An early clinical characterization of panic attacks, called the “phobic anxiety-depersonalization syndrome,” described panic and depersonalization symptoms that typically occurred after a traumatic experience or severe stressor and eventually evolved into agoraphobia
(1). In DSM-IV, panic disorder is the only anxiety disorder (not related to trauma) that has a dissociative symptom—derealization or depersonalization—as a criterion, although the diagnosis may also be given in the absence of depersonalization or derealization.
A history of physical and sexual abuse during childhood has been linked both to increased dissociative tendencies in adults
(2,
3) and to increased rates of panic disorder
(4–
6). However, only a subgroup of panic patients experience depersonalization or derealization during panic attacks. We therefore hypothesized that individuals with prominent depersonalization/derealization during panic are more likely to have a history of significant childhood trauma than individuals without such symptoms. To our knowledge, this study is the first to examine this relationship.
METHOD
Seventy-four outpatients aged 18–65 years entering a clinical trial of fluoxetine, imipramine, or placebo for panic disorder completed assessments for both childhood trauma and panic symptoms before study treatment, after providing written informed consent. Diagnoses were confirmed by using the Structured Clinical Interview for DSM-III-R
(7), and patients with current major depressive disorder, psychotic disorders, substance abuse/dependence in the past 6 months, or other major psychiatric disorder were excluded. Study participants were required to have had at least one panic attack per week during the 4 weeks before study entry.
Patients rated the frequency (sometimes, common, usually, or always) and severity (mild, moderate, or severe) of each DSM-III-R symptom during typical panic attacks. A semistructured interview, the Brief Physical and Sexual Abuse Questionnaire, was used to assess for the presence (score=1) or absence (score=0) of a history of traumatic events before age 16 in seven categories: 1) traumatic separation from the primary caregiver for more than 1 month, 2) substance-abusing family member in the home, 3) experience of harsh punishment (hitting with object), 4) physical injury to patient or sibling resulting from harsh punishment, 5) witnessing physical violence between caregivers, 6) forced sexual contact with an older child or adult (nonrelative), and 7) forced sexual contact with a relative (maximum score=7).
Patients who indicated that during panic attacks they commonly, usually, or always experienced depersonalization/derealization of moderate severity or greater were classified as dissociating patients (N=34) and were compared with the remainder of the group (N=40) on rates of childhood traumatic events and cumulative trauma exposure. Comparisons were made using the chi-square test. The severity of depersonalization/derealization during panic attacks in patients with more than two different types of childhood traumatic events and in patients with more than three different types of childhood traumatic events, respectively, were compared with the severity of those symptoms in the remainder of the group. Dissociating patients and nondissociating patients were also compared with respect to severity of illness on the following measures: 1) number of weekly panic attacks, 2) Hamilton Rating Scale for Anxiety
(8) score, 3) Hamilton Rating Scale for Depression
(9) score, and 4) SCL-90-R
(10) subscale scores.
RESULTS
The study group consisted of 27 men and 47 women with a mean age of 36.4 years (SD=10.0); 27 were Hispanic, six were African American, 34 were Caucasian, and seven had other ethnicities. Most patients (N=64; 87%) met the criteria for agoraphobia. Other comorbidity was as follows: past major depressive disorder, 22% (N=16); and social phobia, 9% (N=7). Average chronicity of panic disorder was 35 months (range=3–60 months). Dissociating patients and nondissociating patients did not differ significantly in the presence of agoraphobia or in gender, ethnicity, level of education, or marital status. Dissociating patients were significantly younger than nondissociating patients (33.8 versus 38.6 years) (t=2.11, df=72, p=0.04).
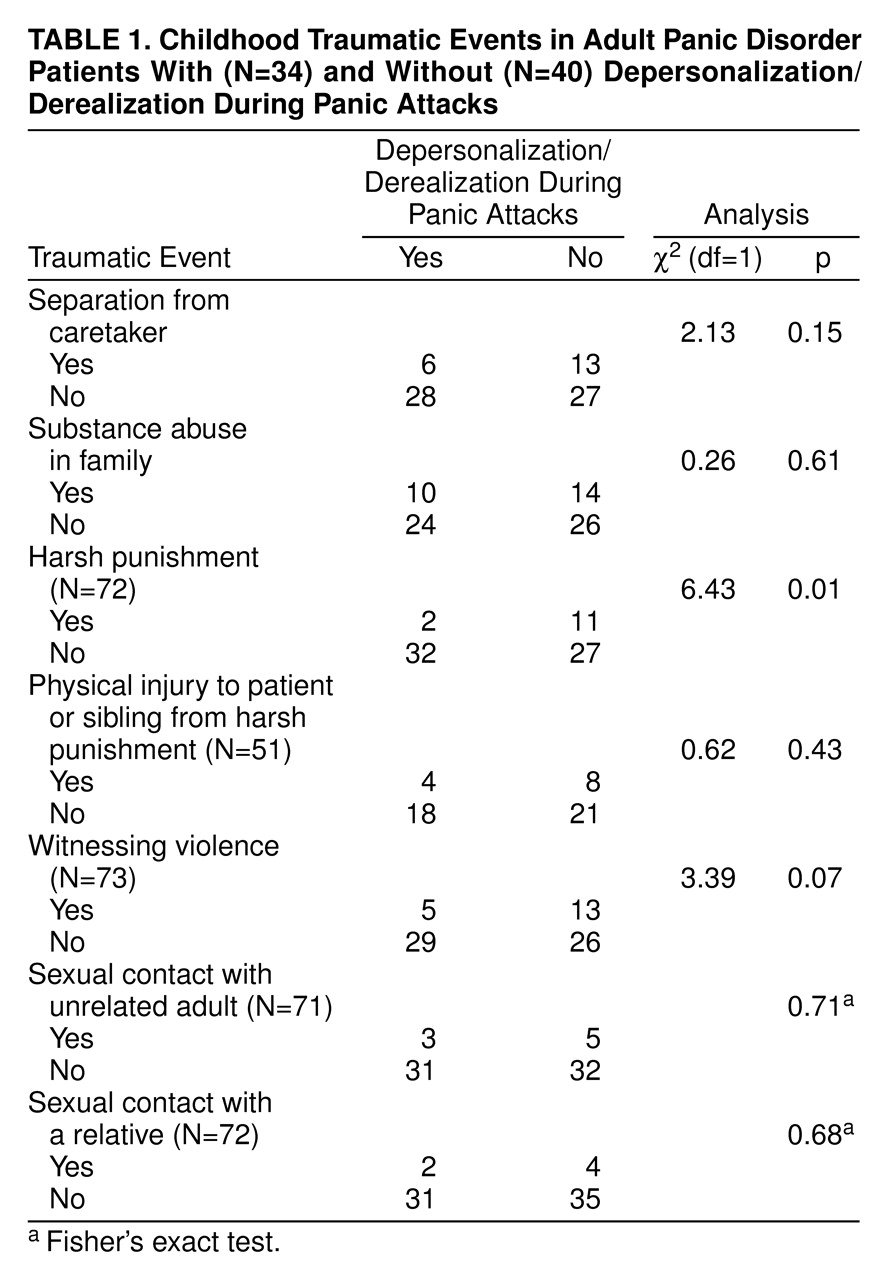
Patients with depersonalization/derealization during panic attacks did not report significantly more childhood trauma events than patients without such symptoms (
table 1). In fact, the only significant finding was in the opposite direction: patients who reported having been punished with an object that produced bruises or bleeding were significantly less likely to experience depersonalization/derealization during panic attacks than patients who had not been harshly punished (
table 1). This result may be a chance finding due to multiple comparisons. Similar results were found in the two analyses when the group was divided into groups with high and low levels of trauma. Patients with high levels of trauma—those who reported more than two or three different childhood traumatic events—were less likely to report depersonalization/derealization during panic than the remainder of the group (χ
2=4.33, df=1, p=0.04, N=74, and χ
2=6.86, df=1, p=0.009, N=74, respectively). Findings also did not differ when only those with severe depersonalization/derealization were compared to those without such symptoms.
Regarding severity of illness, dissociating patients reported significantly more situational panic attacks than nondissociating patients (two versus one per week) (t=2.0, df=54, p=0.05, N=74, unequal variances test) and scored significantly higher on the SCL-90 somatization subscale (20.4 versus 15.2) (t=2.41, df=69, p=0.02, N=71). No other differences between groups were found on symptom measures.
DISCUSSION
Contrary to our hypothesis, we found no evidence that a history of childhood traumatic experiences increased the likelihood of experiencing dissociative symptoms during a panic attack. Depersonalization/derealization during panic was also only minimally associated with greater symptom severity. This group size provides estimated power of 73% to detect a medium effect size (0.30) at p=0.05, and there was no evidence of a trend in the predicted direction.
Limitations of the study include use of a convenience group of treatment-seeking individuals and retrospective assessment of childhood traumatic events. The semistructured interview we used currently lacks validating data, but it assesses traumatic events whose links to adult psychopathology have been widely studied. Rates of childhood trauma in the study group were in the low-to-moderate range for clinical samples, which may be due in part to the exclusion of significant comorbidity. As the study did not include a general measure of dissociation, such as the Dissociative Experiences Scale, we could not rule out the possibility that depersonalization/derealization during panic was associated with increased trait dissociation. This issue can be addressed in replication studies.
Our findings do not agree with those of a previous study showing greater levels of disability, symptom severity, and agoraphobia in panic patients with depersonalization/derealization
(11). However, that study included individuals with major comorbid depressive and anxiety disorders, which might increase both dissociation symptoms and disability. An advantage of our study is that childhood trauma findings were not confounded by the presence of significant current comorbid disorders. Our findings suggest that depersonalization/derealization during panic per se is not a marker for a history of significant childhood trauma.
The treatment implications for depersonalization/derealization during panic are unknown and should be examined in clinical trials. In posttraumatic stress disorder, dissociative symptoms may improve with treatment of the primary disorder
(12).
Our findings, if replicated, are consistent with a multifactorial model of dissociation
(13). For example, it is possible that trauma-related dissociative symptoms are distinct from depersonalization/derealization during panic. A large epidemiologic study found that general psychopathology and childhood trauma contributed independently to increase risk for dissociative symptoms
(3). The study reported here suggests the existence of additional, unidentified factors other than general psychopathology and childhood trauma that mediate dissociative symptoms during panic. Further study of dissociating and nondissociating patients with panic disorder might contribute to our understanding of the neurobiological and psychological variables that influence depersonalization and derealization.