Schizophrenia has a long-term course characterized by exacerbations and remissions of psychotic symptoms and a relative persistence of negative symptoms
(1–
3). Perhaps because negative symptoms are associated with cognitive dysfunctions (e.g., alogia, attentional impairment, avolition), patients with schizophrenia continue to show ongoing psychosocial morbidity, including difficulty in returning to work or school. The persistence of psychosocial impairment and negative symptoms (under other names) has been observed since the original definition of the illness, leading Kraepelin to refer to it as a “dementia” and Bleuler to identify “thought disorder” (loosening of associations) as its core defining feature. More recent longitudinal studies of schizophrenia have suggested that cognitive deficits remain relatively stable over time, and that deterioration does not occur
(4–
7).
Achieving accurate definitions of the clinical course of cognitive and psychosocial impairments and the degree to which they do or do not progress is an important task in current schizophrenia research. Studies that examine the clinical course of schizophrenia raise important questions about underlying mechanisms of the disorder, such as the extent to which neural abnormalities are present and the degree to which they are static or progressive. In vivo imaging tools now permit us to examine such questions directly. Positron emission tomography (PET) permits us to examine whether functional abnormalities in the brain are associated with chronicity, in that it offers an opportunity to visualize and measure blood flow in vivo.
In a previous PET study
(8), we found abnormalities in widely distributed brain regions in a group of neuroleptic-naive patients experiencing their first episode of schizophrenia. It is still unclear whether neuronal abnormalities observed by using PET during the early stage of illness are also present during later stages, or whether the pattern of abnormalities changes after patients have been chronically ill. If abnormalities occur, these could reflect either the long-term effects of medications, the toxic effects of persistent or recurrent psychotic symptoms, or an underlying progressive morbid process. If abnormalities do not occur, this suggests that the mechanisms of the illness are nonprogressive and do not resemble a dementia-like process.
The present report is a follow-up to our previous study. Here we examine a group of patients who were chronically ill but who were studied with PET when neuroleptic-free, thereby eliminating the potential confound of acute medication effects. In the present study, we compare the regional cerebral blood flow (rCBF) of neuroleptic-free patients with chronic schizophrenia and the rCBF of normal subjects during the resting state, as in our previous study of neuroleptic-naive first-episode patients. The aim of the current study was to examine the patterns of rCBF in chronic schizophrenia and determine if the patterns of flow abnormality in chronically ill patients are similar to those of first-episode patients. We hypothesized that we would find a similar pattern of abnormalities in distributed brain regions in the chronically ill patients, reflecting the relative stability of cognitive function that has been reported in recent papers
(6,
7).
In first-episode patients, we observed abnormalities in distributed anatomically connected regions, including the prefrontal cortex, cerebellum, and thalamus. Similar findings in chronically ill patients would be consistent with the hypothesis that schizophrenia is characterized by a fundamental group of neural abnormalities that remain relatively similar over the course of the illness, which are manifest as the fundamental and persistent abnormalities in cognitive function originally described by Bleuler. In earlier work
(9–
11), we described these fundamental neural abnormalities as involving cortical-cerebellar-thalamic-cerebellar circuitry and the associated cognitive abnormalities as “cognitive dysmetria.”
METHOD
Subjects
We examined 30 patients diagnosed as having schizophrenia according to DSM-IV who had been chronically ill. Twenty-five were men, and five were women. Their mean age was 33.0 years (SD=10.3), and their mean educational level was 13.1 years (SD=2.2). The mean educational level of their fathers was 12.9 years (SD=3.8). Twenty-six were right-handed, two were left-handed, and two were ambidextrous. Their mean duration of illness was 10.2 years (SD=9.4). They had been neuroleptic-free for a minimum of 3 weeks before PET scan.
Severity of symptoms was measured just before the PET study with the Scale for the Assessment of Negative Symptoms
(12) and the Scale for the Assessment of Positive Symptoms
(13). These scales were used to construct measurements of three dimensions of symptoms that could be used to examine correlations between symptom severity and patterns of blood flow as measured by PET: psychoticism, disorganization, and negative symptoms. The patients’ mean global scores for the psychoticism dimension (i.e., hallucinations and delusions) and the negative symptoms dimension (i.e., affective flattening, anhedonia, alogia, and avolition) were 2.7 (SD=1.6) and 2.4 (SD=1.1), respectively, which would be in the mild to moderate range. Their mean global score for the disorganization dimension (i.e., positive formal thought disorder and bizarre behavior) was 1.2 (SD=1.4), which would be in the questionable to mild range. Individual summed scores were calculated for each subject for each dimension to be used in the PET correlational analyses.
Extrapyramidal side effects of medications were assessed with the Simpson-Angus Rating Scale
(14) and the Abnormal Involuntary Movement Scale
(15). The patients’ mean total scores on those scales were 2.5 (SD=4.2) and 1.3 (SD=1.8), respectively.
Thirty normal comparison subjects (25 men and five women) were recruited from the community through a newspaper advertisement. Their mean age was 30.1 years (SD=9.5), and they were all right-handed. Their mean educational level was 14.5 years (SD=2.2), and the mean educational level of their fathers was 12.7 years (SD=3.1).
All patients and comparison subjects gave written informed consent to a protocol approved by the Human Subjects Institutional Review Board of the University of Iowa.
Imaging Data Acquisition
All subjects were studied during a resting state, lying quietly with eyes closed and having received no specific instructions about mental activity. We have previously characterized this cognitive condition as “random episodic silent thinking”
(16) because it consists of unfocused and uncensored thinking about past recollections, future plans, or other personal thoughts. In a second and more intensive experimental study of the resting state, we confirmed the nature of this “random episodic silent thought” through extensive debriefing interviews done immediately after PET data acquisition
(17).
All subjects had either an initial sham (no tracer injected) or scout (15 mCi of tracer) scan to reduce their anxiety; during these scans all procedures were identical to an image acquisition condition except that no arterial blood was sampled. The PET data were acquired after patients had been given an intravenous bolus injection of 50–75 mCi of [15O]H2O in 5–7 ml of saline. A GE 4096-plus 15-slice whole-body scanner was used. Arterial blood sampling, needed for calculation of tissue perfusion, and imaging (ten 10-second or twenty 5-second frames) began at the time of tracer injection and continued for 100 seconds.
On the basis of time-activity curves, four 10-second or eight 5-second frames reflecting the 40 seconds immediately after the bolus transit were summed
(18). The summed image was reconstructed into 2-mm voxels in a 128×128 matrix by using a Butterworth filter (order=6, cutoff frequency=0.35 Nyquist interval). Using the blood curve and an assumed brain partition coefficient of 0.9, we calculated rCBF on a voxel-by-voxel basis according to the autoradiographic method
(19).
Images were analyzed by the locally developed software package Brain Research: Analysis of Images, Networks, and Systems
(20–
22). PET data were coregistered on a T
1-weighted magnetic resonance image. The coregistered images were resampled and simultaneously visualized in all three orthogonal planes. Since statistical analyses are particularly sensitive to registration errors, we applied a standard automated registration check for all scans; if registration was found to be inaccurate on the basis of a predefined conservative level, the registration was redone. In addition, registration was visually checked for each case and repeated if errors were observed.
A nonparametric randomization test was used to determine between-group differences—the random episodic silent thinking condition in comparison subjects was subtracted from the random episodic silent thinking condition in patients. The test is a nonparametric technique that makes no assumptions about variance and is not affected by between-group differences in variance. Each t value in the image is compared with a large number of randomly generated t values generated from random rearrangements of the data. The p value is empirically found from this randomly generated distribution. It is particularly appropriate for complex between-group comparisons in PET studies
(23,
24).
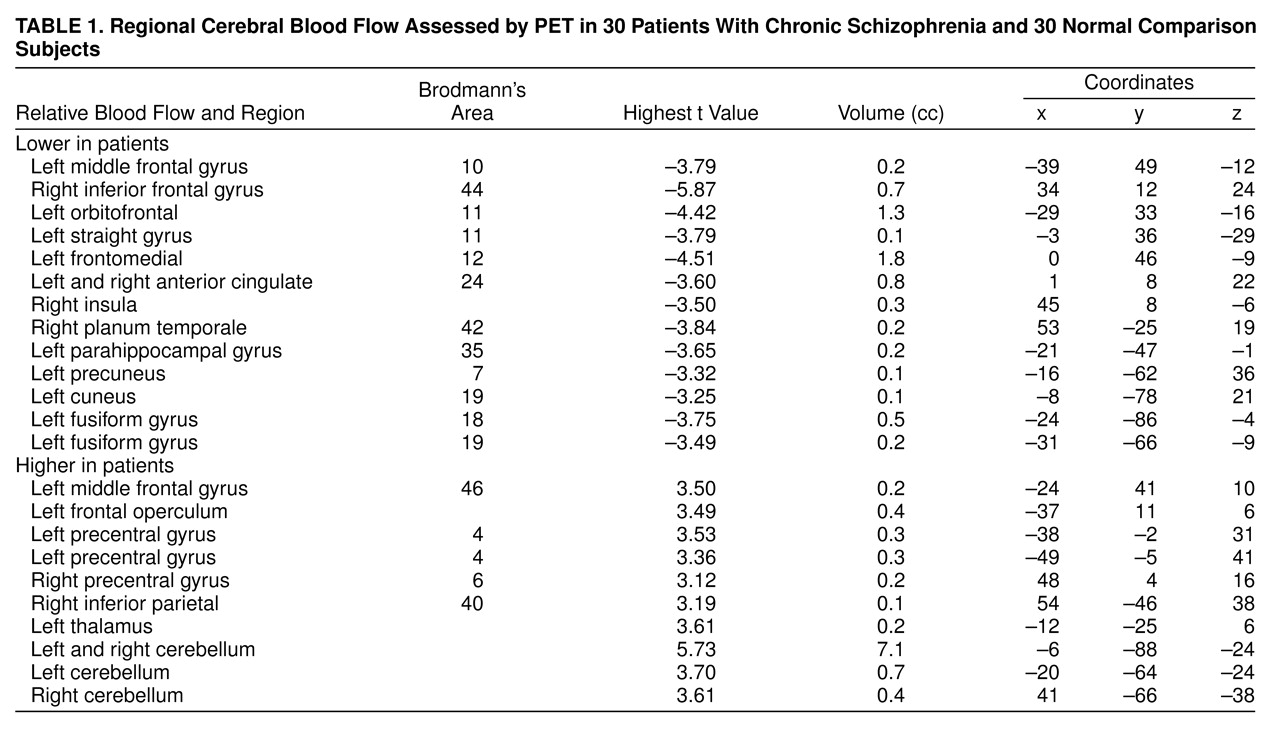
Areas showing significant regional differences were identified as “peaks,” which were expressed as the highest t value, the volume of the peak, and the standard atlas coordinates
(25). The peaks reported in
table 1 contained at least 60 contiguous voxels exceeding a t threshold of 3.61. Anatomical localization was based not only on direct visual inspection of coregistered magnetic resonance and PET images but also on the atlas. Regional differences associated with a negative t value indicate that flow was lower in patients than in comparison subjects, whereas those with a positive t value indicate that flow was higher in patients than in comparison subjects.
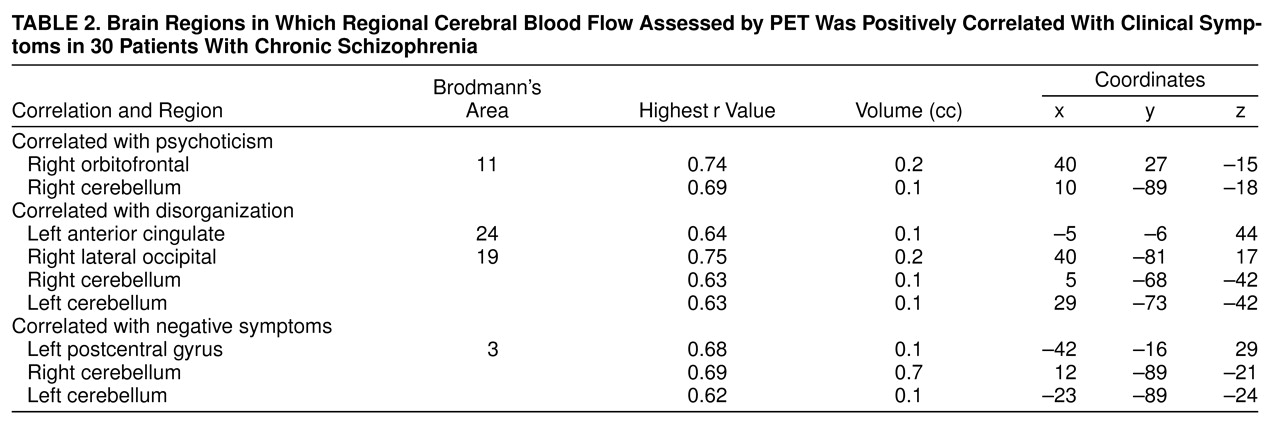
In addition, a correlation analysis was performed to clarify the relationship between rCBF and the three symptom dimensions. Resolution was reduced from a voxel size of 1.08×1.35×1.48 mm to 3.0×2.7×2.0 mm to decrease the time required to compute the large number of correlations. A Pearson correlation coefficient between blood flow within each voxel and symptom severity for each of the three dimensions was calculated. A threshold was then applied so that only regions with a correlation coefficient above 0.60 (p<0.005) and a size criterion of at least 40 contiguous voxels were selected. Each peak produced in this analysis was reported as the highest r value, its volume, and the atlas coordinates (
table 2). This is a stringent and conservative level for detecting correlations, which reduces the risk for type I errors, although it may have a higher risk for type II errors.
RESULTS
Significant areas found in the randomization analysis comparing the neuroleptic-free patients with chronic schizophrenia and the healthy volunteers are shown in
table 1. The results comparing the drug-naive first-episode patients with normal subjects in the same condition have been reported previously
(8). As
table 1 indicates, the chronically ill patients differed from the healthy volunteers in multiple regions. These differences involve both areas of lower flow and areas of higher flow.
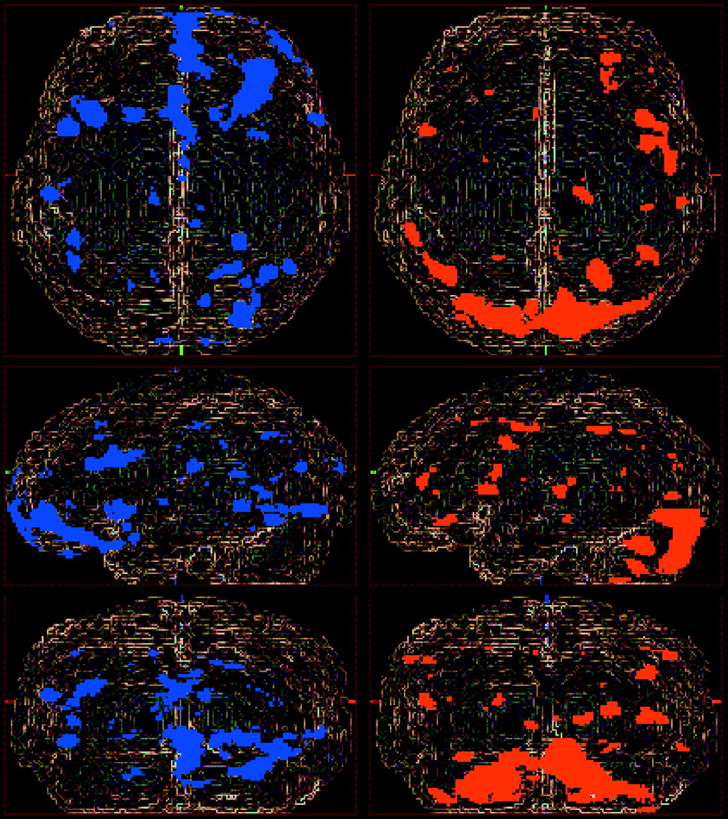
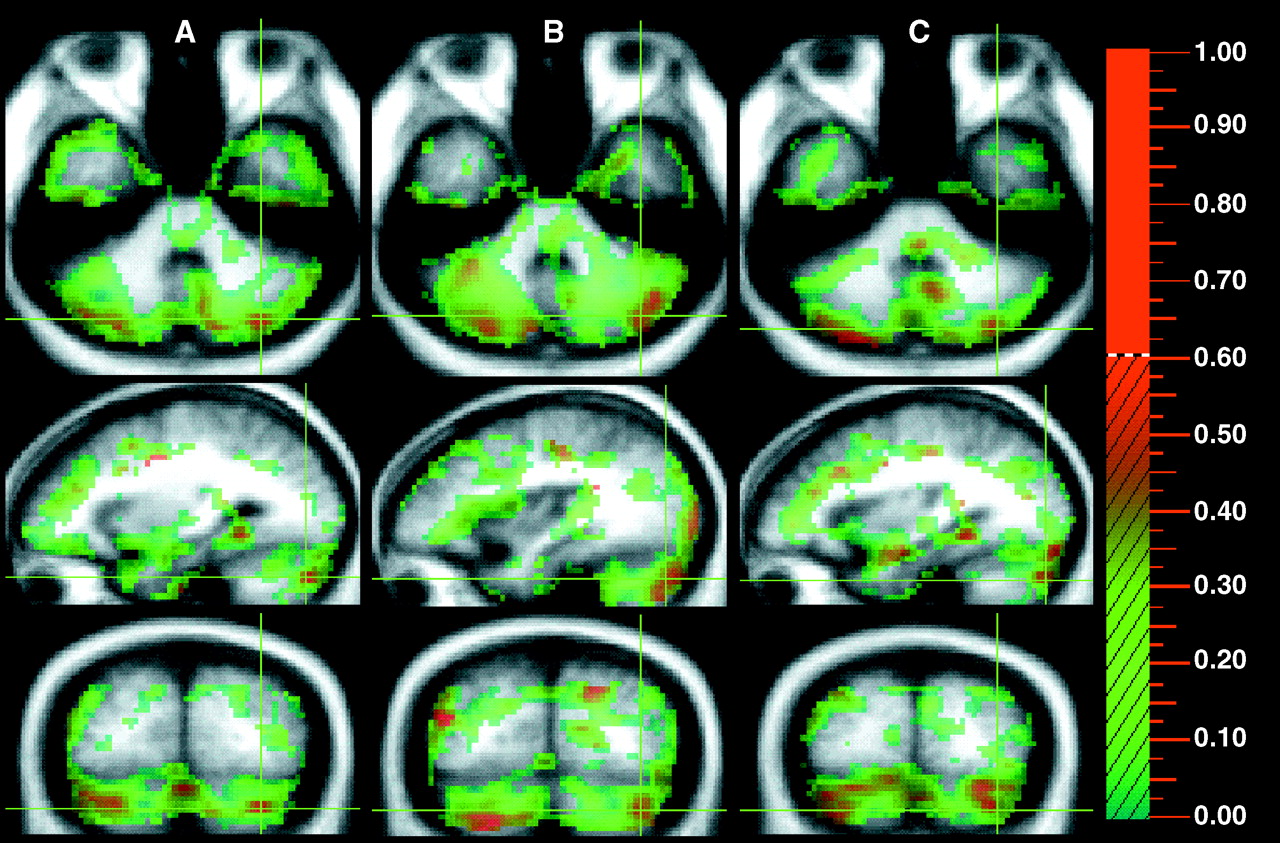
As observed previously in the first-episode patients, the chronically ill patients manifested “hypofrontality”: lower blood flow in extensive prefrontal regions, including lateral (Brodmann’s areas 10 and 44), ventral (Brodmann’s area 11), and medial (Brodmann’s areas 12 and 24) cortexes (frontal areas of
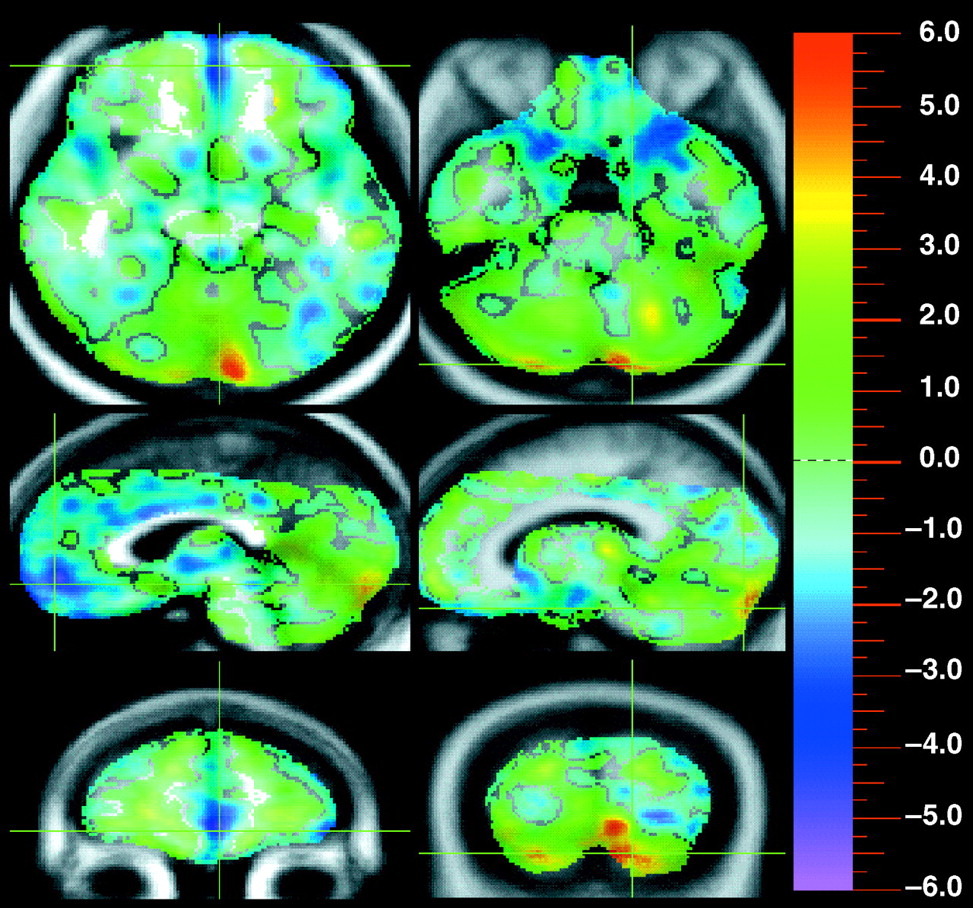
figure 1). Specifically, the left side of
figure 2 shows that medial and orbital prefrontal area was inactive in the chronically ill patients. In addition, a few small areas in the temporal and parietal lobe, primarily involving medial or deep cortices, had decreased flow. Furthermore, the left visual cortex (Brodmann’s areas 18 and 19) appeared to form a cluster of inactivity. However, visual inspection of
figure 1 indicates that these regions are relatively small, in comparison with the extensive areas of decreased flow in frontal regions.
Areas were also observed in which the chronically ill patients had higher flow than the healthy volunteers. The most prominent increase was shown in both sides of the cerebellum in the chronically ill patients (large peak in the right side of
figure 2).
Figure 1 shows the cerebellar hyperperfusion compared with the prefrontal hypoperfusion. In addition, the thalamus also displayed increased blood flow (sagittal view of the right side of
figure 2). Like the frontal decreases, these areas of increased flow are similar to those previously observed in first-episode patients. Additionally, other small areas of increased flow were observed, which include parts of the dorsolateral prefrontal area (Brodmann’s area 46), motor and premotor area (Brodmann’s areas 4 and 6), and inferior parietal area (Brodmann’s area 40).
The analysis examining the correlations between each of the three symptom dimensions and rCBF is shown in
table 2. These correlations indicate those regions in which higher flow was associated with greater severity of symptoms. As this table indicates, only one brain region—the cerebellum—displayed increased flow for all symptom dimensions. Extensive high correlations were observed both in the cerebellar vermis and in the lateral cerebellum (
figure 3). Increases in the vermis were correlated with severe psychoticism (coordinates 10, –89, 18), negative symptoms (coordinates 12, –89, –21), and disorganization (coordinates 5, –68, –42). Apart from the generalized cerebellar correlations, specific correlations were also seen with specific dimensions: the orbitofrontal cortex with psychoticism, anterior cingulate with disorganization, and postcentral gyrus with negative symptoms.
DISCUSSION
The major finding in this study is that neuroleptic-free patients with chronic schizophrenia showed lower blood flow in prefrontal areas and higher flow in thalamic and cerebellar regions than normal comparison subjects. The overall pattern of decreased blood flow in most of the prefrontal areas (
figure 1) is consistent with findings from the majority of previous studies reporting “hypofrontality”
(26–
28). Resting hypofrontality has also been demonstrated in neuroleptic-naive first-episode patients by our group
(8) and by others
(29). Since a similar hypofrontality is present in both first-episode and chronically ill patients, these findings suggest that this regional dysfunction reflects an abnormality that is present at onset and persists with chronicity. The similarity between first-episode and chronically ill patients also suggests that prefrontal dysfunction is not due to the chronicity of illness or long-term neuroleptic treatment.
Dysfunction in the prefrontal cortex has been proposed to contribute to the pathophysiology of schizophrenia because the area receives a dense dopaminergic innervation forming the mesocortical dopamine system
(30). This persisting neural dysfunction in the prefrontal area may account for enduring cognitive deficits in schizophrenia regardless of its stage. Hypofrontality has been associated with impairment in executive functions, including anticipation, goal establishment, planning, response trials, monitoring of results, and use of feedback
(31–
33).
Nonetheless, patterns of prefrontal blood flow in the current study challenge a simplistic view of hypofrontality for several reasons. In addition to decreases in flow, we also observed increases in some regions, such as the dorsolateral area. This simultaneous existence of hyper- and hypofunctioning regions may account at least in part for the inconsistent findings of previous functional imaging studies regarding hypofrontality, since abnormalities may vary depending on how the regions of interest are defined. These findings suggest, therefore, that the concept of “global hypofrontality” should be revised and that the differences in subregions should be taken into account. Second, hypofrontality in this study is not confined to the dorsolateral area but is also found in the orbital area and in the medial area, including the anterior cingulate. These three aspects of the frontal lobe are involved in different cognitive functions and have different neural connections with other regions
(34), suggesting that primary impairment may exist in other integrating regions with reciprocal connections to all these frontal regions.
In addition to areas in the prefrontal cortex with decreased flow, we also observed increases in several regions. Particularly noteworthy are the increases in the thalamus and the cerebellum, since they were also observed in the first-episode patients. As in the case of the frontal dysfunctions, these results suggest a continuity of abnormalities that are present at onset of schizophrenia and persist as the illness becomes more chronic. This group of consistent and persistent regional abnormalities may define those regions which are fundamental or basic in the disorder.
These three regions have been shown to have anatomical interconnections that regulate many aspects of motor and mental activity
(10,
35–
37). Therefore, an abnormality in one region of a reciprocal neural loop may produce compensatory changes in other interconnected regions, altering the functional relationships and forming a complex pathological cascade. The thalamus has been thought to serve as a filter of sensory information, to relay information between the cerebellum and cortical regions, and to modulate motor and cognitive coordination
(10,
35,
37,
38). The cerebellum plays a critical role in coordinating complex mental and language skills as well as motor skills
(36). This has been supported by numerous functional imaging studies demonstrating increased blood flow in the cerebellum during a wide range of cognitive tasks
(39–
45). The areas of increased flow in the cerebellum and thalamus may indicate that these brain regions are working harder to compensate for decreases in other regions. Thus, cerebellar and thalamic hyperfunction during the resting state may occur in order to compensate for hypofrontal function.
The results of the present study also suggest that cerebellar resting hyperfunction may be related to the psychopathology and clinical presentation of schizophrenia. That is, the correlational analyses suggest that increases in cerebellar flow are associated with increases in all three symptom dimensions, suggesting that the cerebellum may play a central role in producing the entire range of symptoms that occur in schizophrenia. These results highlight the possibility that abnormalities in the cerebellum, a “metron” that monitors the timing of mental and motor activities (i.e., helps to form accurate and appropriately matched connections between mental associations), could account for the broad range of psychopathology in schizophrenia. These findings provide an anatomical explanation for Bleuler’s conceptualization of “loosening of associations.” We have suggested previously
(46) that a more modern formulation of this idea could be called “cognitive dysmetria,” or poor coordination of mental activities, which could be the basic cognitive abnormality that defines the phenotype of schizophrenia.
CONCLUSIONS
Whether progressive neural abnormality is associated with chronicity of schizophrenic illness is an important issue in contemporary schizophrenia research. Theoretically, long-term neuroleptic treatment or chronicity of illness itself can produce neurochemical changes at the molecular level, such as in second messenger systems or gene expression, and force the patterns of distribution of rCBF to be different from those at the early stage of illness. The findings of this study revealed, however, that abnormal patterns of blood flow in chronically ill patients are quite similar to those in first-episode patients; rCBF is decreased in the frontal lobe and increased in the thalamus and the cerebellum in both first-episode and chronic schizophrenia. All these areas are major nodes in a distributed circuit that modulates motor and mental activity, which we have referred to as the cortico-cerebellar-thalamic-cortical circuit. These results suggest that an imbalance in functional relationships between cortical and subcortical regions (i.e., thalamus, cerebellum) occurs during the early stage of illness and persists during the chronic period. This suggests that abnormalities in these regions may represent the fundamental neural abnormality in schizophrenia and account for its persistent but nonprogressive cognitive abnormalities.