Previous studies have suggested that posttraumatic stress disorder (PTSD) is associated with small hippocampal size. Adults with PTSD related to combat exposure or childhood physical or sexual abuse have been repeatedly shown to have smaller hippocampal size, relative to healthy comparison subjects
(1–
7). However, two studies investigating children or adults with maltreatment-related PTSD failed to find smaller hippocampal size
(8,
9).
Research in nonhuman primates has suggested that stress and prolonged glucocorticoid exposure may damage the hippocampus
(10,
11), thus raising the possibility that traumatic stress or the chronic stress of having PTSD may induce hippocampal degeneration in humans. However, the mechanisms of possible stress-induced hippocampal degenerative changes in humans with PTSD are a matter of dispute
(12,
13). Another possibility is that preexisting small hippocampal size increases the risk for traumatic exposure or for developing PTSD
(14,
15).
The present study compared trauma-exposed subjects with PTSD and trauma-exposed subjects without PTSD to clarify whether small hippocampal size is related to PTSD or to trauma exposure (regardless of whether PTSD is present). Two studies have found that trauma-exposed subjects with PTSD had smaller hippocampal volumes than trauma-exposed subjects without PTSD
(3,
15), whereas another study
(16) did not. However, the latter study, which prospectively explored whether smaller hippocampal size occurs in recent trauma survivors with PTSD, did not include a healthy comparison group.
Studies investigating individuals with combat- or maltreatment-related PTSD revealed a high prevalence of substance-related disorders and depression
(1–
7,
15). These disorders were shown to be related to small hippocampal size as well
(17,
18). We decided to study individuals with a severe burn injury, as burn trauma is less often associated with comorbid conditions, compared with combat- or assault-related trauma
(19,
20).
Several studies have demonstrated that the strength of traumatic exposure is significantly related to PTSD severity
(2,
3,
21–23). Burn trauma results in PTSD less often than does combat- or assault-related trauma
(20,
24). More intense combat exposure increases the risk for developing PTSD
(19). In contrast, burns over a large body surface do not imply a heightened risk for developing PTSD
(20,
25), thus facilitating the recruitment of PTSD and non-PTSD study groups with a comparable severity of traumatic exposure.
In the present investigation the hippocampal volumes of 15 adult burn patients with PTSD and 15 adult burn patients without PTSD were compared to those of matched healthy subjects (N=15). The goals of the study were 1) to investigate whether hippocampal size is smaller in trauma-exposed subjects who do not show evidence of confounding comorbid conditions, 2) to investigate whether hippocampal size is smaller in trauma-exposed subjects without PTSD, 3) to investigate whether hippocampal size differs between subjects with and without PTSD, and 4) to analyze the relationship between traumatic stress-related variables and hippocampal size.
Method
Subjects
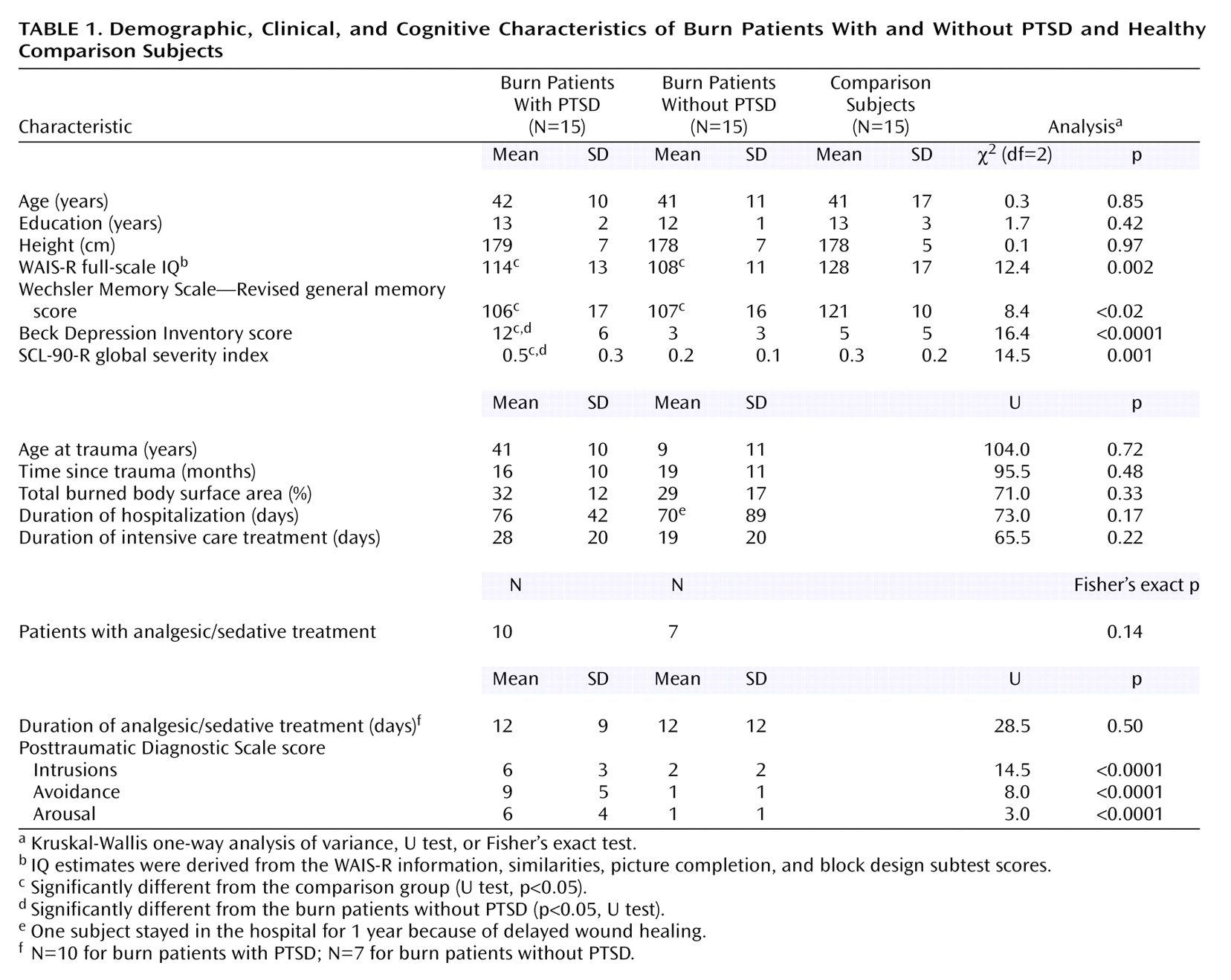
Thirty men who had been exposed to a severe burn trauma between 1999 and 2000 participated in the study (
Table 1). Of the injuries, 60% occurred at work, 27% occurred at home, and 13% happened elsewhere. Explosions caused 30% of the injuries, and scalding accounted for 30%, flames for 17%, electric current for 10%, and other agents for 13%.
All trauma-exposed subjects were recruited from three regional burn centers (Berufsgenossenschaftliches Unfallkrankenhaus Hamburg, Berufsgenossenschaftliche Unfallklinik Berlin-Marzahn, Städtische Kliniken Dortmund Nord-Unfallklinik). Of 214 men contacted, 132 were interested in participating in the study. Of these subjects, 91 were excluded because of a neurological, substance-related, or depressive disorder; because of a history of previous trauma; because they sustained brain injury as part of the trauma; or because their medical or personal condition did not allow traveling and a 2-day stay in the Psychiatric Hospital of the University of Göttingen for the study. Forty-one subjects were invited to participate. Of these subjects, three refused to participate and two were excluded because a neurological disorder became evident during the investigation. Fifteen subjects met the criteria for PTSD, and 21 subjects did not have PTSD. Six of the subjects without PTSD were not included in the analyses described in this report because they could not be adequately matched to the subjects with PTSD according to age, height, education, age at time of the traumatic event, and burn size.
Fifteen subjects met the DSM-IV criteria for chronic PTSD on the basis of interviews with the Structured Clinical Interview for DSM-IV (SCID). In all of these subjects, PTSD occurred shortly after the traumatic event. The other 15 subjects confirmed diagnostic criterion A, but none or at most one of criteria B–D. All subjects were free of any other current or lifetime axis I or axis II DSM-IV disorder according to the SCID interview. At the time of assessment, 80% of the subjects with PTSD and 80% of the subjects without PTSD were employed full- or part-time. None of the subjects received psychotropic medication.
The trauma-exposed subjects were compared with 15 healthy male subjects who were matched with the trauma-exposed subjects for age, height, and years of education. The comparison subjects were recruited by means of an advertisement in a local newspaper and leaflets distributed in the hospital of the University of Göttingen and in the town of Göttingen. Only subjects without a history of neurological or psychiatric disorder (as assessed by the SCID) were included. After a complete description of the study to the subjects, written informed consent was obtained.
Clinical Assessment
The Posttraumatic Diagnostic Scale
(26) was used as a measure of PTSD severity. Depressive symptoms were assessed with the Beck Depression Inventory
(27). The global severity index of the Symptom Checklist (SCL-90-R)
(28) was used as a measure of the overall level of distress. The WAIS-R
(29) and the Wechsler Memory Scale—Revised
(30) were used to assess intellectual and mnemonic functions. Subjects also received a more comprehensive neuropsychological (a computer-driven test battery for attentional functions and various memory tests) and psychopathological (stress coping and personality questionnaires) assessment. Results of these assessments will be reported elsewhere.
The objective severity of the traumatic stressor was assessed by the total burned body surface area (
Table 1). Seventeen burn patients received analgesic/sedative therapy because of repeated surgery or severe pain caused by the removal and replacing of bandaging material or because of smoke poisoning or head burns that made endotracheal intubation for maintenance of an imperiled airway necessary. We assessed the duration (days) of analgesic/sedative therapy to evaluate the effects of this medical treatment (
Table 1).
Magnetic Resonance Image (MRI) Acquisition and Analysis
All subjects received an MR scan, obtained by using a 1.5-T Philips Gyroscan machine (Philips Medical Systems, Best, the Netherlands). Scanning parameters of the T1-weighted three-dimensional sequence were as follows: TE=6.0 msec, TR=24.0 msec, flip angle=30°, field of view=256, sagittal slice plane, matrix=256×256, slice thickness=1.3 mm, slice number=130, three-dimensional acquisition mode. Volumetric analysis was done on the basis of three-dimensional MR images. The images were transferred to a computer workstation and processed by using the CURRY software (version 4.5, Neurosoft, Inc., El Paso, Tex.). Images were reformatted into continuous slices of 1-mm thickness.
Total brain volume was calculated with automated multistep algorithms and three-dimensional region growing methods that are limited by gray matter value thresholds. Volumetric analysis of the hippocampus was done by using three-dimensional software (CURRY) that allows simultaneous analysis of sagittal, coronal, and horizontal images. The hippocampus was disarticulated from surrounding tissue on coronal slices by means of manual tracing according to a standardized protocol
(31) and by aid of the serial sections provided by Duvernoy
(32). The horizontal and sagittal views were consistently employed in addition to the coronal view for the demarcation of the borders of the hippocampus. All analyses were done by a single rater who was blind to the subjects’ diagnostic information. For defining the intrarater reliability of the demarcation of the hippocampus, one hemisphere image for 11 randomly chosen subjects was reassessed. The intraclass correlation coefficient for this procedure was 0.94.
Statistical Analysis
Because of the small sizes of the study groups, group comparisons were performed by using nonparametric statistical methods. Kruskal-Wallis analyses of variance (ANOVAs) and U tests were applied to compare differences between groups in demographic, clinical, and cognitive variables and in total brain volume. Partial correlation coefficients with adjustment for total brain volume were used to examine the relationship between hippocampal size and demographic, clinical, and cognitive variables.
The hippocampal volumes of the trauma-exposed subjects and the healthy subjects were compared by an overall nonparametric three-by-two analysis of covariance (ANCOVA)
(33), with group as the between-subjects factor (trauma subjects with PTSD, trauma subjects without PTSD, comparison subjects) and hemisphere as the within-subjects factor (left, right) and with adjustment for total brain volume. This model was followed up by separate two-by-two (group-by-hemisphere) ANCOVAs and univariate ANCOVAs for the left and right hippocampus volumes, respectively. The relationship between traumatic stress-related variables and hippocampal volumes was further examined with multiple regression analyses.
All analyses were two-tailed, and alpha was defined as p<0.05. Statistical computations were performed by using SAS for Windows, Version 8.01 (SAS Institute, Cary, N.C.), nonparametric ANCOVAs (http://www.ams.med.uni-goettingen.de/de/sof/ld/NPAR.SAS), and SPSS for Windows, Version 10.0 (SPSS, Inc., Chicago).
Results
Subject Characteristics
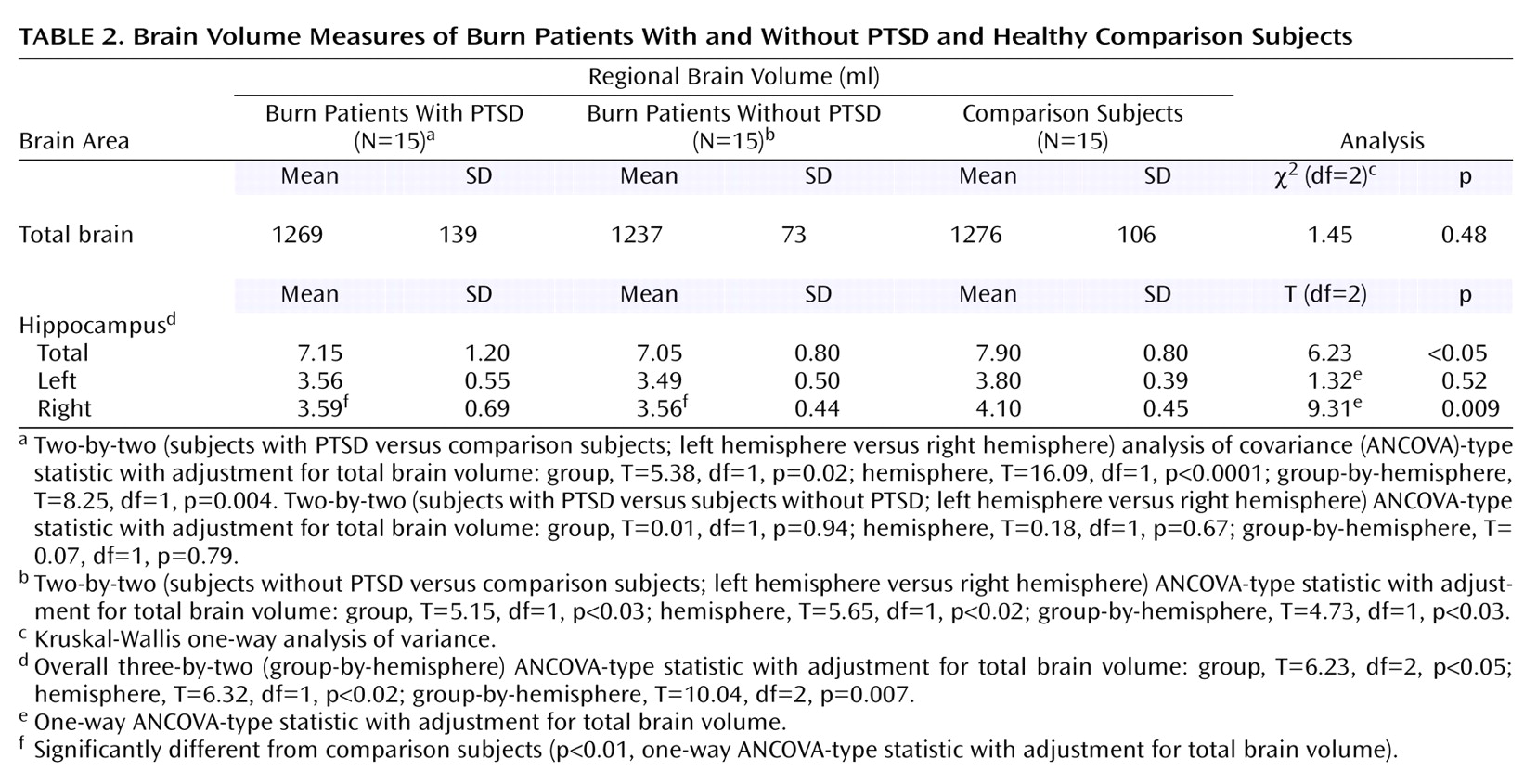
The groups did not differ with respect to demographic variables or total brain volume (
Table 1 and
Table 2). Both trauma-exposed groups had significantly lower general intelligence and memory test scores, compared with the healthy subjects. The trauma-exposed subjects with PTSD showed significantly higher scores on the Posttraumatic Diagnostic Scale, Beck Depression Inventory, and SCL-90-R global severity index, compared with the trauma-exposed subjects without PTSD. According to normative data from the Posttraumatic Diagnostic Scale
(26), one of the PTSD subjects had very severe PTSD, five subjects had severe PTSD, eight had moderate PTSD, and one had mild PTSD. There were no significant relationships between burn type (see Method section, Subjects subsection) and hippocampal volume or any clinical variable (ANCOVAs, ANOVAs).
Seventeen trauma-exposed subjects received analgesic/sedative therapy as part of the medical treatment (
Table 1). In all of these cases, a ketamine/benzodiazepine combination and an opioid/benzodiazepine combination were applied in an alternating manner. Subjects who did not receive analgesic/sedative treatment sometimes received short anesthesia for surgery or for replacing of bandaging material. In the majority of these cases, anesthesia was performed with opioids. Subjects with analgesic/sedative treatment had higher Posttraumatic Diagnostic Scale symptom scores, compared with subjects without analgesic/sedative treatment (intrusions: mean=5 [SD=4] versus mean=2 [SD=2] [p<0.04, U test]; avoidance: mean=6 [SD=5] versus mean=2 [SD=2] [p<0.03, U test]; arousal: mean=4 [SD=4] versus mean=2 [SD=2] [p<0.03, U test]). Comparisons of these two subgroups on all other variables were not significant.
Hippocampal Volume: Group Comparisons
Relative to the healthy comparison subjects, trauma-exposed subjects had smaller volumes of the right hippocampus (subjects with PTSD: –12%; subjects without PTSD: –13%) and left hippocampus (subjects with PTSD: –6%; subjects without PTSD: –8%).
The overall three-by-two (group-by-hemisphere) ANCOVA yielded significant effects of group, hemisphere, and group-by-hemisphere, indicating significantly smaller hippocampal size in trauma-exposed subjects, relative to the comparison subjects (
Table 2). The follow-up two-by-two (group-by-hemisphere) ANCOVAs for each trauma group and the comparison group confirmed these results. The two-by-two (group-by-hemisphere) ANCOVA for the two trauma groups did not reveal any significant effects, indicating similar hippocampal size in both groups. Univariate ANCOVAs revealed that the smaller hippocampal size of both trauma groups was statistically significant for the right hemisphere, but not for the left hemisphere. The detailed results of all statistical comparisons are given in
Table 2.
Relative to the comparison subjects, the trauma-exposed subjects who received analgesic/sedative treatment (N=17) (
Table 1) had smaller volumes of the left (–5%) and right (–9%) hippocampus. However, the difference in hippocampal volume for the trauma-exposed subjects who did not receive analgesic/sedative treatment was larger (left hippocampus: –10%, right hippocampus: –17%). Univariate ANCOVAs with adjustment for total brain volume revealed that the subjects without analgesic/sedative treatment (T=15.67, df=1, p<0.0001) but not those who received analgesic/sedative treatment (T=2.91, df=1, p=0.0898) had significantly smaller right hippocampal size, relative to the comparison subjects. The difference between the two trauma-exposed groups was not significant (p>0.10). The same was true for all comparisons of left hippocampal volumes (p>0.30).
Relationship Between Hippocampal Volume and Traumatic Stress-Related Variables
The total burned body surface area, global severity index, Posttraumatic Diagnostic Scale total score, and Beck Depression Inventory score were entered into stepwise multiple regression analyses (significance level for selecting variables: p=0.05). Total brain volume was entered as a further predictor to control for the influence of brain size. Considering all trauma-exposed subjects, total brain volume (proportion of explained variance [R2]=0.45, p<0.0001) and total burned body surface area (R2=0.11, p<0.03) significantly predicted left hippocampal volume, indicating smaller hippocampal volumes in subjects with larger burns. The addition of the other variables did not significantly improve the prediction.
Multiple regression analyses were also conducted for the 17 subjects who received analgesic/sedative treatment. Total burned body surface area, global severity index, Posttraumatic Diagnostic Scale total score, Beck Depression Inventory score, total brain volume, and duration (days) of analgesic/sedative treatment were used as predictors. Total brain volume (R2=0.56, p<0.0001), Posttraumatic Diagnostic Scale score (R2=0.11, p<0.05), and total burned body surface area (R2=0.09, p<0.05) significantly predicted left hippocampal volume, indicating smaller hippocampal volumes in subjects with larger burns and more severe PTSD symptoms. Total brain volume (R2=0.63, p<0.0001), Posttraumatic Diagnostic Scale score (R2=0.15, p=0.007), and duration of analgesic/sedative treatment (R2=0.06, p<0.04) significantly predicted right hippocampal volume, indicating smaller hippocampal volumes in subjects with shorter duration of analgesic/sedative treatment and more severe PTSD symptoms.
Relationship Between Hippocampal Volume and Demographic, Clinical, and Cognitive Variables
In trauma-exposed subjects (N=30), left and right hippocampal volumes were not significantly related to age, education, age at the time of the traumatic event, past time since the traumatic event, duration of hospitalization, duration of intensive care treatment, IQ, and memory test score, respectively (all p>0.15). The same was true when the subgroup of subjects who received analgesic/sedative treatment (N=17) was considered (p>0.10).
Discussion
Our results demonstrate small hippocampal size in individuals who experienced a severe burn trauma and complement earlier findings of small hippocampal size in individuals who were exposed to combat or maltreatment. Consistent with previous findings in persons who were exposed to trauma as adults
(1,
3,
15), we found predominantly small right hippocampal volumes in this group of adult burn patients. In contrast, small left hippocampal size is frequently observed in persons with prepubertal traumatic experiences
(2,
4,
7).
The trauma-exposed subjects in our study, although as well educated as the healthy comparison subjects, showed significantly lower intellectual and mnemonic functions (compare with
Table 1). Neuropsychological impairments in the domain of intelligence and memory were also reported for Vietnam combat veterans
(1,
21) and adult survivors of childhood physical or sexual abuse
(21,
34).
In contrast to PTSD study groups who were exposed to combat or maltreatment
(1–
7,
15), the burn patients in the present study did not present with substance-related disorders or major depression, which have been shown to be related to small hippocampal size as well
(17,
18). Our results clearly argue against the assumption that trauma-related small hippocampal size may be solely an effect of these confounding comorbid conditions.
Small Hippocampal Size in Trauma-Exposed Individuals Without PTSD
The results of our study demonstrate that trauma-exposed subjects without PTSD (or any other current or lifetime psychiatric diagnosis) have smaller hippocampal size, relative to healthy comparison subjects. Thus, PTSD may not be a necessary condition for small hippocampal size in trauma-exposed individuals. A study of Vietnam combat veterans did not find significantly smaller hippocampal size in combat veterans without PTSD, relative to healthy comparison subjects
(3). However, in that study, the difference in size of the right hippocampus of the combat veterans without PTSD, relative to healthy comparison subjects, was similar in magnitude (–11%) to that of the burn patients without PTSD in the current study (–13%) and may have failed to reach statistical significance because of the small number of subjects (combat veterans: N=7; comparison subjects: N=8).
In the current study, the trauma-exposed subjects with PTSD did not differ in hippocampal size from the trauma-exposed subjects without PTSD. Similar results were obtained in individuals who were exposed to accidents
(16). PTSD severity, as measured with the Clinician-Administered PTSD Scale, was moderate in this PTSD study group (mean score=58)
(16). A moderate PTSD severity was also present in the PTSD group in the current study. In contrast, in two studies of Vietnam combat veterans that found smaller hippocampal size in subjects with PTSD, compared to subjects without PTSD, the mean Clinician-Administered PTSD Scale scores of the study groups with PTSD were >70
(3,
15). These findings raise the possibility that more severe, long-lasting, and unremitting forms of PTSD are more likely to be associated with small hippocampal size. This conclusion is supported by our multiple regression analyses, which revealed an association of PTSD symptoms and hippocampal size only in the subgroup of trauma-exposed subjects who received analgesic/sedative treatment. This subgroup presented with significantly stronger PTSD symptoms, compared to the subjects who did not receive analgesic/sedative treatment.
Small Hippocampal Size as a Result of Traumatic Stress
We found a relationship between larger burn size and smaller hippocampal volume in the trauma-exposed subjects in our study. Therefore, it could be assumed that traumatic stress by itself results in some kind of damage to the hippocampus. A similar relationship between severity of traumatic stress and hippocampal size was obtained in Vietnam combat veterans
(3) and in subjects with childhood physical or sexual abuse
(5). However, other studies failed to find a relationship
(1,
2,
4,
7,
15). Our results suggest the need to explore the extent of physical trauma in PTSD study subjects who have sustained significant physical injuries.
None of the trauma-exposed subjects in our study displayed any neurological or neuropsychological abnormalities at time of our assessment. Furthermore, subjects who sustained brain injury as part of the trauma were rigorously excluded (see Method section, Subjects subsection). However, encephalopathy or delirium due to hypoxia or multiple metabolic aberrations is a common event in burn victims
(35,
36), although the majority of patients recover from these conditions. There is also evidence that burn trauma leads to substantially increased cortisol levels
(37). Probably, the reduced hippocampal volumes of the burn patients in our study are related to these factors. The hippocampus is known to be especially vulnerable to hypoxia and metabolic insults
(32).
Multiple regression analyses showed a negative relationship between left hippocampal volume and burn size and a positive relationship between right hippocampal volume and duration of analgesic/sedative treatment. Single correlations, with adjustment for total brain volume, between burn size or analgesic/sedative treatment and left or right hippocampal volume were significant (r=–0.43, r=0.50, and r=0.54, p<0.05), except for the relationship between burn size and right hippocampal volume (r=–0.05, p>0.80). The functional significance of this finding remains to be elucidated.
Effects of the Analgesic/Sedative Treatment
We observed a relationship between longer duration of analgesic/sedative treatment and larger hippocampal volume. Group comparisons revealed that the difference in hippocampal size in the subjects with analgesic/sedative treatment, relative to the healthy subjects, was of less magnitude than the difference in the subjects without analgesic/sedative treatment. It could be speculated that the analgesic/sedative treatment might have had a protective effect on the hippocampal neurons of the burn patients in the present study. Animal studies demonstrated that
N-methyl-
d-aspartic acid (NMDA) glutamate receptor activation inhibits hippocampal neurogenesis
(38) and that NMDA antagonists protect hippocampal neurons from acute ischemic injury
(39). Ketamine, which was used as an analgesic/sedative agent in the burn patients in this study, is an NMDA antagonist. Possibly, the pertinent use of combined ketamine/benzodiazepine sedation offers a powerful tool for neuroprotection while largely preventing the unwanted side effects of NMDA antagonists
(40).
Trauma-exposed subjects who received analgesic/sedative treatment presented with significantly stronger PTSD symptoms than subjects who did not receive this treatment. However, the subjects who received analgesic/sedative treatment did not differ in burn size or with regard to any other variable from the subjects who did not receive analgesic/sedative treatment. Possibly, the enduring posttraumatic application of the NMDA antagonist ketamine increased the vulnerability of the burn patients to develop PTSD symptoms. The subanesthetic application of ketamine in humans is known to produce dissociative cognitive and perceptual alterations
(41). Preclinical data suggest that NMDA antagonists may produce these effects by a transient stimulation of corticolimbic glutamate release
(42).
Conclusions
We found smaller hippocampal size in a group of burn patients without any confounding comorbid psychiatric disorders. Our results indicate that PTSD is not a necessary condition for small hippocampal size in trauma-exposed individuals. In addition, our results suggest the need to explore the extent of physical trauma in trauma-exposed study subjects who have sustained significant physical injuries. Furthermore, our results suggest that the posttraumatic application of NMDA antagonists probably protects against hippocampal damage induced by traumatic stressors but may increase the risk for developing PTSD symptoms. Future studies are needed to explore the therapeutic potential of drugs that attenuate glutamate release in individuals who have been exposed to traumatic stress.