Clinical depression has a substantial impact on coronary heart disease events
(1). One possible mediator of this relationship is platelet activation, an important factor in coronary heart disease
(2). Previous studies have found increased platelet activation in depressed patients
(3,
4). The present study sought to determine whether sertraline diminishes platelet activation among depressed patients. We also assessed aspects of platelet serotonergic function to determine whether decreases in platelet activation are associated with changes in these measures.
Method
We tested 21 depressed patients who were 25–52 years old and 21 sex- and age-matched (within 3 years) comparison subjects. Depressed patients were otherwise healthy and had not taken medications affecting platelet activation for at least 14 days before testing. Subjects with substantial medical or other psychiatric disease were excluded. Individuals who had taken antidepressants or anxiolytics previously had been drug-free for at least 4 months. There was one smoker (sex- and age-matched) in each group. Subjects were recruited through local advertisements. The study was approved by the institutional review board of the University of Alabama at Birmingham. After complete description of the study to the subjects, written informed consent was obtained.
Depressed subjects were screened over the phone by interviewers using the 21-item Hamilton Depression Rating Scale; individuals with a Hamilton depression scale score of 20 or higher were then interviewed in an office visit with the Primary Care Evaluation of Mental Disorders (PRIME-MD) and the Beck Depression Inventory. Subjects with a Beck Depression Inventory score of 10 or higher and a diagnosis of major depressive episode according to the PRIME-MD were evaluated by a psychiatrist (J.L.S.) using a repeat Hamilton depression scale and clinical evaluation. These subjects then entered into the study.
Nondepressed comparison subjects were screened by using the PRIME-MD and Beck Depression Inventory; lack of depression was determined by a lack of depressive symptoms and anhedonia and a Beck Depression Inventory score less than 10.
All subjects were tested as described elsewhere
(5,
6). Nondepressed subjects were tested only once.
Depressed patients began taking 50 mg/day of sertraline after blood testing and were evaluated at 3 weeks; 11 of the 17 patients who returned for the second evaluation had their dose increased to 100 mg/day (one patient started on 25 mg and increased to 50 mg at 3 weeks). After 6 weeks, 17 patients returned for repeat laboratory and Beck Depression Inventory testing.
Platelet activation measures were performed as described elsewhere
(5,
6). Three markers for activation detection were used: AC1.2-PE for platelet secretion; anti-LIBS-1, specific for fibrinogen receptor binding; and annexin V, a marker of membrane procoagulant activity
(3).
Procedures for platelet serotonin receptor measures have been described elsewhere
(5). Studies were accomplished in triplicate by using [
3H]LSD, creating saturation curves from concentrations ranging from 0.2 nM to 1.7 nM to determine receptor density (B
max) and apparent affinity (K
d).
Fifty milliliters of platelet-rich plasma was added to 950 μl of perchloric acid (0.2 mol/liter), vortexed, and stored at –70˚C. Analysis for platelet serotonin content, determined by high performance liquid chromatography, was performed by Dr. Michael Owens at Emory University.
For both groups, a family history of coronary heart disease was defined as a parent or grandparent with a coronary heart disease event or stroke before the age of 65.
Results
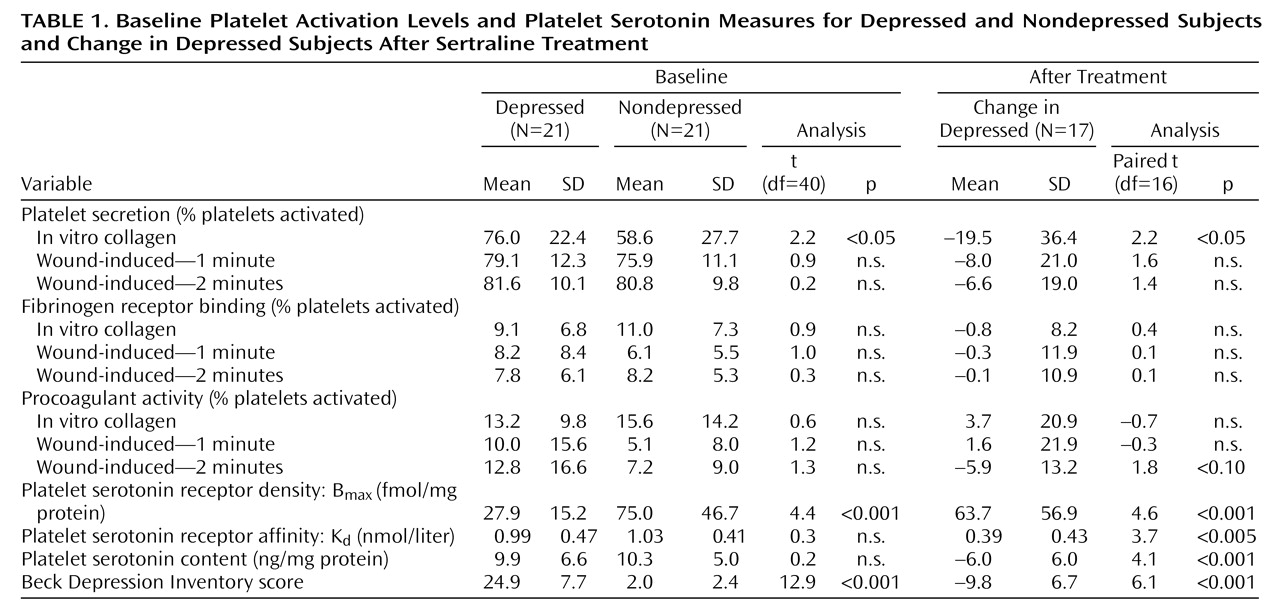
There were 11 women and 10 men in each group and one black woman in each group. Eleven of the depressed patients had a family history of coronary heart disease, compared with seven of the comparison subjects. Platelet secretion in response to collagen was higher among depressed patients (
Table 1). In contrast, B
max was lower in depressed patients than in comparison subjects. Individuals with both depression and a family history of coronary heart disease had nonsignificantly higher wound-induced fibrinogen receptor binding at 1 minute (mean=10.6, SD=9.9) than the other subjects (mean=5.9, SD=5.4) (t=1.97, df=40, p=0.06).
After sertraline treatment, collagen-induced platelet secretion decreased (
Table 1). Most other platelet activation measures showed minimal change, although wound-induced procoagulant activity at 2 minutes was nonsignificantly decreased (t=1.8, df=16, p=0.09). Regression analyses indicated that changes in platelet activation were not related to B
max or platelet serotonin content, final sertraline dose, changes in Beck Depression Inventory scores, or a Beck Depression Inventory follow-up score of less than 10.
Discussion
The present study provides initial evidence that sertraline treatment decreases platelet activation. Collagen-induced platelet secretion was higher among depressed patients than comparison subjects and also decreased after sertraline treatment. The specific findings regarding platelet secretion are highly consistent with previous findings showing increased secretion among depressed patients
(3,
4) and diminished secretion with selective serotonin reuptake inhibitor (SSRI) treatment
(7). Our study also indicates that depressed patients with a family history of coronary heart disease may have increased fibrinogen receptor binding, although the findings were not statistically significant due to the small number of subjects. The fibrinogen receptor is the final common pathway of platelet aggregation
(2), and our previous studies have demonstrated its importance
(5,
6).
We postulated that the sertraline-associated decrease in platelet activation would be mediated through platelet serotonergic mechanisms; however, although sertraline did substantially alter platelet serotonin content and Bmax, these changes were not associated with change in platelet activation. Decreases in platelet activation were also not related to improvement in Beck Depression Inventory scores, but this finding may be limited by the relatively short treatment duration of 6 weeks.
Contrary to expectations and the findings of other studies
(8,
9), serotonin 2A receptor density was higher among nondepressed subjects. One explanation for this discrepancy is that the relationship between receptor density and depression may be confounded by smoking status. In our previous study
(6), receptor density was greater in smokers than in nonsmokers, and this difference was not related to depressive symptoms. The present study had only one smoker in each group. Although previous studies
(8,
9) did not report whether patients were smokers or not, given the high rates of depression among smokers
(10), it is possible that many subjects in these studies were smokers.
In summary, sertraline diminishes the increased platelet secretion found among depressed patients. Sertraline and other SSRIs may diminish the risk of coronary heart disease among depressed patients by decreasing platelet activation. Future studies would benefit from a placebo-controlled design, a larger number of subjects to explore interactions between family history of coronary heart disease and depression, and a longer follow-up period.