risperidone. In order to test noninferiority, one must test the null hypothesis that the standard treatment is better than the experimental treatment by at least some specified amount. The specified amount in this study, 20%, was the margin of difference in discontinuation rates that was pragmatically testable within the available budget and sample size parameters; smaller prespecified margins would have required unattainable sample sizes. Our results suggest that the differences in discontinuation rates between these three treatments are much smaller than 20%.
There were no significant differences between groups in PANSS total score or percentages of patients meeting predetermined treatment response criteria. However, greater reductions were seen in positive symptom subscale scores at 12 weeks in the olanzapine and risperidone groups than in the quetiapine group, and this advantage persisted with olanzapine at 52 weeks. A similar slight advantage for risperidone on the PANSS positive symptom subscale was seen in another recently reported trial
(25) . These results suggest that quetiapine, although comparably effective in the treatment of patients early in the course of schizophrenia, schizoaffective disorder, or schizophreniform disorder as assessed on global measures, may be somewhat less potent than olanzapine and risperidone at the doses administered in this study.
Previous studies suggesting that first-episode patients receive therapeutic benefit from antipsychotic doses lower than those required for chronic patients and that first-episode patients develop unnecessary extrapyramidal side effects at higher doses led us to use lower dose ranges of olanzapine and risperidone in this study than those used in the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE). However, given quetiapine’s low extrapyramidal side effects liability, we expected that the quetiapine doses used in CATIE would be tolerable in our study population. This may have been a factor in the comparable effectiveness demonstrated by quetiapine. In the CATIE phase 1 and phase 2 schizophrenia trials
(26 –
28), higher mean modal doses of olanzapine and risperidone but similar mean modal doses of quetiapine were used; in these trials, olanzapine and, less consistently, risperidone proved to be more effective than quetiapine. It remains an empirical question whether higher doses will improve the relative effectiveness of quetiapine in chronic patients.
First-episode patients with psychotic illness tend to be treatment responsive
(5,
6,
8,
29) . Overall, 62% of our study population met response criteria at some point during the trial (64%, 58%, and 65% in the olanzapine, quetiapine, and risperidone groups, respectively), as indicated by mild or absent positive, negative, or mood symptoms and a global rating of illness severity as mild or less. While clinical improvement was good, these patients were sensitive to medication side effects. Moderate to severe daytime drowsiness, increased sleep hours, weight gain, and menstrual irregularities were commonly experienced. It is possible that these treatments would have been associated with less sedation if olanzapine and risperidone had been given as a single bedtime dose. Over half of patients who remained in treatment with any of these agents at 1 year gained more than 7% of their body weight. Weight gain was more prominent and more likely in the olanzapine group, which is consistent with findings from other studies. Extrapyramidal side effects were uncommon and not severe, probably because low doses of olanzapine and risperidone were used.
Patients early in the course of psychotic illness (and their families) who are willing to participate in a trial such as this one may represent an especially insightful and agreeable subgroup of early-psychosis patients. Still, about 70% of patients in this study discontinued prior to 1 year. More than half of the discontinuations were against the preferences of the treating clinicians, indicating a need to improve methods of preemptively identifying and addressing patients’ reasons for leaving treatment
(3,
9) .
Overall, five patients made suicide attempts, of which two resulted in completed suicides. These events occurred despite the close attention provided in clinical research aftercare programs.
Since our primary aim was to test the durability of the study drugs over time rather than to measure change from a carefully determined baseline, we allowed patients who had some prior antipsychotic treatment to participate. Thus, our study population may differ in baseline characteristics from populations in some first-episode studies.