Magnetic resonance imaging (MRI) studies have identified many brain regions affected in schizophrenia
(1). The thalamus has been a focus of interest
(2) because of its role as a sensory filter and reports of schizophrenia as a disorder of deficient information filtering
(3). Andreasen
(2) proposed a model of schizophrenia placing the thalamus in the center of dysfunctional cortical-subcortical-cerebellar circuitry.
MRI studies of the thalamus in schizophrenia have not conclusively demonstrated abnormalities. Although some
(4–
8) have reported reduced volumes, others
(9–
11) have found no significant reductions. Postmortem studies
(12,
13) have reported reductions in the volume and number of neurons in the mediodorsal thalamus.
Most MRI studies of the thalamus have studied chronically ill patients, and one study found an association between antipsychotic medication dose and thalamic volumes
(7). Thus, little is known about thalamic abnormalities in the early stages of psychosis, when the possible confounding effects of disease chronicity and long-term medication exposure do not apply.
In this study we investigated thalamic volumes in a group of patients who were experiencing their first psychotic episode and who had no or minimal exposure to antipsychotic medication. Our hypothesis was that patients would have smaller thalamic volumes than nonpsychotic comparison subjects.
Method
Cerebral scans of 29 healthy volunteers (mean age=25.4 years, SD=5.8) and 38 patients (mean age=24.2 years, SD=5.4) with a DSM-IV diagnosis of schizophrenia, schizophreniform disorder, or schizoaffective disorder (according to the Structured Clinical Interview for DSM-IV Axis I Disorders, Patient Edition
[14]) were obtained with MRI. Twenty-eight of the patients were men, and 20 of the comparison subjects were men. The groups were matched in age (t=–0.87, df=65, p=0.39) and height (t=–0.49, df=65, p=0.63).
The mean duration of the patients’ illness was 30.8 weeks (SD=24.9). Thirteen patients had never taken an antipsychotic, 18 were treated with typical antipsychotics, and seven were treated with atypical antipsychotics. The mean duration of treatment for medicated patients was 4.6 weeks (SD=3.0). Research psychiatrists (D.G.F., S.O’C., V.C.D.) rated symptoms using the Positive and Negative Syndrome Scale
(15) within 5 days of MRI scanning. Inter- and intrarater reliability (over a period of 1 year), obtained from videotaped patient interviews, was above r=0.90.
Patients were recruited as inpatients or outpatients from a catchment area including inner and outer London. Comparison subjects were recruited from the same area; these volunteers had no history of mental disorder themselves or of psychosis among first-degree relatives. Scanning of patients and comparison subjects was interleaved.
All participants provided written informed consent. The study was approved by the Ethics Committee of the Bethlem and Maudsley National Health Service Trust.
Brains were scanned with a 1.5-tesla GE Signa Advantage MRI scanner (Milwaukee). Three-dimensional T1-weighted spoiled gradient recalled scans were acquired in the axial plane with the following sequence: TE=2.2 msec, TI=300 msec, TR=11.3 msec, field of view=22 cm, flip angle=20°>, number of excitations=1, producing 124 1.5-mm slices. A phantom was scanned biweekly for quality control.
Thalamic boundaries were based on detailed guidelines described elsewhere
(11). Volumetric measurements were obtained by using stereological assessment software (MEASURE
[16]). Thalamic ratings were performed by one researcher (U.E.) who was blind to diagnostic status. Inter- and intrarater reliabilities (over a period of 1 month), computed in a random sample of 10 brains, were r=0.82 (p<0.001) and r=0.99 (p<0.001), respectively.
Total thalamic volume was analyzed by one-way analysis of covariance (ANCOVA) with height as the covariate. Repeated measures ANCOVAs were performed, with side (left or right) as within-subject factors and group (patients or comparison subjects) as between-subject factors covarying for height. Further ANCOVAs covarying for height were performed to investigate sex differences and to examine medication status, comparing patients receiving atypical antipsychotics, those receiving typical antipsychotics, and untreated patients. Height was used as a covariate because it has been shown to predict brain size and has been used in previous MRI studies of schizophrenia
(17). Pearson correlations explored associations between thalamic volumes and Positive and Negative Syndrome Scale subscores, duration of treatment (in weeks), and duration of illness (in weeks).
Results
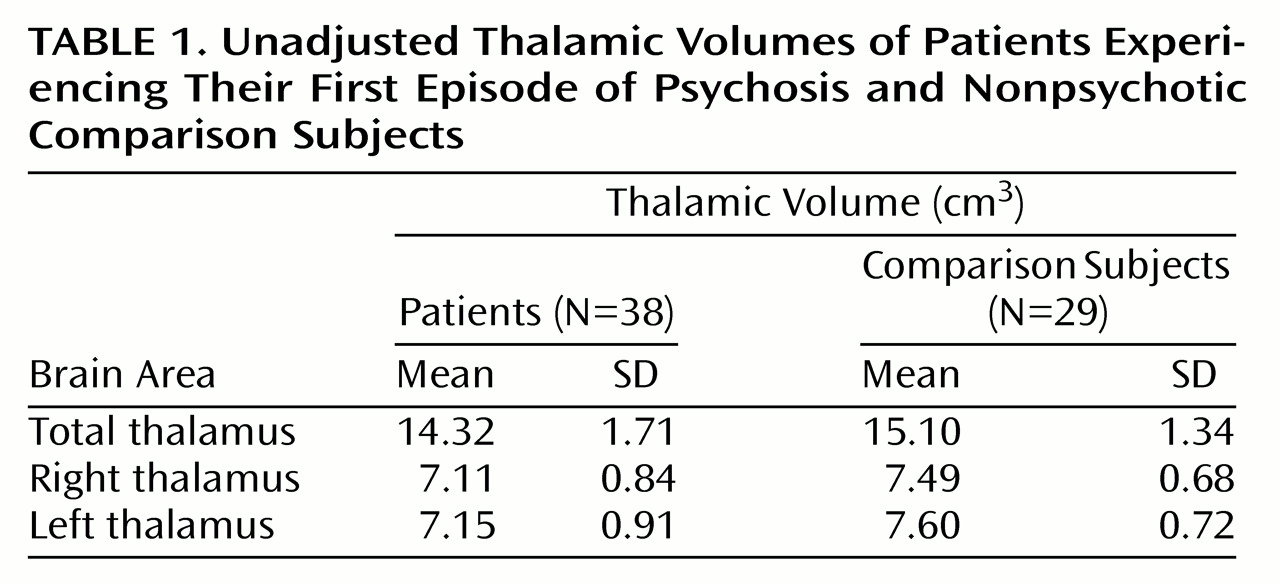
Patients had smaller total thalamic volumes than comparison subjects (F=3.87, df=1, 64, p=0.05). There was no effect of side (F=1.09, df=1, 64, p=0.30) and no side-by-group interaction (F=0.47, df=1, 64, p=0.50). A significant effect of group, however, was found (F=4.34, df=1, 64, p=0.04), confirming the effect for total thalamus. Thalamic volumes (
Table 1) were similar to values reported previously for patients with schizophrenia
(11).
There was no effect of sex (F=1.59, df=1, 62, p=0.21) and no sex-by-group interaction (F=0.00, df=1, 62, p=0.98). In the comparison of patients receiving atypical antipsychotics, those receiving typical antipsychotics, and medication-naïve patients, no differences in thalamic volume were found (F=0.01, df=2, 34, p=0.99).
Thalamic volumes did not correlate significantly with the positive, negative, or global psychopathology scales or any of the subscales of the Positive and Negative Syndrome Scale (all p>0.11), duration of treatment (r=0.11, p=0.50), or duration of illness (r=0.01, p=0.96).
Discussion
The main finding of this study is that patients experiencing their first episode of psychosis had smaller thalamic volumes than nonpsychotic comparison subjects. This finding is consistent with structural
(2) and functional
(18) imaging evidence of thalamic abnormalities in schizophrenia.
No association between thalamic volumes and symptom scores was found, unlike previous reports of chronic schizophrenia
(6,
11), possibly reflecting the fluctuating nature of symptoms early in psychotic illness.
Because medication status and treatment duration did not affect thalamic volumes, the observed differences may represent early manifestations of the psychotic disease process, possibly reflecting a neurodevelopmental insult. The functional importance of thalamic volume reductions may lie in aberrant gating of information through cortical-subcortical circuits
(2,
3).
Given the structural and functional heterogeneity of the thalamus, abnormalities may be localized to specific nuclei. Future studies should investigate thalamic subregions such as the anterior or mediodorsal nuclei
(19), which have been found to be abnormal in schizophrenia
(10,
13).