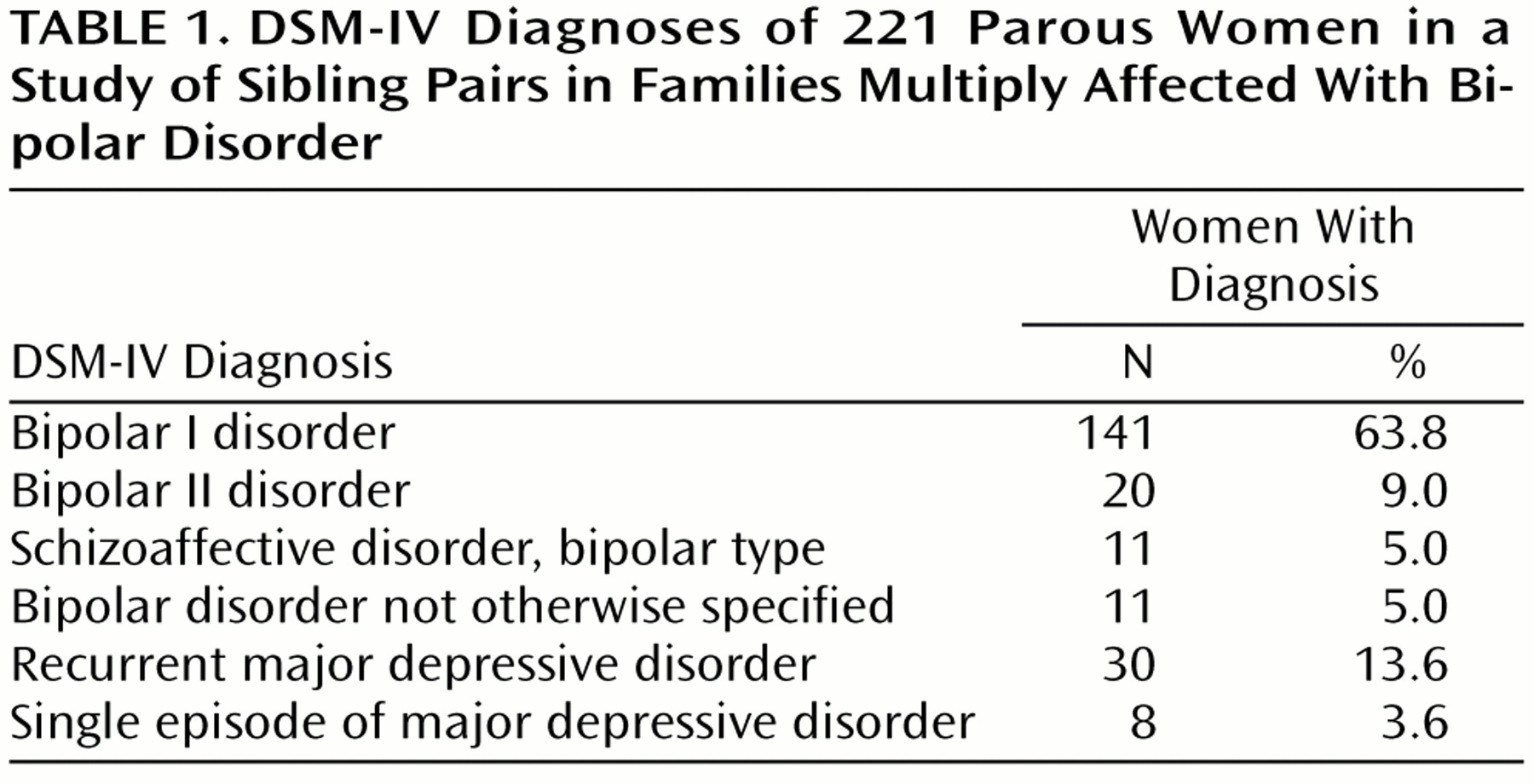
For the women with narrowly defined bipolar I disorder and schizoaffective disorder, bipolar type, the mean age at onset of affective illness was 28 years (median=25, SD=11), the mean number of manic episodes was 5.2 (median=4, SD=5.6), and the mean number of depressive episodes was 4.9 (median=4, SD=4.9). Eighty-five (56%) of these women had experienced psychotic symptoms at some stage during their illness.
Occurrence of Perinatal Episodes of Illness
Using the definition of puerperal psychosis already outlined, we found that episodes followed 81 (26%) of 313 deliveries to the 152 parous women in the narrow diagnostic group. Fifty-eight (38%) of the 152 women had experienced at least one episode of puerperal psychosis, 12 (8%) had experienced two episodes, and one (1%) had experienced three. A further 39 (26%) had suffered some other form of perinatal affective episode in pregnancy or within 6 months of delivery. This included four women with a hypomanic episode in the puerperium, 11 with an affective episode in pregnancy, five with a manic episode with onset after 6 weeks, and 19 with an episode of postnatal depression or anxiety. Fifty-five parous women in the narrow diagnostic group (36%) had not suffered any form of perinatal affective episode.
The average numbers of deliveries to women with bipolar disorder with a history of puerperal psychosis (mean=2.07, range=1–5) and deliveries to parous women with bipolar disorder who had no perinatal episodes (mean=2.15, range=1–6) were very similar and did not differ significantly.
Familial Clustering of Puerperal Episodes
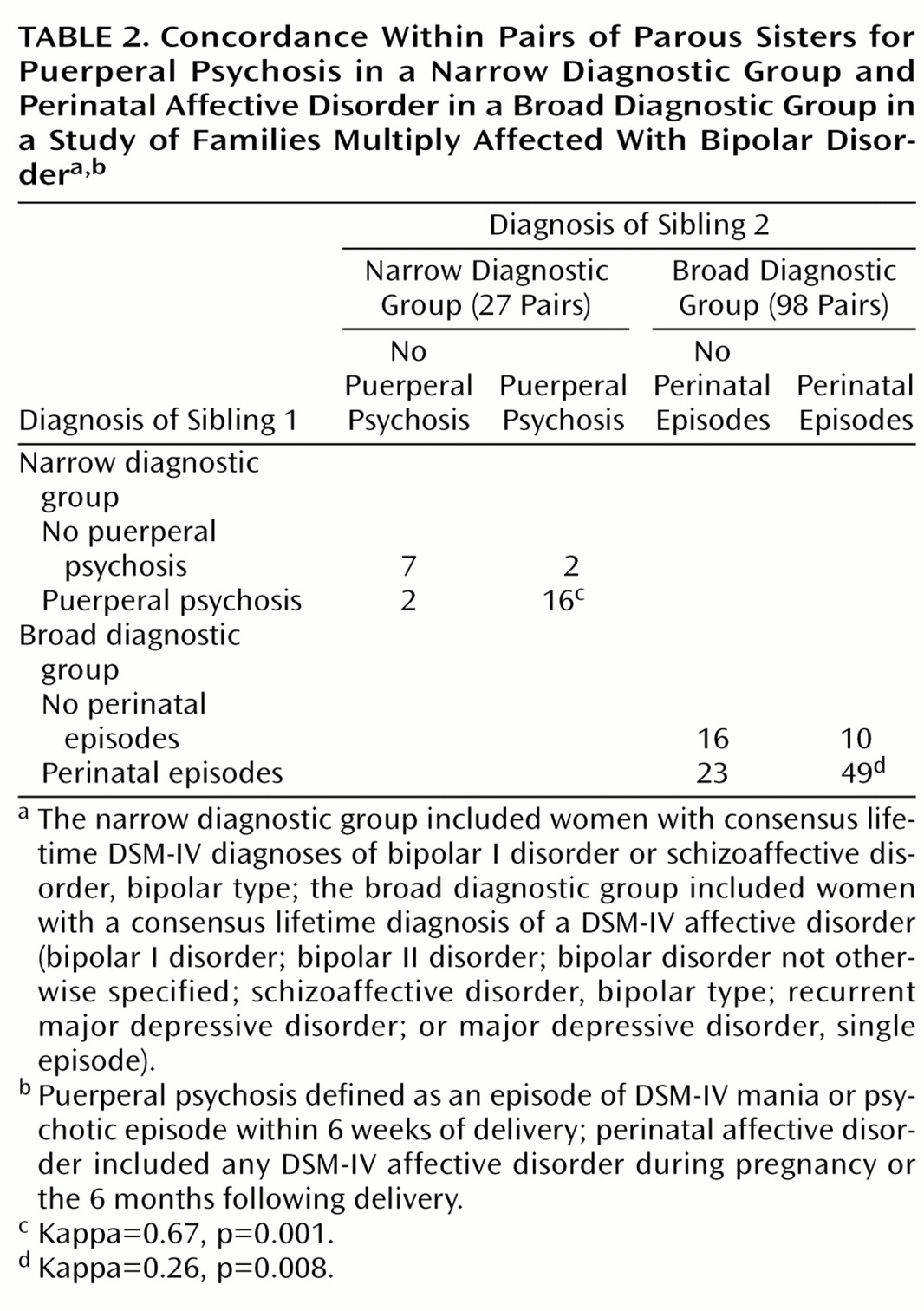
In the narrow diagnostic group, 23 of the 27 pairs of parous sisters were concordant for narrowly defined puerperal psychotic episodes; only four were discordant (
Table 2). For the same 27 sibling pairs, there was less marked familial clustering for the wider definition of perinatal episode, including all affective episodes in pregnancy or the puerperium (kappa=0.43, p=0.03). In the broad diagnostic group, 65 of 98 pairs of parous sisters were concordant for the relaxed definition of perinatal episodes (
Table 2).
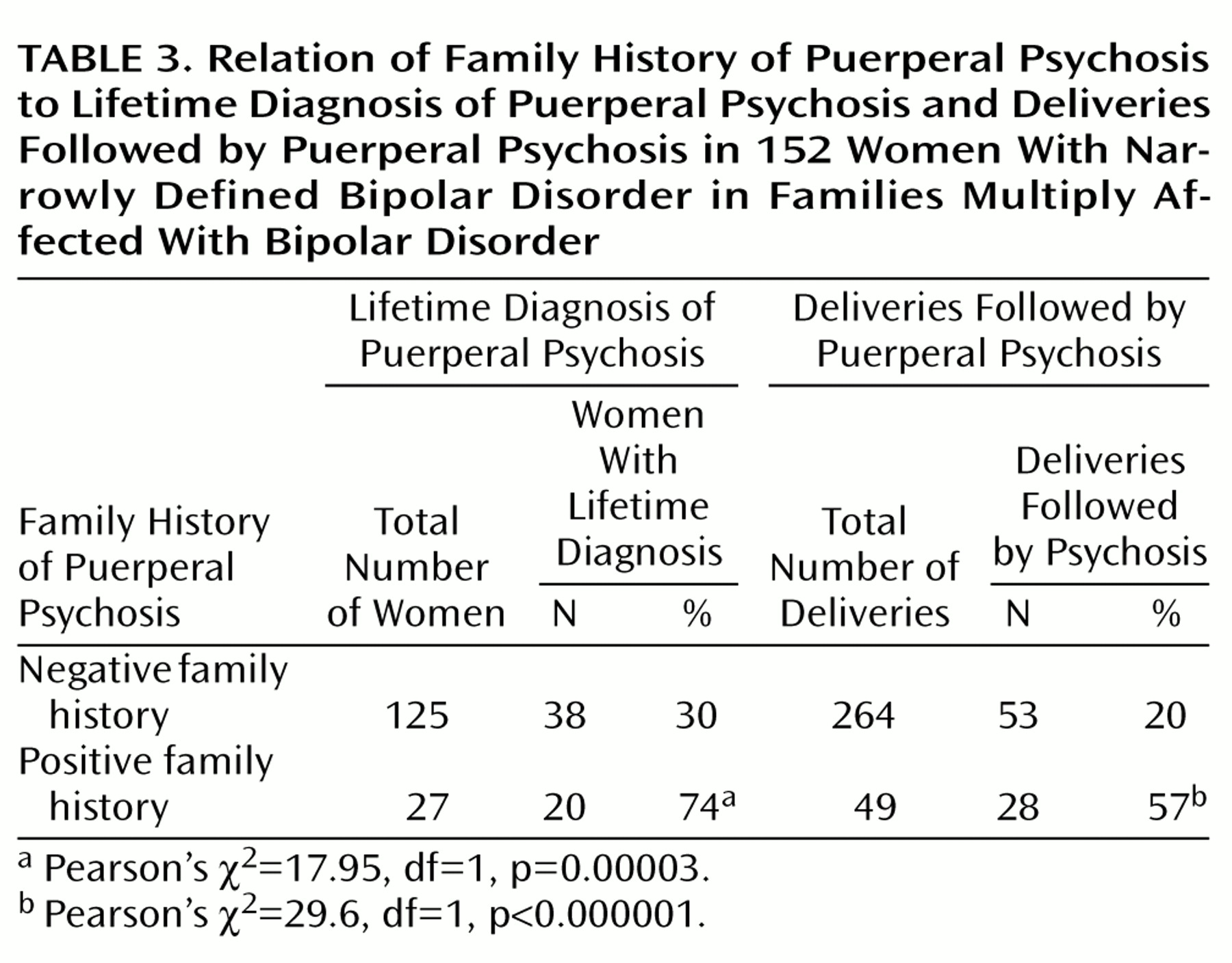
Of the 152 parous women in the group with narrowly defined bipolar disorder, 27 had a first-degree relative with a history of puerperal psychosis. Seventy-four percent of these women had themselves experienced an episode of puerperal psychosis, compared with only 30% of the women with bipolar disorder and no family history of puerperal psychosis (
Table 3). Women with bipolar disorder who had a family history of puerperal psychosis were at more than a sixfold greater risk of suffering an episode of puerperal psychosis (odds ratio=6.54, 95% confidence interval [CI]=2.55–16.76) and nearly a fourfold greater risk of suffering any perinatal episode of illness (odds ratio=3.83, 95% CI=1.25–11.74) than parous women with bipolar disorder who had no such family history (Pearson’s χ
2=6.14, df=1, p=0.02).
Sixty-nine (31%) of the 221 women in the broad diagnostic group had a first-degree relative with a history of a broadly defined perinatal episode. Fifty-one (74%) of the 69 women had themselves suffered an episode of perinatal affective disorder, compared with 87 (57%) of the 152 women with no such family history (Pearson’s χ2=5.63, df=1, p=0.02). Women with a family history of perinatal episodes were more than twice as likely to suffer an episode of perinatal affective disorder than women with no such family history (odds ratio=2.12, 95% CI=1.54–2.92).
The analysis of the lifetime occurrence of puerperal episodes does not take into account the fact that women differed in the number of episodes of parturition and the periods of risk to which they were exposed. Therefore, we analyzed the data for first pregnancies alone and for each individual pregnancy.
In the narrow diagnostic group, episodes of puerperal psychosis followed 66% (N=18) of first deliveries to women with a family history of puerperal psychosis but only 23% (N=29) of first deliveries to women with no such family history (Pearson’s χ
2=15.77, df=1, p=0.00008), a greater than sixfold increase in risk (odds ratio=6.1, 95% CI=2.34–15.97). For all pregnancies, episodes of puerperal psychosis followed 57% of deliveries to women with a family history of puerperal psychosis but only 20% of deliveries to women with no such family history (
Table 3) (under the assumption that each pregnancy can be treated as an independent event, odds ratio=5.31, 95% CI=2.80–10.08).
In the broad diagnostic group, an episode of perinatal affective disorder occurred in relationship to 56% (N=40) of first pregnancies in women with a family history of perinatal affective episodes but only 39% (N=40) of first pregnancies in women with no family history of perinatal episodes (odds ratio=2.01, 95% CI=1.09–3.69, Pearson’s χ2=5.09, df=1, p=0.03). For all pregnancies, episodes of perinatal affective disorder were associated with 40% (N=52) of deliveries in women with a family history of perinatal disorder but only 28% (N=95) of deliveries to women with no such family history (under the assumption that each pregnancy can be treated as an independent event, Pearson’s χ2=8.44, df=1, p=0.004, odds ratio=1.75, 95% CI=1.20–2.55).