It is now well documented that major depressive disorder is one of the most common mental disorders in adolescence (e.g., references
1–
3). Given the high prevalence of major depressive disorder in adolescence, examining the natural course of episodes in this age group is clearly important. In a previous study
(4), we found that individuals who had experienced an episode of major depressive disorder by age 19 were at significantly elevated risk for future major depressive disorder, compared to participants with adolescent-onset nonmood disorders and adolescents with no disorder. In these three groups, rates of major depressive disorder over the 5-year period from age 19 through 23 were 45.0%, 28.2%, and 18.5%, respectively. In addition, compared to no-disorder comparison subjects, formerly depressed adolescents had significantly higher rates of nonmood disorder in the follow-up period (33.2% versus 19.5%). The primary purpose of the study reported here was to identify the factors in formerly depressed adolescents that predict major depressive disorder recurrence in young adulthood.
To our knowledge, only six studies have examined predictors of recurrence of major depressive disorder in depressed children or adolescents. Five studies examined patient groups
(5–
9), and one examined the offspring (6–23 years of age) of adults treated for depression
(10). The results of these studies are inconsistent, perhaps because of the generally small size of the study groups and the considerable variation in participants’ ages, duration of the follow-up periods, treatment settings, and assessment methods.
The framework that guides our research is based on an integrative, multifactorial model
(11), in which depression is conceptualized as the end result of environmentally initiated changes in behavior, affect, and cognitions. The model distinguishes between antecedents, which occur before the onset of the depression, and consequences, which are observable during and after an episode of depression and which may influence the risk of recurrence. Antecedents examined in the study reported here included having lived in a stressful environment during adolescence (e.g., a nonintact household, a high level of conflict with parents, stressful life events). The model also recognizes individual differences (vulnerabilities and protective factors) that increase or decrease the impact of the antecedent events and moderate the impact of the consequences of depression on recurrence. Vulnerabilities examined in this study included psychopathology among family members, female gender (which has often been shown to be a risk factor), elevated level of depression symptoms, depressotypic cognitions, and excessive emotional reliance. Protective factors included self-rated social competence and positive coping skills. The model, like most other current theories of the etiology of depression, does not distinguish between first onset and recurrent episodes of depression, even though the results of other studies
(12–
14) have suggested that these two types of episodes may be predicted by different variables.
Consistent with the expectation that having experienced an episode of depression creates vulnerabilities that effect recurrence, clinical aspects of the episode of major depressive disorder in adolescence (e.g., early onset, longer duration, recurrence during adolescence, greater severity, treatment utilization, and suicide attempts) were hypothesized to be associated with recurrence. Comorbid adolescent psychopathology was also hypothesized to be a vulnerability for recurrence. Last, traits measuring selected young adult personality disorders (i.e., antisocial and borderline personality disorders) were posited to reflect stable characteristics of the person that constitute vulnerabilities for recurrence.
This study focuses on individuals who experienced and recovered from an episode of major depressive disorder during adolescence, which we defined as before age 19. On the basis of their psychiatric outcome between age 19 and 23, individuals were assigned to four mutually exclusive groups: 1) those with no further disorder, 2) those with a recurrent episode of major depressive disorder but no comorbid mental disorder, 3) those with a recurrent episode of major depressive disorder that was accompanied by a nonmood disorder, and 4) those with no recurrence of major depressive disorder but who experienced a nonmood disorder.
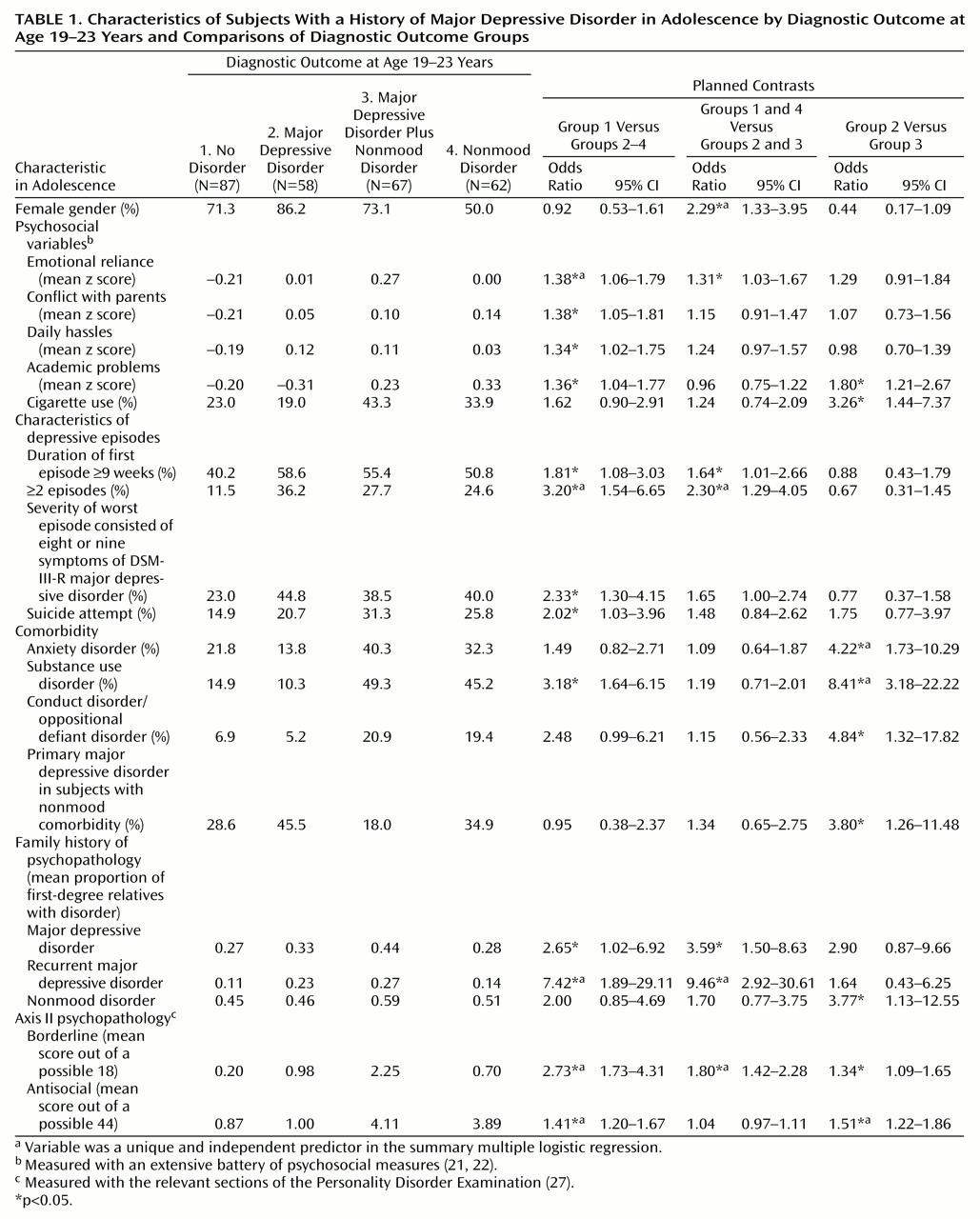
This design allowed us to address three questions. First, what factors predict staying well (group 1 versus groups 2, 3, and 4). Second, what factors predict major depressive disorder recurrence (groups 1 and 4 versus groups 2 and 3). Third, what factors predict pure (i.e., noncomorbid) major depressive disorder versus major depressive disorder with a co-occurring nonmood disorder (group 2 versus group 3).
Method
Participants
Probands
Participants were a subset of individuals from the Oregon Adolescent Depression Project. Participants were originally randomly selected from nine senior high schools in western Oregon. A total of 1,709 adolescents (ages 14–18; mean age at initial assessment=16.6 years, SD=1.2) completed the initial assessment (time 1), which consisted of an interview and questionnaires, between 1987 and 1989. Approximately 1 year later (time 2), 1,507 participants (88.2%) participated in a reassessment that used the same interview questions and questionnaires (mean interval between time 1 and time 2=13.8 months, SD=2.3) (additional details are provided elsewhere
[2]).
As probands from the Oregon Adolescent Depression Project reached their 24th birthday, participants with a history of major depressive disorder at time 2 (N=360), those with a history of nonmood disorder at time 2 (N=284), and a subset of those with no history of mental disorder at time 2 (N=457) were invited to participate in a time 3 interview. The no-disorder comparison group was representative of the entire group of participants with no mental disorder at time 2 (N=863) in age and gender within age; all participants with nonwhite ethnicity were invited to participate in the time 3 assessment.
Of the 1,101 young adults selected for time 3 interview, 940 participated (85.4%). Of those participants, 57.2% were female, 89.0% were white, 34.1% were married, 96.8% had graduated from high school, and 31.4% had a bachelor’s degree or a higher educational level. Their average age at time 3 was 24.2 years (SD=0.6). Women were more likely than men to complete the time 3 assessments (88.9% versus 81.0%) (χ2=13.55, df=1, N=1,101, p<0.001). Differences in time 3 participation as a function of other demographic characteristics or time 2 diagnostic status were nonsignificant.
A total of 315 time 3 participants had experienced an episode of major depressive disorder before age 19. Forty-one of these participants were deselected to better clarify the predictors of major depressive disorder recurrence between age 19–23: 22 were experiencing the major depressive disorder episode at the time of their 19th birthday, three met criteria for bipolar disorder after age 19, three met criteria for dysthymia but not major depressive disorder after age 19, and 13 met criteria for adjustment disorder with depressed mood but not for major depressive disorder after age 19. Thus, the reference group for the present study consisted of 274 participants who had experienced and recovered from an episode of major depressive disorder by age 19.
Family members
Lifetime psychiatric information was obtained from the first-degree relatives over the age of 13 (biological parents, full siblings) of the Oregon Adolescent Depression Project participants in the time 3 assessment. To supplement the direct interviews, informant psychiatric data were collected from probands or another first-degree relative. Our goal was to collect diagnostic data from two sources for each family member. Diagnostic information was available for the relatives of 234 of the 274 probands with a history of major depressive disorder during adolescence (85.4%). Of the 761 first-degree relatives for whom diagnostic information was collected, direct interviews were obtained for 442 (58.1%); data for 145 (19.1%) of the family members were based on a single source.
After a thorough description of the study, written informed consent was obtained from Oregon Adolescent Depression Project probands (and their guardians, if applicable) and from the family members.
Diagnostic Interviews
Oregon Adolescent Depression Project probands
Participants were interviewed at time 1 with a version of the Schedule for Affective Disorders and Schizophrenia for School-Age Children (K-SADS) that combined features of the epidemiologic version
(15) and the present episode version and included additional items to derive DSM-III-R diagnoses. At time 2 and time 3, participants were interviewed with the Longitudinal Interval Follow-Up Evaluation
(16), which elicited detailed information about the course of psychiatric symptoms and disorders since the previous interview. Time 3 interviews were conducted by telephone, and time 3 diagnoses were made by using DSM-IV criteria.
Most diagnostic interviewers had an advanced degree in clinical or counseling psychology or social work, and all were extensively trained before data collection. Interrater reliability for lifetime diagnoses in a randomly selected subsample at time 1 (N=233) was moderate to excellent: kappa=0.86 for major depressive disorder, and kappa=0.76–0.89 for nonmood disorder categories. For a randomly selected subsample at time 3 (N=178), interrater reliability was excellent for the primary categories of major depressive disorder (kappa=0.87) and nonmood disorder (kappa=0.82).
Family members
Parents and siblings were interviewed with either the Structured Clinical Interview for DSM-III-R, Nonpatient Version (SCID-NP)
(17) or the K-SADS employed in the time 1 proband assessment, modified for collection of DSM-IV criteria. Family history data were collected by using the revised Family Informant Schedule and Criteria
(18), which is based on the Family History Research Diagnostic Criteria
(19), modified for DSM-IV criteria. Using all available data, the project’s four senior diagnosticians (P.R., D.N.K., P.M.L., and Nicholas Allen), who were blind to proband diagnoses, derived best-estimate diagnoses
(20) for relatives.
Outcome Variable: Psychopathology in Early Adulthood
The primary outcome variable used in this study was the development of another episode of major depressive disorder during early adulthood. The 274 formerly depressed participants were categorized into four groups: 1) no disorder, consisting of 87 participants (31.8%) who experienced neither major depressive disorder nor a nonmood disorder from age 19 through 23; 2) major depressive disorder, consisting of 58 participants (21.2%) who had a recurrence of major depressive disorder by age 24 but no nonmood disorder during the 19–23 age period; 3) major depressive disorder plus nonmood disorder, consisting of 67 participants (24.5%) who had a recurrence of major depressive disorder and experienced a nonmood disorder during the 19–23 age period; and 4) nonmood disorder, consisting of 62 participants (22.6%) who experienced a nonmood disorder but did not have a recurrence of major depressive disorder during the 19–23 age period. Of the 129 participants with a nonmood disorder during the 19–23 age period, 99 (76.7%) had a diagnosis of substance use disorder, 44 (34.1%) anxiety disorder, three (2.3%) oppositional defiant disorder, three (2.3%) conduct disorder, two (1.6%) eating disorder, one (0.8%) schizophreniform disorder, and one (0.8%) somatoform disorder. The majority of these nonmood disorder episodes (58.1%) were new disorders that began after age 19 (i.e., did not represent the continuation of a nonmood disorder that began before age 19 and persisted into the 19–23 age period). Twenty-two of the 274 participants (8.0%) were experiencing a current major depressive disorder episode at the time 1 assessment; differences in diagnostic outcome as a function of time 1 current major depressive disorder status were nonsignificant (χ2=3.39, df=3, N=274, n.s.).
Predictor Variables
Demographic characteristics
Four dichotomous time 1 variables were included: 1) gender; 2) family intactness (living with versus not living with both biological parents); 3) highest parental education within the household (bachelor’s degree versus less than a bachelor’s degree), which was included as a proxy measure of socioeconomic status; and 4) ethnicity (white or nonwhite).
Psychosocial variables
An extensive battery of psychosocial measures was administered at time 1 to all participants. All measures had been previously shown to possess very good psychometric properties
(21,
22)). Variables were standardized and scored such that higher values reflected more problematic functioning.
Current depression was assessed by using the 20-item National Institute of Mental Health Center for Epidemiologic Studies Depression Scale (CES-D Scale)
(23) (alpha=0.89; time 1–time 2 r=0.61) (df=1505, p<0.001 for all correlations). Negative cognitions were assessed with 27 items on self-reinforcement, likelihood of future positive events, dysfunctional attitudes, and perceived control over one’s life (alpha=0.81; time 1–time 2 r=0.61). Attributional style was assessed with the 48-item Kastan Attributional Style Questionnaire for Children (N. Kaslow, R.L. Tanenbaum, M.E.P. Seligman, unpublished 1978 questionnaire) (alpha=0.63; time 1–time 2 r=0.55). Self-esteem was assessed with nine items on physical appearance and general self-esteem (alpha=0.81; time 1–time 2 r=0.62). Excessive emotional reliance was assessed with 10 items on the extent to which the individual desires excessive support and approval from others and is interpersonally sensitive (alpha=0.83; time 1–time 2 r=0.54). Self-rated social competence was assessed with 12 items (alpha=0.85; time 1–time 2 r=0.64). Coping skills were assessed with 17 items (alpha=0.76, time 1–time 2 r=0.55). Social support from friends was assessed with 13 items (alpha=0.81, time 1–time 2 r=0.60). Social support from family was assessed with 22 items (alpha=0.86, time 1–time 2 r=0.64). Conflict with parents was assessed with the 45-item Issues Checklist scale
(24) (alpha=0.81; time 1–time 2 r=0.51). Daily hassles were assessed with 20 items from the Unpleasant Events Schedule
(25) (alpha=0.79; time 1–time 2 r=0.55). Major life events were assessed by using questions about 11 negative life events involving self or significant other (parent, sibling, other relative, close friend) during the past year (alpha=0.78; time 1–time 2 r=0.52). Academic problems were assessed with nine items from the questionnaire and the time 1 K-SADS interview (e.g., lifetime occurrence of school expulsion or suspension, truancy, repeating a grade in school, most recent grade point average). Physical illness at time 1 was assessed by using 90 items on physical symptoms, number of sick days, and physician visits during the past year. Cigarette use was assessed in the time 1 K-SADS interview with a question about whether the participant had been a daily cigarette smoker.
Adolescent major depressive disorder
The following six characteristics of adolescent major depressive disorder were included in the analysis: 1) age at onset of first major depressive disorder episode before age 13 years (N=47 of 274, 17.2%) versus at age 13 or older, 2) duration of the first major depressive disorder episode of 2–8 weeks (N=136 of 274, 49.6%) versus 9 or more weeks, 3) single major depressive disorder episode before age 19 (N=207 of 274, N=75.5%) versus two or more episodes, 4) severity of the worst episode indicated by the presence of five to seven DSM-IV symptoms (N=175 of 274, 63.9%) versus eight or nine symptoms, 5) treatment utilization (outpatient or inpatient treatment or medications) for major depressive disorder during adolescence (N=58 of 274, 21.2%) versus no treatment, and 6) history of a suicide attempt during adolescence (N=62 of 274, 22.6%) versus no attempt.
Psychiatric comorbidity during adolescence
Four categories of comorbid psychiatric disorders occurring before age 19 were examined: 1) dysthymia (N=20 of 274, 7.3%), 2) anxiety disorders (N=74 of 274, 27.0%), 3) substance use disorder (N=80 of 274, 29.2%), and 4) conduct disorder/oppositional defiant disorder (N=35 of 274, 12.7%). For the 143 participants with nonmood comorbidity during adolescence, the major depressive disorder episode was categorized as either primary (N=42, 29.4%) or secondary (N=101, 70.6%) on the basis of the age at onset of the two disorders; primary major depressive disorder could not be determined for eight participants due to simultaneous onset with the nonmood disorder.
Family history of psychopathology
Three variables were included as indications of the degree of psychopathology in the family: 1) the proportion of first-degree relatives (parents and siblings) with major depressive disorder, 2) the proportion of relatives with recurrent major depressive disorder, and 3) the proportion of relatives with nonmood disorder.
Personality disorders
The two most frequent and relevant DSM-IV personality disorders (antisocial and borderline) were assessed by using relevant portions of the Personality Disorder Examination
(26). Personality Disorder Examination dimensional scores (i.e., summation of partial and full symptom criteria) were used in the analyses. The interrater reliability of the Personality Disorder Examination dimensional scores was excellent (intraclass correlation coefficients>0.80).
Statistical Analyses
To address the three primary questions posed in this study (What are the predictors of staying well, of major depressive disorder recurrence, and of pure depression?), three multiple logistic regression analyses were conducted with each potential predictor variable. The first multiple logistic regression analysis compared the no-disorder control group to the remaining three outcome groups (i.e., major depressive disorder, major depressive disorder plus nonmood disorder, and nonmood disorder). The second multiple logistic regression analysis identified the predictors of major depressive disorder recurrence by comparing participants who experienced major depressive disorder (i.e., the groups with major depressive disorder and with major depressive disorder plus nonmood disorder) with those who did not (i.e., the groups with no disorder and with nonmood disorder). The third multiple logistic regression analysis compared predictors of pure major depressive disorder versus comorbid major depressive disorder plus nonmood disorder. To test for possible moderating effects of gender, gender was entered in the model in a second block within each multiple logistic regression analysis, and the predictor-by-gender interaction term was entered in the third block. By using variables that emerged as significant univariate predictors of the specific contrast, three summary multiple logistic regression models with the likelihood ratio backward selection procedure were conducted to identify unique predictors (i.e., variables that remained significant when controlling for other variables in the model).
The strength of the associations is illustrated by the odds ratio with 95% confidence interval (CI). For the examined contrasts and for interactions with gender, with alpha set to 0.05, statistical power was sufficient (>0.80) to detect medium effect sizes or larger (Cohen’s w>0.30). Although numerous tests were performed, thereby inflating the type I error rate, statistical significance was based on p<0.05 to identify predictors of potential clinical relevance.
Discussion
Formerly depressed adolescents who developed psychiatric problems during young adulthood were characterized during adolescence by more severe depressive episodes (e.g., longer episode duration, multiple episodes, greater number of symptoms, history of suicide attempts); by elevated stress, conflict, and interpersonal dependency; and, for males only, by a negative attributional style. These individuals also had an elevated rate of substance use disorder during adolescence, and, as young adults, they showed traits associated with borderline and antisocial personality disorder. In addition, their parents and siblings were more likely to have experienced both single-episode and recurrent major depressive disorder. Variables that independently contributed to the prediction of psychopathology in young adulthood included emotional reliance, multiple depressive episodes, a family history of recurrent major depressive disorder, borderline and antisocial personality disorder symptoms, and attributional style (for males). Excessive emotional reliance is a component of the broader construct of interpersonal dependency
(27), which has been implicated theoretically in the etiology of depression, especially in the psychoanalytic literature (e.g., references
28,
29). We previously reported that excessive emotional reliance predicted depression onset in adolescents
(22) and that emotional reliance remained elevated after major depressive disorder recovery
(30). The results reported here indicate that emotional reliance is also predictive of the recurrence of psychopathology, particularly of major depressive disorder, underscoring both the centrality of emotional reliance to depression theory and its potential explanatory breadth to other disorders.
Variables that specifically predicted major depressive disorder recurrence included multiple depressive episodes in adolescence, a family history of recurrent major depressive disorder, borderline personality disorder symptoms, and, for females only, increased conflict with parents. Gender was retained in the multivariate solution, but this finding appeared to be due to the greater likelihood that formerly depressed male adolescents would develop pure nonmood disorders in young adulthood. These findings suggest that clinical characteristics, both of the proband and of the first-degree relatives, are among the strongest predictors of major depressive disorder recurrence.
There was no evidence that adolescent comorbidity acted as a risk factor for pure major depressive disorder in young adulthood. The presence of nonmood disorders in adolescence predicted nonmood disorders in young adulthood, generally comorbid with recurrent major depressive disorder. Contrary to previous research (e.g., references
7,
10), comorbid dysthymia in the present study failed to predict major depressive disorder recurrence. Unlike previous research on the impact of double depression (i.e., major depressive disorder superimposed on a preexisting dysthymia), adolescent major depressive disorder and dysthymia in the present study occurred largely at different periods. Additional research is needed to disentangle whether concurrent comorbidity of major depressive disorder and dysthymia specifically confers a risk for major depressive disorder recurrence.
Familial psychopathology was a significant predictor in all three contrasts. Most significantly, the proportion of family members with recurrent major depressive disorder predicted major depressive disorder recurrence in the offspring, with and without a nonmood disorder. These findings are consistent with previous research indicating that the presence of major depressive disorder in family members significantly increases the likelihood of major depressive disorder recurrence in adults (e.g., references
31–
34). The results reported here extend previous research by indicating that recurrent depression breeds true from parent to offspring.
Both elevated antisocial and borderline personality disorder symptoms were significant in multiple contrasts. Several adult studies have suggested strong comorbidity between depression and borderline personality disorder symptoms (e.g., references
35–
38) and a small number of studies of adult patients have shown that axis II pathology, especially cluster B disorders (i.e., antisocial, borderline, narcissistic, histrionic), increases the likelihood of depression recurrence in treated adult patients (e.g., references
39–
41). Our findings on axis II psychopathology need to be qualified in two respects. First, rates of personality disorders were low, so elevated dimensional scores were generally in the subthreshold range. Second, the data on axis II psychopathology were obtained at time 3. Therefore, the direction of these associations cannot be determined, although previous research supports the hypothesis that adolescent depression precedes the onset of personality disorder symptoms
(42).
The majority of psychosocial variables assessed during adolescence were not found to predict recurrence of psychopathology, including negative cognitions, self-esteem, social skills, coping, life events, social support, and elevated depression symptoms (as measured by the CES-D Scale). The most plausible explanation for these nonsignificant findings is that their prognostic impact in previous studies was time limited. Thus, the extent to which a variable’s predictive ability diminishes as a function of time needs to be explored in future research. A second explanation is that the assessment of these variables in the design of the study reported here may have occurred before, during, or after the adolescent major depressive disorder episode.
A depressotypic attributional style predicted future psychopathology in formerly depressed young men. There is a large literature, conducted primarily with adults, examining the role of depressotypic cognitions in predicting recurrence. The findings of these studies are mixed, with some investigations reporting significant results (e.g., reference
43) and others reporting nonsignificant effects (e.g., reference
41). Important issues that need to be addressed in future research concern whether depressotypic cognitions are measured at intake or at the end of treatment, whether results obtained with adults are replicated in samples of adolescents and children, and whether the cognitions specifically predict depression.
A number of limitations of the present study should be acknowledged. Given the absence of previous research in this area, a stringent correction for type I error was not applied, and the results need to be considered preliminary pending independent replication. Second, although a relatively large number of predictors were examined, some potentially important categories of predictors (e.g., biological measures, childhood physical and sexual abuse) were not represented. Third, although our sample was community based, which reduced a number of selection biases, the sample selection may also limit the applicability of our findings to clinical practice. Offsetting these limitations were several noteworthy strengths of this study, including the large sample size, prospective design, rigorous diagnostic interviews, and assessment of a broad array of predictors, including direct interview data on family history of psychopathology. Overall, the findings support arguments by Warner et al.
(10), Ilardi et al.
(41), and Goodyer et al.
(44) that the predictors of depression onset, duration (persistence), and recurrence may differ in important ways.
The clinical implications of this study are straightforward. Clinicians are routinely faced with decisions about what to do with youngsters with a history of major depressive disorder. We previously demonstrated that all individuals with a history of major depressive disorder during adolescence are at very high risk for major depressive disorder recurrence and for other psychiatric disorders during young adulthood
(4). In the study reported here, roughly one-fourth of formerly depressed adolescents experienced subsequent pure major depressive disorder, one-fourth experienced comorbid major depressive disorder, and one-fourth remained free from depression recurrence but experienced a nonmood disorder. Earlier and better identification of the most salient risk factors is the first step in avoiding a protracted course of disorder. Depressed female adolescents (especially those who experience high conflict with parents), adolescents with multiple major depressive disorder episodes, and adolescents with a family history of recurrent depression are at particularly high risk for depression recurrence and should be closely monitored or receive continued prophylactic treatment. The association between recurrent depression and borderline personality disorder features indicates that individuals with recurrent depression may warrant additional treatment focused on emerging axis II psychopathology.