Source of Data
Data were drawn from the National Ambulatory Medical Care Survey. The National Ambulatory Medical Care Survey, which is conducted annually by the National Center for Health Statistics, samples a nationally representative group of visits to physicians in office-based practice. We followed the recommendations of the National Center for Health Statistics in combining data from contiguous survey years to establish a larger base upon which to derive estimates. In order to detect changes in practice patterns in delivery of care through time, we grouped the visits from 1992 to 1995 and those from 1996 to 1999. Attending physicians or their office staff completed a one-page form about each patient visit. The form included basic demographic characteristics of the patients, their source of payment for the visit, their diagnoses, and their medications, including new prescriptions ordered, supplied, or administered and medications continued, with or without new orders. Only minor modifications were made to the survey between 1992 and 1999. The rate of response through the years varied from 70% to 73%.
Survey Design
The surveys were conducted by means of a three-stage sampling design. First, a probability sample of 112 primary sampling units (a county, a group of adjacent counties, or a standard metropolitan statistical area) was drawn, then a probability sample was drawn of practicing physicians within these primary sampling units, and, finally, a systematic random sample was drawn of the visits to these physicians over a 1-week period. Physicians who expected to see more than 10 patients per day recorded visits on the basis of a predetermined sampling interval. Some patient duplication may have occurred with this sampling strategy. The current analysis was confined to visits to psychiatrists.
Variables
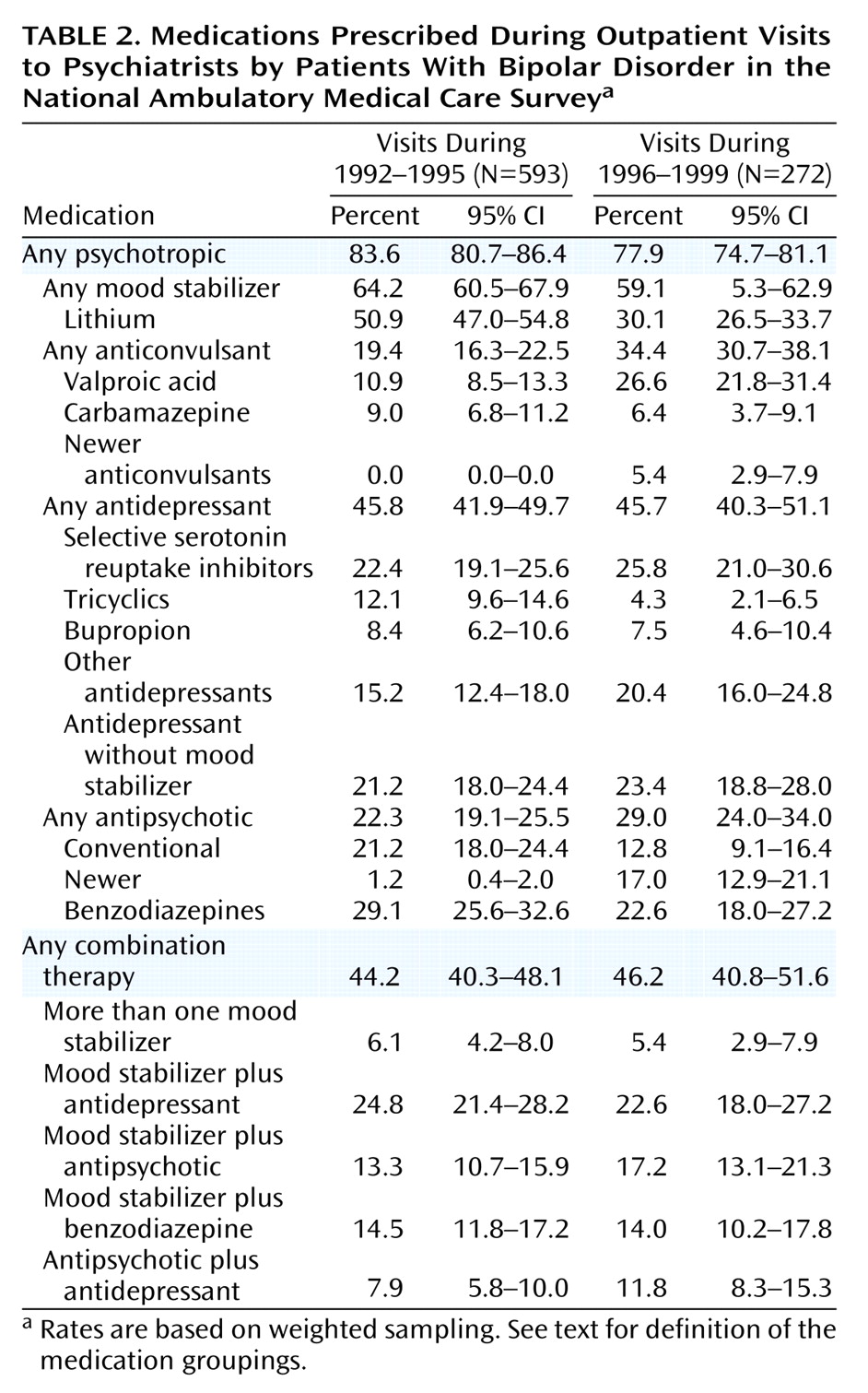
“Mood stabilizers” included lithium, carbamazepine, valproic acid, gabapentin, lamotrigine, and topiramate. “Antidepressant drugs” included tricyclic (and tetracyclic) antidepressants; the selective serotonin reuptake inhibitors (SSRIs) fluoxetine, sertraline, fluvoxamine, paroxetine, and citalopram; and “other antidepressants,” including trazodone, venlafaxine, nefazodone, and monoamine oxidase inhibitors. Because bupropion has been reported to have a lower incidence of medication-induced mania, it was considered as part of a special class of antidepressants for the purposes of our analyses.
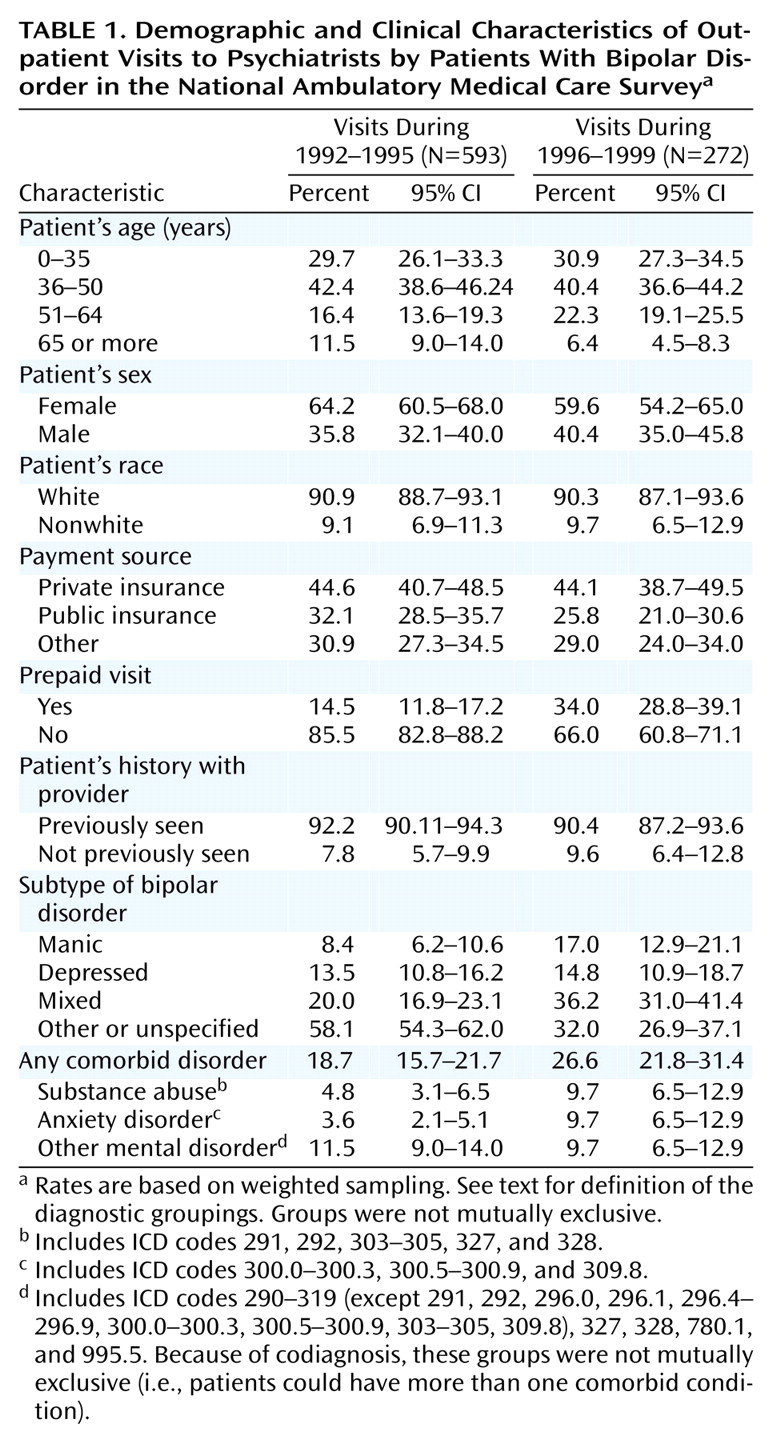
Data were collected regarding patient age, sex, and race, as determined by physician judgment. In addition, the surveys included a status code that classified visits according to whether the physician (or another physician in the same office) had ever seen the patient before.
Data collected on sources of payment for the visit were collapsed into three nonmutually exclusive categories: Medicare, Medicaid, and other government insurance were grouped together as “public insurance”; commercial insurance, including Blue Cross/Blue Shield, was considered to be “private insurance”; and a residual category was created that combined self-pay, uncompensated care, workers compensation, and unknown sources of payment. An additional variable was created to identify patient visits covered by prepaid plans, such as health maintenance organizations, independent practice associations, preferred provider organizations, and other prepaid arrangements.
Up to five ICD-9 codes were specified for each patient visit. Visits with codes 296.0, 296.1, or 296.4 were classified as regarding patients with bipolar mania. Visits assigned code 296.5 were classified as those by bipolar depressed patients. Visits that used code 296.6 were considered as regarding bipolar mixed patients, and visits assigned codes 296.7 or 296.8 were classified as for patients with bipolar disorder, unspecified. “Comorbidity” was defined as for visits assigned an additional code: 290–319, 327–328, 780.1, or 995.5.
Analysis
We examined rates per 100 psychiatrist visits by demographic and insurance characteristics of the sample, the patient diagnostic subtype, and the pharmacological management of the patient. We then examined the association of diagnostic and medication management characteristics of the visits with the patient demographic group, payment source for the visit, whether the patient was previously seen by the psychiatrist, patient diagnostic group, and number of diagnoses made during those visits.
In order to detect changes in practice patterns over time, we grouped the demographic and clinical characteristics of the patients visiting a psychiatrist from 1992 to 1995 and from 1996 to 1999 and compared the patterns of diagnosis and pharmacological treatment during both periods. Because sample sizes of the surveys were larger in the earlier years of the National Ambulatory Medical Care Survey, a larger proportion of the visits in which a diagnosis of bipolar disorder was made occurred from 1992 to 1995.