Suicide, currently the 11th leading cause of death in the United States, accounted for 29,350 deaths in 2000
(1). It is estimated that there are 10–20 suicide attempts for every completed suicide. Despite the staggering morbidity and mortality associated with these behaviors, there is a dearth of demonstrated effective interventions. Although medications such as clozapine
(2) and lithium
(3) have been suggested to have antisuicidal properties, clozapine is the only drug with U.S. Food and Drug Administration (FDA) approval for the treatment of suicidal behavior. A handful of studies are under way to assess both psychosocial and pharmacological interventions that may be useful in at-risk populations (National Institute of Mental Health Computer Retrieval of Information on Scientific Projects database, February 2003). However, a 2002 report by the Institute of Medicine
(4) called for an increase in intervention studies focusing on suicidal behaviors. Planning such intervention studies is bound to raise complex bioethical issues for the investigator.
Bioethical Issues in Intervention Research for Suicidal Behavior
Designing intervention research with suicidal subjects while maintaining adherence to the ethical domains outlined in the 1998 Belmont Report
(5) on protection of human research subjects is fraught with difficulty. This landmark report, which is the basis for federal regulations for research involving human subjects, proposed that research ensure respect for persons, beneficence, and justice. Respect for persons is reflected in the informed consent process, through which the researcher provides information and assesses the subject’s capacity and the subject gives voluntary written consent. Beneficence is attained by maximizing the benefits of the study design while keeping risks to a minimum. Justice is the equitable selection of subjects so that the burdens and benefits of research are distributed fairly. All three areas pose challenges for the design of studies targeting suicidal acts.
How respect for persons through the informed consent process can be guaranteed in studies that include mentally ill subjects in general has been often debated
(6,
7). Concerns about whether psychiatric patients can truly have capacity to consent or can participate in research voluntarily are central issues in this debate. Similar concerns have been raised about the capacity and voluntarism of suicidal subjects
(8). Furthermore, intervention studies for suicidal behavior are expected to have some lethal outcomes
(9), as is the case in treatment trials in conditions with high mortality such as malignancies or end-stage coronary artery disease. As individuals become suicidal, impaired capacity may be reflected in unwillingness to stay in the protocol and to accept interventions to reduce mortality, which are ordinarily considered to be in the individual’s interest. Thus, research on lethal psychiatric illnesses is conducted in a population vulnerable to fluctuations in capacity, creating an ethical tension between voluntariness and clinical care. If a subject consents to a study with procedures for detection and prevention of suicide risk and such interventions are to be implemented in risk situations, the research clinician may face the decision of what to do if a subject refuses interventions that are both part of the protocol and indicated clinically. Ordinarily the research subject is free to discontinue participation. But if the subject wishes to decline an intervention yet in the clinician’s judgment is at acute risk, how should the patient’s right to refuse participation be maintained when discontinuation of study participation may be a harbinger of imminent suicide risk? In addition, if the most acutely suicidal patients drop out, bias is created because the information on whether they ultimately die by suicide will not be collected. Such clinical, methodological, and ethical dilemmas illustrate informed-consent issues particular to suicidal subjects and have been a focus of attention for intervention researchers
(10; see also http://www.nimh.nih.gov/suicideresearch/highrisksuicide.cfm).
In a review of safety and ethical issues in intervention research for suicidal behavior, Pearson et al.
(10) illustrated the difficulties of maintaining beneficence (see also http:// www.nimh.nih.gov/suicideresearch/highrisksuicide.cfm). The need for increased monitoring of suicidal subjects, even in studies that compare treatment as usual to a given intervention, introduces methodological complications. It adds standardization to a condition that, by its very nature, is not supposed to be standardized, and it may have an effect on the outcome measure, suicidal acts
(11). Indeed, if surveillance is too good, the outcome measure rate may decrease in a way that is inconsistent with “real-world” conditions, which at a minimum diminishes the study’s ecological validity and at worst makes the study impossible to conduct. Enhanced monitoring of suicidal acts may also decrease statistical power to detect a treatment effect on suicidal behavior, necessitating a larger sample. For example, assume that two suicide prevention treatments result in suicide attempts in 20% and 40% of the study population, respectively. Assume further that surveillance alters the outcome rate equally in both treatments, to 10% and 30%, respectively. This change may decrease the effect size, depending on how it is calculated, and consequently affect the risk-benefit ratio. Moreover, the number of suicide attempts needed for comparison may be greater, depending on the impact of surveillance on effect size. Nonetheless, in our opinion,
on a patient-year basis, subjects are safer in a monitored study than in an unmonitored study.
Investigators have grappled with the decision about whether to design a study that distributes risk evenly across the population to be studied by including suicidal individuals or to protect these vulnerable subjects by not exposing them to the risks of randomization. Generally, studies have opted to protect suicidal patients by exclusion. Thus, beneficence and risk minimization are at the heart of decisions to exclude suicidal subjects from clinical trials. However, these decisions lead to an unfortunate decrease in justice, because equal selection of subjects is not possible. The price of this choice is a paucity of information about the efficacy of treatments for precisely those persons with the highest-risk psychiatric disorders, actively suicidal individuals. Not only is there scant information about effective interventions to prevent suicidal acts, but it is also unknown whether suicidal patients have intrinsically different responses to psychopharmacological and psychological interventions.
Post and Luckenbaugh
(12) described reasons for the paucity of randomized, controlled trials in bipolar disorder, in which suicidal behavior is common. For example, existence of effective treatments for bipolar disorder, a high-risk disorder, makes it nearly impossible to implement a placebo-controlled trial. Characteristics of the disorder, such as the occurrence of various mood states requiring different pharmacological interventions and the high incidence of suicidal acts, are additional difficulties. About 20% of patients with bipolar disorder end their own lives
(13). In epidemiologic samples, about 29% of respondents with bipolar disorder acknowledge a suicide attempt in their lifetime
(14). In addition, although numerous studies have prospectively examined risk factors for suicidal acts in mood disorders (unpublished review by M.A. Oquendo and J.J. Mann), there is still no reliable way of using known risk factors to anticipate risk. Despite the enormity of this public health problem, few prospective studies have examined interventions to prevent suicidal acts in bipolar disorder
(3).
To our knowledge, there are no reports on ethical and practical issues surrounding the daunting task of enrolling bipolar disorder subjects at risk for suicide into randomized, controlled trials. We describe experience in a federally funded randomized, controlled trial currently under way that is designed to assess pharmacotherapeutic effects on suicidal acts in bipolar disorder and describe strategies to protect human subjects in intervention research for suicidal behavior. Although the focus is on bipolar disorder, the issues addressed are pertinent to intervention research in other conditions associated with suicidal behavior.
Study Design
A 2.5-year randomized, controlled trial design compares the effects of lithium and valproate on suicidal behavior in patients with bipolar disorder. A treating psychiatrist, who is blind to the study medications, is advised by an unblinded, nontreating psychiatrist about study drug dosing on the basis of blood levels, protecting the double blind. The blinded psychiatrist uses both clinical assessment and dosing recommendations in decision making.
Study Population
To ensure generalizability to bipolar disorder populations at risk for suicidal acts, subjects with all bipolar disorder subtypes (I, II, and not otherwise specified) are enrolled as either outpatients or inpatients. Patients with comorbid substance abuse, personality disorders, or psychosis are included. This strategy maximizes equal selection of subjects, or justice. However, since suicidal acts are relatively rare, only bipolar disorder subjects with a previous suicide attempt who were currently in a mixed or depressed state, the phases of bipolar disorder associated with high suicidal risk
(15–
18), are enrolled. These latter strategies may counterbalance the loss of statistical power due to surveillance of suicidal behavior and increase the beneficence of the design.
Comparator Drugs
The comparator drugs are lithium and valproate, the only FDA-approved medications for treatment of bipolar disorder at the time of the study design. Lithium is the test drug for an antisuicidal effect, and valproate is a control for the benefits of mood stabilization. Extensive, mostly uncontrolled, European data suggest that lithium has antisuicidal properties independent of its mood stabilization properties
(3). Choosing these comparators enhanced beneficence, since the risks of mood instability are minimized while the main hypothesis—whether lithium has antisuicidal effects—is addressed.
Informed Consent
At two separate points, the study is described to all potential participants by a clinician. All clinicians have a minimum of master’s-level training in psychology. As a rule, there is an initial contact by telephone in which the patient receives both a brief screening interview and a general description of the study from a clinician. If the patient expresses interest, he or she is evaluated in person by two clinicians, a research psychiatrist and a psychologist. The research psychiatrist conducts a formal informed consent interview during which the patient’s capacity is assessed and documented. In-person assessment by two clinicians increases surveillance for signs of impaired capacity as well as evidence of imminent suicide risk. Acutely ill psychiatric patients who are deemed to be imminently suicidal are hospitalized. Because such patients may be at increased risk for lack of capacity to consent, the subjects who require hospitalization at study entry have an independent assessment of capacity by the clinical team on the inpatient unit, who have no direct involvement in the study. These procedures may assist in the identification of potential subjects who lack capacity to give informed consent. In addition, because of anticipated suicidal behavior, the informed consent process includes a discussion about clinical monitoring, availability of hospitalization as an intervention, and the staff’s mandate to act in the face of acute suicide risk. This discussion bolsters respect for participants by informing subjects of procedures to be implemented in situations of acute suicide risk during which the subject may wish to decline study participation.
Conducting the Study in Phases to Address Phases of Illness
During the acute stage, mood is stabilized with the double-blind study medication—lithium or valproate—and an antidepressant if the patient is currently experiencing a major depressive episode or an antipsychotic if the patient is in a mixed episode. Algorithms that include different antidepressants or antipsychotics are available, so that the patient’s failure to respond to one triggers a switch to another in a different class (e.g., failure to respond to 40 mg/day of paroxetine for 6 weeks leads to a switch to bupropion). The second or continuation phase starts when the subject has been euthymic for 2 weeks. The subject continues to take the study medication and antidepressant for 6 months or to take the study medication and antipsychotic for 2 months. The third phase, an 18-month maintenance phase, occurs after the subject’s antidepressant or antipsychotic has been tapered off and the subject is receiving only the maintenance study medication. It is in this third stage that the hypothesis can be tested. However, because of the nature of the illness, intervention algorithms for new mood episodes are required, and their availability simultaneously increases feasibility and beneficence.
Flexible Algorithm to Treat Emerging Mood Episodes
Given the likelihood of relapse into different phases of illness, a treatment plan derived from consensus recommendations
(19) and evidence-based strategies
(20) is in place. Algorithms allow the research psychiatrist to add “rescue medications” in an open fashion. For example, the psychiatrist may sequentially add up to three predetermined antidepressants if the patient becomes depressed or three predetermined antipsychotics if manic or mixed states develop. Once the subject becomes euthymic, rescue drugs are withdrawn and the subject continues to take only the double-blind study drug. Thus, the study can be conducted in the face of mood instability, a difficult issue in the design of randomized, controlled trials for bipolar disorder
(12). Further, the fact that clinicians respond to individual needs enhances beneficence, yet in a quantifiable fashion, which facilitates data analyses.
Protection of Human Subjects
The challenges of protecting human subjects were a focus from the early stages of design. Data needed to be gathered in this high-risk population while maximally reducing morbidity and mortality. With these goals in mind, six separate strategies are integrated into the study design.
Surrogate Outcome Measures to Protect Subjects From Actual Suicidal Acts
The outcome measure is time of survival until one of three events: 1) hospitalization or implementation of rescue procedures for suicidal ideation involving a plan, 2) suicide attempt, or 3) suicide completion. Suicide planning is operationalized. If the patient acknowledges one or more planning items in the Scale for Suicide Ideation
(21), such as writing a suicide note, research clinicians intervene with hospitalization, a change in medication, or increased monitoring. Thus, the study design encourages suicide prevention while measuring drug effects on the occurrence of clinical situations associated with imminent suicidal acts, as well as on actual suicide attempts or completions. This approach is not without problems, since it cannot be ascertained whether interventions in fact aborted a suicidal act or were responses to “false alarms” in which a suicidal act would not have occurred.
No Placebo Control
A placebo condition was not included. The efficacy of lithium and valproate in bipolar disorder is well established, and it was deemed unethical to maintain high-risk subjects without medication. In particular, the study objective was not treatment efficacy in general but efficacy in the prevention of suicidal behavior. Also, the power analysis suggested that the antisuicidal effect size of the comparator drugs was sufficiently large to be detected with this design. Power analyses ensure that the risks of randomization are balanced by the likelihood of answering the scientific question. The inclusion of a placebo lead-in time was also rejected, since the subjects are enrolled while in highest-risk phases, while depressed or in a mixed state, and the scientific question was to be answered in the last phase of the study.
Psychosocial Interventions to Monitor for Exacerbation or Increased Risk
The study design includes the use of family-focused treatment
(22). The family-focused treatment emphasizes planning for relapse (“relapse drill”), provides family education about bipolar disorder, and addresses medication nonadherence. The use of relapse drills, formulated by research psychologists, with each subject’s family provides a format for including the subject’s support system in surveillance for clinical changes that might auger suicide risk. In addition, weekly family-focused treatment sessions include assessment of mood and suicidal ideation and behavior during the first 8 weeks of the study, when patients are in a depressed or mixed state and thus at increased risk.
Close Monitoring
After family-focused treatment phase is completed, the subject has semiweekly telephone appointments with the psychologist for clinical evaluation and monthly in-person appointments with the psychiatrist. If the psychologist notes a worsening in symptoms, the psychiatrist is contacted immediately for evaluation. Family and crisis interventions are then instituted. Also, patients and their families are instructed to call study staff in case of changes in symptoms or limiting side effects, and a research psychiatrist is available by pager around the clock. This high level of monitoring facilitates the implementation of rescue interventions, including, but not limited to, hospitalization in the case of acute suicide risk.
Subject Retention in the Event of a Hospitalization
Patients who require hospitalization are admitted to a general clinical research unit. Because the general clinical research unit and research clinic use the same research pharmacy, patients who are admitted continued to take the maintenance double-blind medication. The availability of inpatient phases of treatment allows for the assessment of the antisuicidal properties of the comparator medications in the face of mood instability and for the observation of subjects who have a suicidal event.
Early Detection of Large Effect Sizes
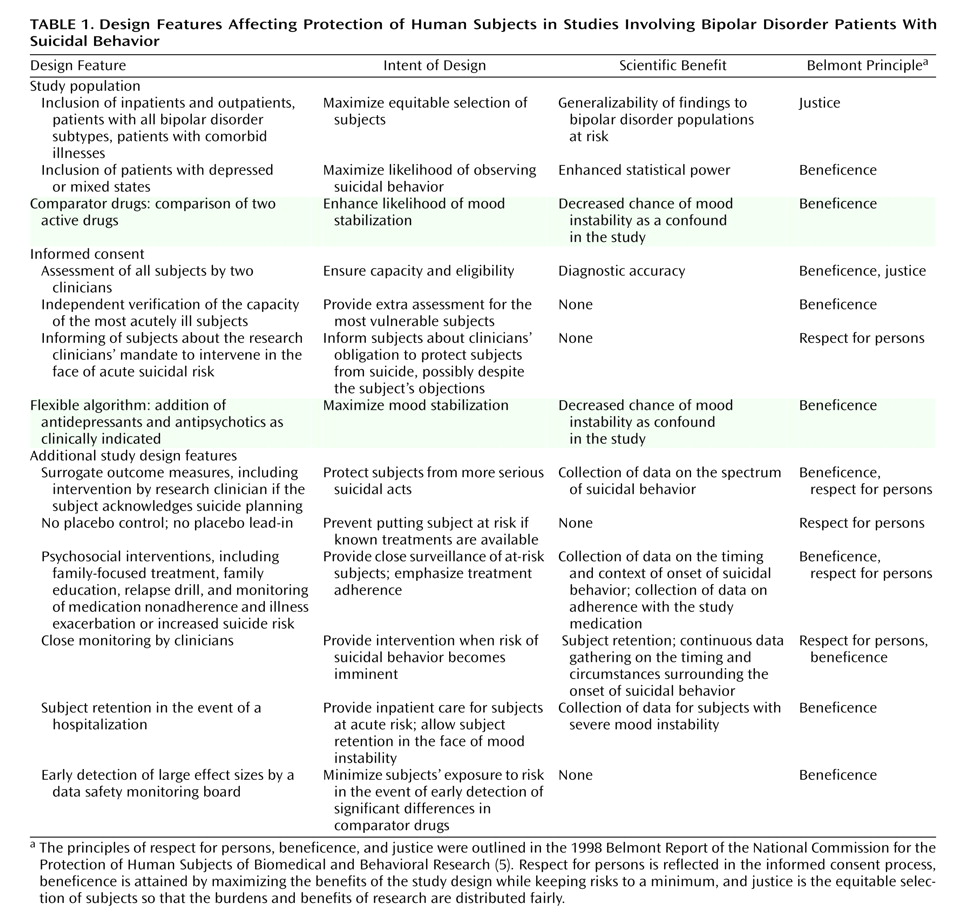
The independent data safety monitoring board established specifically to oversee this study monitors study progress and has established guidelines for the conduct of interim analyses and for early termination of the study. The board meets with the nontreating, unblinded research psychiatrist to review suicidal events in each of the treatment conditions. Thus, the data safety monitoring board can detect an early large effect of the drug on suicidal behavior and terminate the study, preventing unnecessary exposure to risk for the subjects. (See
Table 1 for a summary of the study design decisions and their effects on human protections and scientific considerations.)
Discussion
The design of a randomized, controlled trial that minimizes risk of morbidity and mortality for suicidal patients with bipolar disorder is possible, yet it requires deliberation to address the bioethical tensions that arise. Increasing both justice and beneficence by including subjects with comorbid conditions and severe illness enhances the generalizability of findings and has recently been advocated
(23). This approach results in equitable distribution of the burden of investigation as well as applicability of study results to a larger population. Nowhere is this more paramount than in the search for interventions for suicidal behavior.
Including only high-risk individuals also increases the benefits of the research to society. By enrolling only subjects with previous suicidal behavior, the study question is answered specifically for those most in need of effective interventions. In addition, increasing the base rate of the behavior of interest in the sample decreases the number of subjects required to answer the study question. However, this recruitment strategy still leaves a critical question unanswered: Are individuals with a given psychiatric condition who have shown suicidal behavior different in their clinical response to interventions than those without suicidal behavior?
Few published studies have addressed specific protections for subjects beyond noting that written informed consent was obtained and/or that the study was approved by a bioethics committee. A notable exception is the recent study by Meltzer et al.
(2), in which protections for the suicidal individuals enrolled in the trial are detailed. As more intervention research is conducted, the dissemination of information about strategies for protection of human subjects is likely to increase.
A long neglected benefit of clinical research participation relates to subjects’ perceptions of their reasons for enrollment. A study of schizophrenic subjects’ attitudes toward research participation found that patients endorsed participation as important for personal reasons, such as providing hope to the subject, and for altruistic reasons, including helping others, advancing science, and supporting schizophrenia research
(24). Thus, apart from benefiting society, studies may provide subtle yet measurable benefits to mentally ill subjects. The addition of exit interviews to identify altruistic reasons for participation in intervention studies may allow for future inclusion of these benefits into the risk-benefit analysis of the value of a study.
This article does not address the importance of assisting research staff in coping with the suicide of a subject. Clinicians’ reactions to negative outcomes and possible interventions to support clinicians who care for subjects with adverse outcomes have been described
(25). For studies of interventions for suicidal acts, a formalized system to deal with suicides has been recommended
(10).
Novel strategies for studying pharmacological interventions for subjects with bipolar disorder and for suicidal bipolar disorder subjects in particular are still lacking. Considering the parallels in treatment issues for bipolar disorder and epilepsy
(12,
26), approaches that have been utilized successfully in the identification of novel antiepileptic drugs may be of use. For example, “add-on” designs, in which the study treatment or placebo is added on to known effective treatment, eliminate the risks of placebo controls yet have resulted in measurable outcomes
(27). In addition, because bipolar illness is not typically treated with monotherapy, add-on designs reflect usual treatment patterns. These strategies may prove useful in studies of interventions for suicidal bipolar disorder patients as well.