Our patient had no previous history of psychiatric illness until age 52. He was seen with auditory hallucinations, thought broadcasting, and other paranoid delusions. His medical history was remarkable for a seizure disorder. His neuropsychological performance did not suggest dementia. He was treated with an antipsychotic, an antidepressant, and an anticonvulsant but ultimately seemed to benefit most from antipsychotic medication. He developed the symptoms of tardive dyskinesia within a year of treatment with haloperidol decanoate. Approximately 6 years after the onset of his psychiatric symptoms, our patient experienced remission of his psychiatric symptoms, and his psychotropic medications were discontinued. Nearly 4 years later, at the time of this report, he continued to function independently, with no psychiatric symptoms, but he still had some persistent extrapyramidal symptoms and tardive dyskinesia.
Diagnostic Implications
Our patient’s differential diagnosis included the following:
1. Psychotic disorder due to a general medical condition (seizure disorder). Our patient’s history and the results of a physical examination and laboratory assessments provided no evidence of any medical condition that likely caused his psychotic illness other than seizure disorder.
An increased incidence of psychotic symptoms in patients with seizure disorders has been observed for more than a century
(14). Mesial temporal lobes are often implicated in the psychopathology of schizophrenia and are also a frequent point of origin for complex partial seizures
(15). There is a higher risk of schizophrenia in patients with complex partial seizures than in those with generalized tonic-clonic seizures
(16). Psychosis may follow the onset of epilepsy, during an interval ranging from 14 to 21 years
(15). Some researchers have hypothesized that complex partial seizures may induce a neurologic reorganization that subsequently predisposes patients to psychosis
(17).
Our patient’s seizures were, however, of the grand mal type, and his last known seizures occurred 23 years before the onset of his psychotic symptoms. While he may have continued to experience subtle seizures, the results of a recent EEG did not suggest an ongoing seizure disorder. Finally, antipsychotics, rather than anticonvulsants, proved to be the best treatment for his psychotic symptoms. Our patient’s seizure disorder (or its underlying neuropathological cause) might have made him vulnerable to subsequent psychosis, but a diagnosis of psychosis secondary to a seizure disorder would be difficult to justify in this case.
2. Dementia of the Alzheimer’s type with delusions and hallucinations. Psychotic symptoms that first appear in late life may be symptoms of Alzheimer’s disease or other dementing disorders
(18). Our patient’s neuropsychological performance was, however, not consistent with that of Alzheimer’s disease. One of the hallmarks of Alzheimer’s disease is rapid forgetting, but our patient showed consistently normal retention of material, once learned, on measures of memory. In fact, his neuropsychological performance and his everyday functioning improved when his status was assessed over several years.
3. Brief reactive psychosis. Although our patient’s incarceration constituted a significant stressor in his life and was concurrent with the onset of his psychotic symptoms, he continued to experience symptoms years after his release. The persistence and duration of his psychotic symptoms precluded this diagnosis.
4. Factitious disorder or “hysterical psychosis” (19). It is possible that the onset of our patient’s psychosis was related to a conscious or unconscious motivation to gain early release from incarceration. Such motivation would suggest a diagnosis of factitious disorder, conversion reaction, or dissociative disorder. Yet our patient demonstrated improvement with treatment while incarcerated. In addition, he served his entire sentence and, in fact, experienced a severe psychotic episode and decline in function a year after his release. While the patient might have had a primary or secondary gain from the development of psychosis while incarcerated, there were no obvious environmental reasons for chronicity or eventual remission.
5. Mood disorder with psychotic features. Our patient never met the DSM-IV criteria for a manic or hypomanic episode or for major depressive episode. His affect was typically described as blunted or flat. There was no history of marked mood fluctuations.
6. Delusional disorder. Bizarre delusions, including thought insertion and prominent auditory hallucinations, ruled out this condition.
7. Schizophrenia. Onset of our patient’s psychotic symptoms at age 52 would have excluded this diagnosis in DSM-III, which explicitly prohibited the diagnosis of schizophrenia in cases with onset of prodromal symptoms after age 45. DSM-III-R permitted a diagnosis of late-onset schizophrenia in such cases. The DSM-IV criteria have no restrictions or specifiers based on age at onset, although the construct of late-onset schizophrenia has remained somewhat controversial
(20–
24).
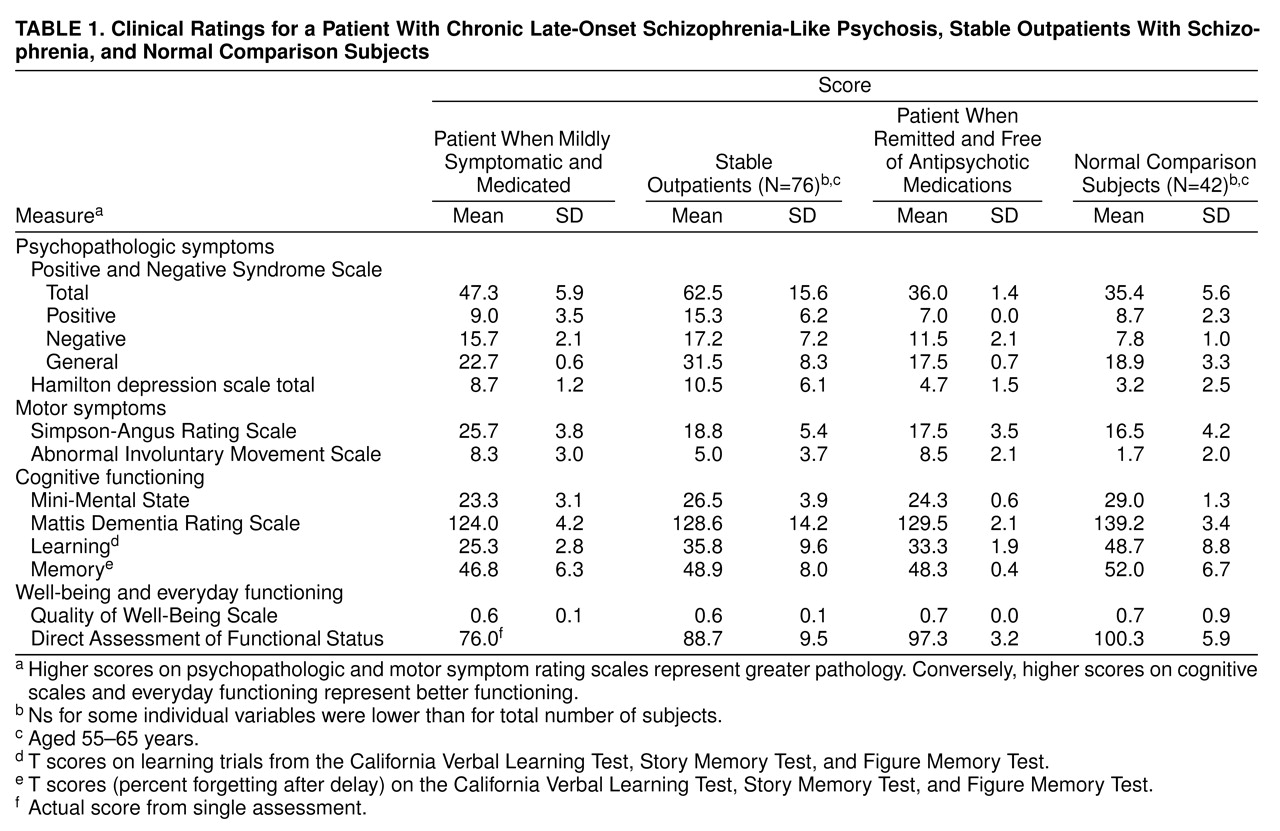
Clinically, our patient seemed to meet the DSM-IV criteria for schizophrenia. As a medicated and mildly symptomatic outpatient, his ratings for psychopathologic symptoms, well-being, and everyday functioning were similar to those of other clinically stable outpatients with schizophrenia. As his symptoms remitted, however, our patient’s scores on these scales became similar to those of normal comparison subjects. While chronicity is the rule in schizophrenia, several investigators have found that as many as 20% of such patients experience remission in late life
(25,
26). Certain factors have reportedly been associated with a positive long-term outcome in schizophrenia
(27,
28). Our patient had several of these characteristics, including good premorbid adjustment, acute onset of psychosis, and early intervention with antipsychotic medications. His neuropsychological performance was similar to that seen in patients with schizophrenia rather than to that of patients with Alzheimer’s disease.
Our patient’s psychosis differed from that found in typical schizophrenia in several important ways. He had no family history of schizophrenia and had apparently normal premorbid functioning. A major stressor precipitated his first psychotic episode, and after discharge from the hospital, he did well in the absence of neuroleptic treatment for a year. His subsequent remission resulted in a return to completely normal premorbid functioning, without any of the “stigmata” of chronic schizophrenia. The confluence of all of these unusual features suggests that a diagnosis of late-onset schizophrenia-like psychosis might be appropriately less specific than that of schizophrenia.
8. Psychotic disorder not otherwise specified. Our patient could be given a diagnosis of psychotic disorder not otherwise specified since he did not fit the typical pattern of any common psychotic disorder. This diagnosis is one of exclusion, however, and does not help explain the nature of his illness.
Comparisons Between the Psychotic Illnesses of Newton and Our Patient
Any comparisons of the psychotic illnesses of Newton and our patient are severely limited because we have very poor documentation of the onset, nature, and course of Newton’s symptoms. Nonetheless, at least superficially, there are several interesting parallels between our patient’s psychosis and that reportedly exhibited by Newton. One is the lack of previous symptoms until a psychotic breakdown in their early 50s. A second similarity is the predominance of persecutory delusions. Newton believed that his friends and colleagues were trying to smear his reputation or were otherwise conspiring to hurt his position, and he made reference to conversations that never occurred. He angrily confronted his colleagues about this through his letters. Our patient believed that his neighbors were talking about him, and he actually confronted some individuals, which resulted in an altercation.
Another similarity is the murky nature of the etiology of the psychosis. In both cases there were suggestions of possible organic contributions (metal poisoning for Newton and seizure disorder for our patient), yet on close inspection, the organic explanations seemed unable to fully account for the psychosis. Thus, certain features that would have strongly supported a diagnosis of psychosis secondary to a general medical condition were absent (e.g., Newton did not exhibit the common signs of metal poisoning, and our patient’s history and EEG results did not suggest complex partial seizures). In both cases there were significant psychosocial stressors that might have precipitated the initial psychosis (Newton had experienced a breakup in a close personal relationship and also had professional problems, and our patient was incarcerated).
Finally, both men experienced total remission of their symptoms after months or years of psychotic illness and returned to their premorbid levels of functioning, with little evidence of residual symptoms.
There are, however, some important differences between these two cases. Our patient’s symptoms included auditory hallucinations, bizarre delusions (thought insertion and thought broadcasting), and negative symptoms, including blunted affect and paucity of thought content. Since the records of Newton’s symptoms consist primarily of letters to and among his acquaintances, it is difficult to know whether he experienced hallucinations and other delusions. Furthermore, while the precise onset of Newton’s psychosis is not clear, it appears that his symptoms spontaneously remitted in less than 18 months. In contrast, our patient did not experience full remission until 6 years after his initial episode, despite treatment with antipsychotics.
Relatively little research has been done on chronic late-onset psychotic disorders in patients without dementia or mood disorders. We believe that a proportion of such patients do have late-onset schizophrenia
(22–
24), whereas others have delusional disorder or other DSM-IV-defined primary psychotic disorders. There remain subgroups of patients, however, whose diagnostic categorization is uncertain. The use of terms such as “paraphrenia” or “psychotic disorder not otherwise specified” is unhelpful because these terms do not shed light on the nature of these psychotic disorders. The diagnosis of paraphrenia has been used so inconsistently over the years that it does not appear to have a clear meaning
(29). When Kraepelin
(30) used the term “paraphrenia,” his concept (which made no reference to age at onset) involved a form of psychosis in which patients manifested hallucinations and delusions, but other aspects of their mental functioning and personality were relatively spared. Roth
(31) introduced the term “late paraphrenia” in the 1950s to refer to paranoid psychosis with onset after age 65. However, both terms (“paraphrenia” and “late paraphrenia”) were sometimes used as if they were synonymous with “late-onset schizophrenia.” Some prominent investigators in the United Kingdom, where this terminology has been historically more popular, have recently abandoned the term “paraphrenia” because of a lack of known distinct etiologic or treatment implications (Robert Howard, personal communication, August 1999).
Our patient would appear to meet the DSM-IV criteria for schizophrenia with late onset. In Newton’s case, the available information is inadequate to make a DSM-IV diagnosis. We would, however,
not recommend a diagnosis of late-onset schizophrenia in either individual because of the temporally circumscribed nature of the psychosis, in which both men had relatively normal premorbid and postmorbid functioning. (Patients with late-onset schizophrenia tend to have somewhat subnormal premorbid functioning and generally have a chronic course of illness without full remission.) For the lack of a better term, one may call the disorder “late-onset schizophrenia-like psychosis.” Patients with such a disorder expose the limitations of our present diagnostic systems and call for more research on psychotic disorders with late-life onset that do not fit nicely into the standard nosologic schemas
(24).