Voting is a quintessential right of citizens in democratic societies. Although universal suffrage is now taken for granted in the United States, it has been less than a century since women were accorded the right to vote and barely more than a generation since that right was made meaningful for African Americans
(1). But some persons are still often denied the right to vote, including convicted felons and persons thought to be incompetent to cast a ballot
(2). For the latter group, the justification for exclusion is usually the state’s interest in protecting the integrity of the vote. How one might identify persons who lack the capacity to vote is the focus of this study.
In the United States, state laws generally govern election procedures. Most states have prescribed criteria by which people might be deemed incompetent to vote. Unfortunately, these criteria often focus on membership in a class (e.g., all persons under guardianship) rather than on an assessment of a person’s functional abilities
(3,
4). The states’ failure to require an individualized determination of capacity to vote has been challenged on the grounds that it deprives competent would-be voters of their constitutional right to vote
(5). A 2001 federal district court decision in Maine,
Doe v. Rowe, for the first time laid out the criteria that should be applied in individualized assessments of capacity to vote
(6).
The lawsuit in Doe was brought by three people with mental illness who objected to a provision in Maine’s constitution excluding all persons under guardianship for reasons of mental illness from casting ballots. Maine voters had twice rejected referenda that would have repealed the provision. But the federal district court ruled that the automatic exclusion of this class of persons violated their rights to procedural due process and equal protection and the guarantees against discrimination of the Americans With Disabilities Act. In striking down the offending provision of the Maine constitution, the court adopted a test proposed by the parties in the case: persons are considered incompetent to vote only if they “lack the capacity to understand the nature and effect of voting such that they cannot make an individual choice.” Although the case dealt with persons with mental illness, the criteria apply to all persons whose competence to vote may be in question. (We refer to these criteria hereafter as the “Doe voting capacity standard.”)
The move to individualized, functional determinations of the specific capacity to vote parallels similar trends with regard to assessments of the capacity to consent to treatment or research, complete an advance directive, manage finances, and make other important decisions
(7). In all these areas, efforts have been made to operationalize the relevant legal criteria in assessment instruments that can be applied in a reliable fashion. With regard to voting, such a process not only will help to limit the number of persons excluded from voting by the courts but will also permit election officials and caregivers to decide when a person has become incapable of voting. This is of particular importance for the growing number of persons with Alzheimer’s disease and other progressive cognitive disorders, many of whom now vote
(8,
9), since such a transition is almost inevitable in those disorders and many of them eventually reside in long-term care facilities, where federal regulations stipulate that the facility must respect the residents’ civil rights, including the right to vote
(10). Facility staff, however, are at present without practical guidance as to how to distinguish between residents who are capable and incapable of voting.
In this article, we report the results of a study that explored consequences of applying the criteria identified in the Doe case to persons with very mild to severe Alzheimer’s disease. We focus on the relationships of the Doe voting capacity standard and other measures of capacity to the severity of dementia. Our a priori hypotheses were that voting capacity would correlate inversely with dementia severity and that the criteria cited by the Doe court decision would prove less restrictive than alternative approaches.
Method
Subjects
Eligible subjects were community-dwelling persons (N=33) with very mild to severe Alzheimer’s disease (possible or probable) who attended an annual assessment as part of the longitudinal cohort followed at the Memory Disorders Clinic at the University of Pennsylvania. The diagnosis of Alzheimer’s disease was based on the criteria of the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association
(11), and dementia severity was defined by using standard cut points on the Mini-Mental State Examination (MMSE): very mild, >23; mild, 20 to 23; moderate, 12 to 19; and severe, <12
(12). Most subjects were white (85%); 12% were African American, and 3% were Asian. No subjects refused to participate, although four subjects who originally agreed did not complete the interview because of scheduling issues.
Development of Assessment Tool and Scoring Criteria
The instrument used to assess the capacity to vote, the Competence Assessment Tool for Voting (CAT-V), is based on the structure and scoring criteria of other capacity assessment instruments
(13,
14). It assesses a person’s performance on all four standard decision-making abilities: understanding, appreciation, reasoning, and choice
(15). Although only understanding and choice were required by the
Doe court, we added appreciation and reasoning questions for comparative purposes.
We designed the CAT-V understanding and choice questions on the basis of the standard for voting capacity described in the
Doe case
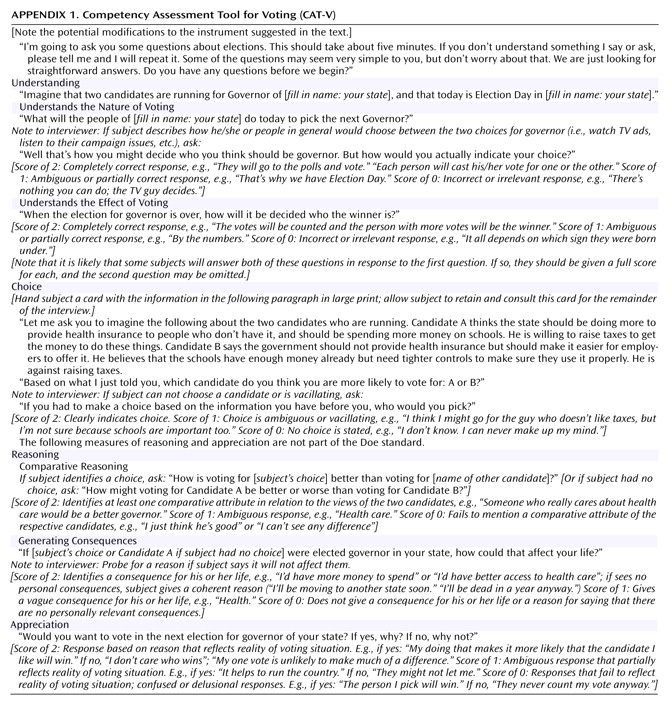
(6). As noted, that case held that a person has the capacity to vote if he or she understands the nature and effect of voting and has the capacity to make a choice. The CAT-V operationalizes these criteria into three questions based on the Doe standard (“Doe standard questions”), which are distinct from the remaining CAT-V questions.
Following an introduction that asks the subject to imagine that it is the day for election of the governor of the state, an interviewer inquires about the person’s understanding of the nature of voting and then asks a question to assess understanding of the effect of voting. Next the interviewer reads aloud a description of two candidates for governor, gives this written description to the person, and then asks the person to choose one of the candidates.
The CAT-V also includes three questions that go beyond the Doe voting capacity standard to assess the abilities to reason about the electoral choice by comparing the candidates and identifying the ways in which choosing one over the other could affect the subject’s own life. Subjects are queried about their appreciation of the significance of voting by being asked to explain why they would or would not want to vote in the next election for governor of their state.
For each CAT-V item, we developed scoring criteria using a 2, 1, or 0 scale where a score of 2 described adequate performance on the measure, 1 described marginal performance, and 0 described clearly inadequate performance. Drafts of the instrument and its scoring criteria were tested on a convenience sample of approximately 10 cognitively normal people (co-workers) and five persons with Alzheimer’s disease. A final version was then administered to consecutive persons with Alzheimer’s disease attending the Memory Disorders Clinic, with recruitment adjusted to approximate equal numbers across the severities of dementia. The instrument and its scoring criteria are shown in
Appendix 1.
Data Gathering
Each subject participated in a face-to-face interview with an investigator (J.H.K.). The interview was digitally recorded to allow two raters (P.S.A. and R.J.B.) to score the interviews independently. The raters (although not the interviewer) were blind to the subject’s MMSE score, age, and education. Periodically, the investigators reviewed their scoring to adjudicate cases of disagreement so as to arrive at a set of final scores that were used in the data analyses. The participants’ demographic data and MMSE scores were taken from the Memory Disorders Clinic database.
Data Analyses
We used a quadratically weighted kappa to assess the interrater reliability of the CAT-V scoring criteria prior to agreement on a consensus score. For each participant, we created a Doe score (range=0–6) by summing the scores on the two measures of understanding (range=0–4) and the measure of choice (range=0–2), created a reasoning score (range=0–4) by summing the subject’s scores on the two measures of reasoning, and assigned an appreciation score on the basis of the single item (range=0–2). Appropriate summary statistics and cross tabulations are used to display the nature of the participants’ performance. We used Fisher’s exact test to examine associations between CAT-V measures, and the Spearman correlation coefficient or the Kruskal-Wallis test was used to examine the associations of CAT-V performance with MMSE scores and the participants’ demographic characteristics.
Human Subjects Protections
Each participant was recruited by an initial contact with the person who accompanied the participant on visits to serve as a knowledgeable informant and decision maker for the person with Alzheimer’s disease, typically a spouse or adult child, referred to as the “caregiver.” If this person agreed to an interview, the person with Alzheimer’s disease provided either verbal informed consent or assent (in which case the caregiver provided verbal informed consent), after disclosure of the nature of the study. This project was approved by the University of Pennsylvania institutional review board. The subjects were assured that the information would be used only for research purposes, and none expressed concern about this issue.
Results
Subject Characteristics
Thirty-three persons with Alzheimer’s disease completed the interview. Sixteen (48%) were male. The mean age was 77.7 years (SD=7.1, range=59–87), and the mean number of years of education was 14.0 (SD=3.4, range=8–20). The mean MMSE score was 16.4 (SD=6.8, range=2–28). According to the standard MMSE cutoff points, the dementia was very mild for five subjects (15%), mild for eight (24%), moderate for 11 (33%), and severe for nine (27%).
Performance on CAT-V
The participants took an average of 3.6 minutes (SD=1.5, range=1.7–8.3) to complete the CAT-V understanding and choice items (i.e., the Doe standard questions) and 6.6 minutes (SD=2.6, range=2.9–14.2) to complete the entire interview. The scoring criteria showed good interrater reliability (prior to consensus reconciliation of differing scores) as measured by the kappa statistic: understanding nature of voting, 0.91; understanding effect of voting, 0.91; choice, 1.00; comparative reasoning, 0.77; consequential reasoning, 0.74; and appreciation, 0.87.
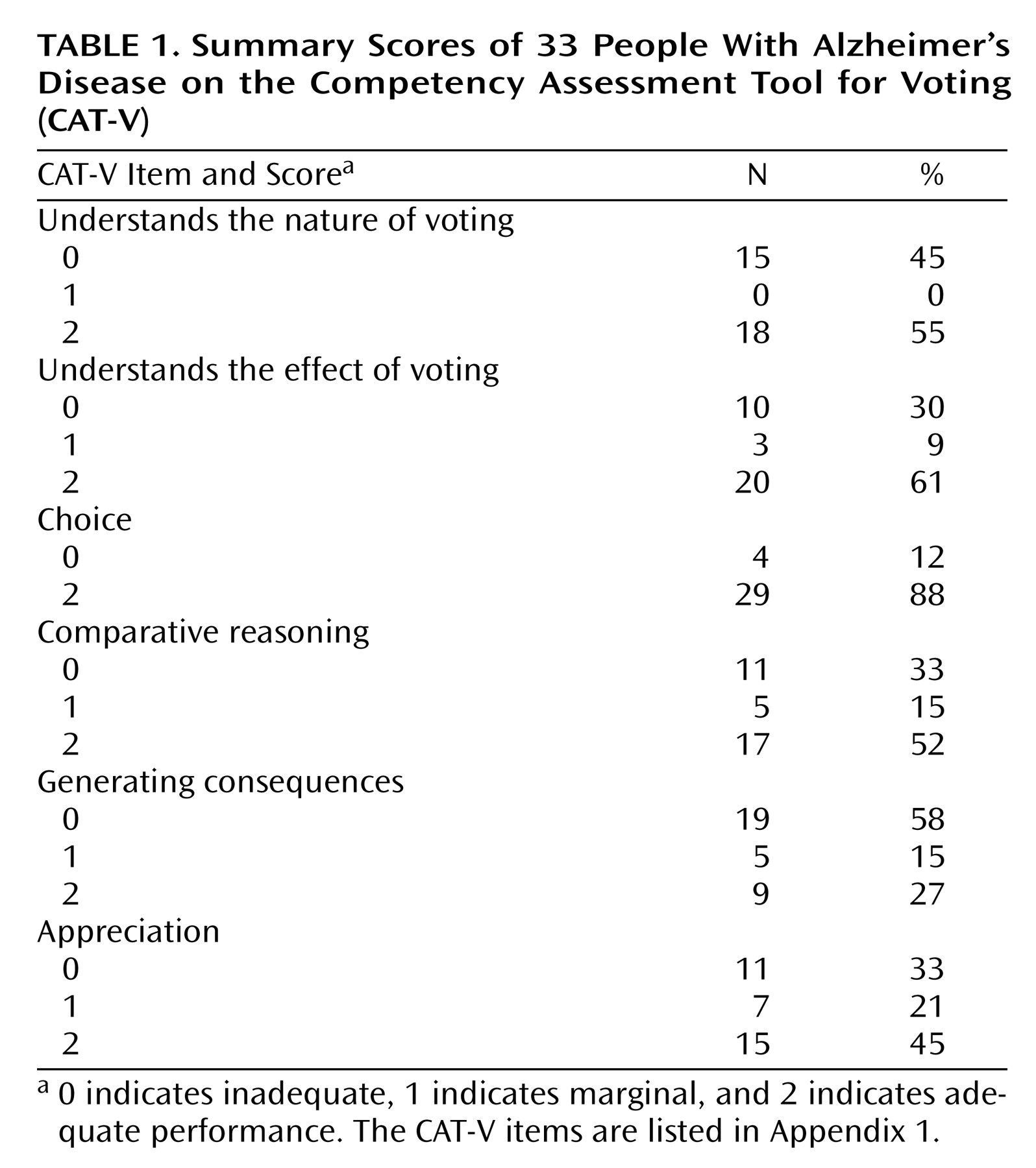
Table 1 shows the distributions of the participants’ scores on each of the CAT-V questions. Twenty-five participants wanted to vote in the next election for governor, and six did not (two participants could not answer the question). Subjects who scored a 0 on the choice item were older than those who scored a 2 (rank-sum test: z=2.3, p=0.02). None of the other CAT-V scores or the desire to vote was associated with either the subjects’ age or their years of education.
Scores on the understanding and choice items showed that subjects typically had either adequate or inadequate performance on these three measures, with marginal performance rare. No one scored 1 on understanding the nature of voting, and only three subjects scored 1 on understanding the effect of voting. The majority of subjects (N=29, 88%) could adequately make a choice. Of the four subjects who did not make a choice, all but one also scored 0 on both understanding items. Thus, only one subject scored a 2 on both understanding items while being unable to make a choice. This subject was undecided about which candidate to pick. Participants showed more variability in their abilities to reason about and appreciate the significance of voting. Between five and seven participants scored a 1 on these measures.
Performance on CAT-V Subscales
Cross-tabular comparisons of scores on the ability to understand the nature of voting to scores on the reasoning and appreciation measures showed that the subjects performed better on the ability to understand the nature of voting than on the abilities to reason about (Fisher’s exact test, p=0.001) and to appreciate the effect of (Fisher’s exact test, p=0.0001) voting. Similar results were found when we compared the scores on the ability to understand the effect of voting and scores on the abilities to reason (Fisher’s exact test, p=0.0001) and appreciate the significance of voting (Fisher’s exact test, p=0.0001).
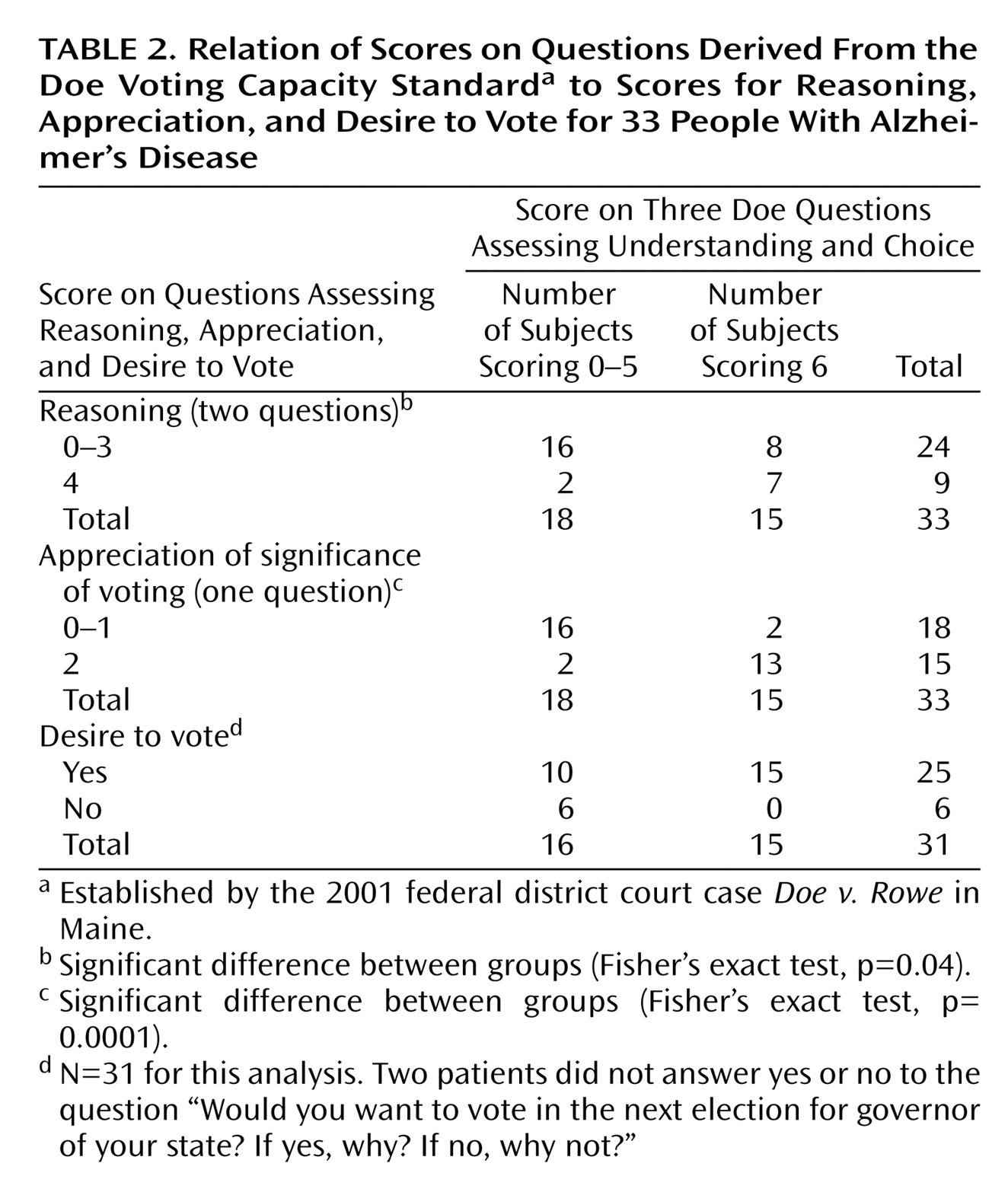
Table 2 shows cross-tabulations relating the subjects’ scores on the Doe standard questions to their scores on the measures of reasoning and appreciation and their desire to vote. The table suggests that persons whose score on the Doe questions was a 6, the maximum score, were more likely to have the maximum scores on reasoning and appreciation.
Every participant who scored 5 or 6 on the Doe questions indicated a desire to vote, but so did eight participants who scored less than 5, including four who scored 2 and two who scored 0. Looked at another way, eight of the 14 subjects who scored 4 or less (including two of the three with scores of 0) expressed a desire to vote.
Relationships Between CAT-V Performance and Dementia Severity
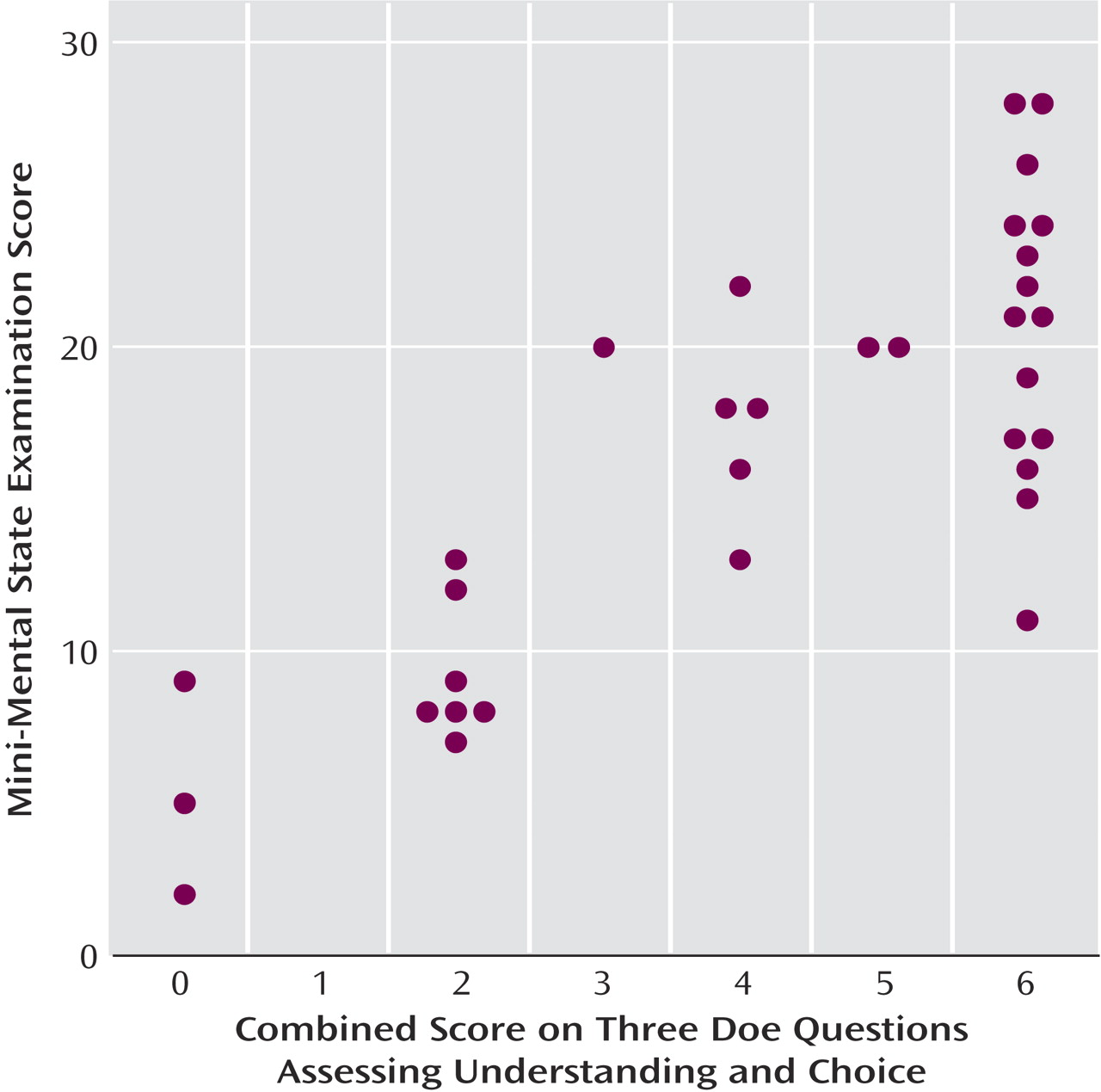
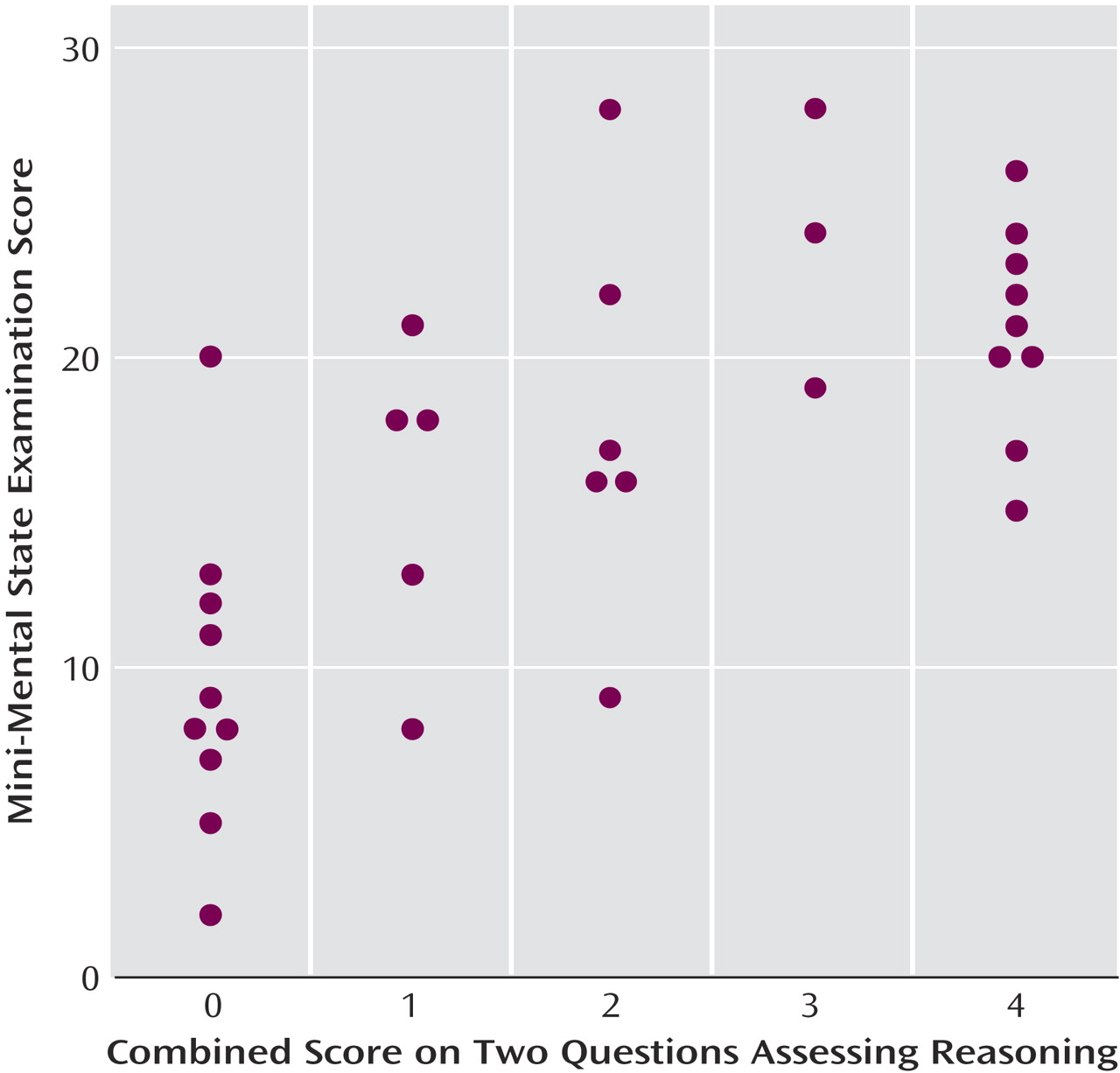
Figure 1 shows that higher scores on the Doe questions were associated with better performance on the MMSE (r
s=0.75, df=32, p<0.0001). Inspection of the graph shows that all persons with severe dementia (MMSE score <12) scored a 2 or lower on the Doe standard questions and that all persons with very mild and most with mild dementia scored a 6. In contrast, persons with moderate-stage dementia showed substantial variability in their scores on the Doe questions, ranging from 2 to 6.
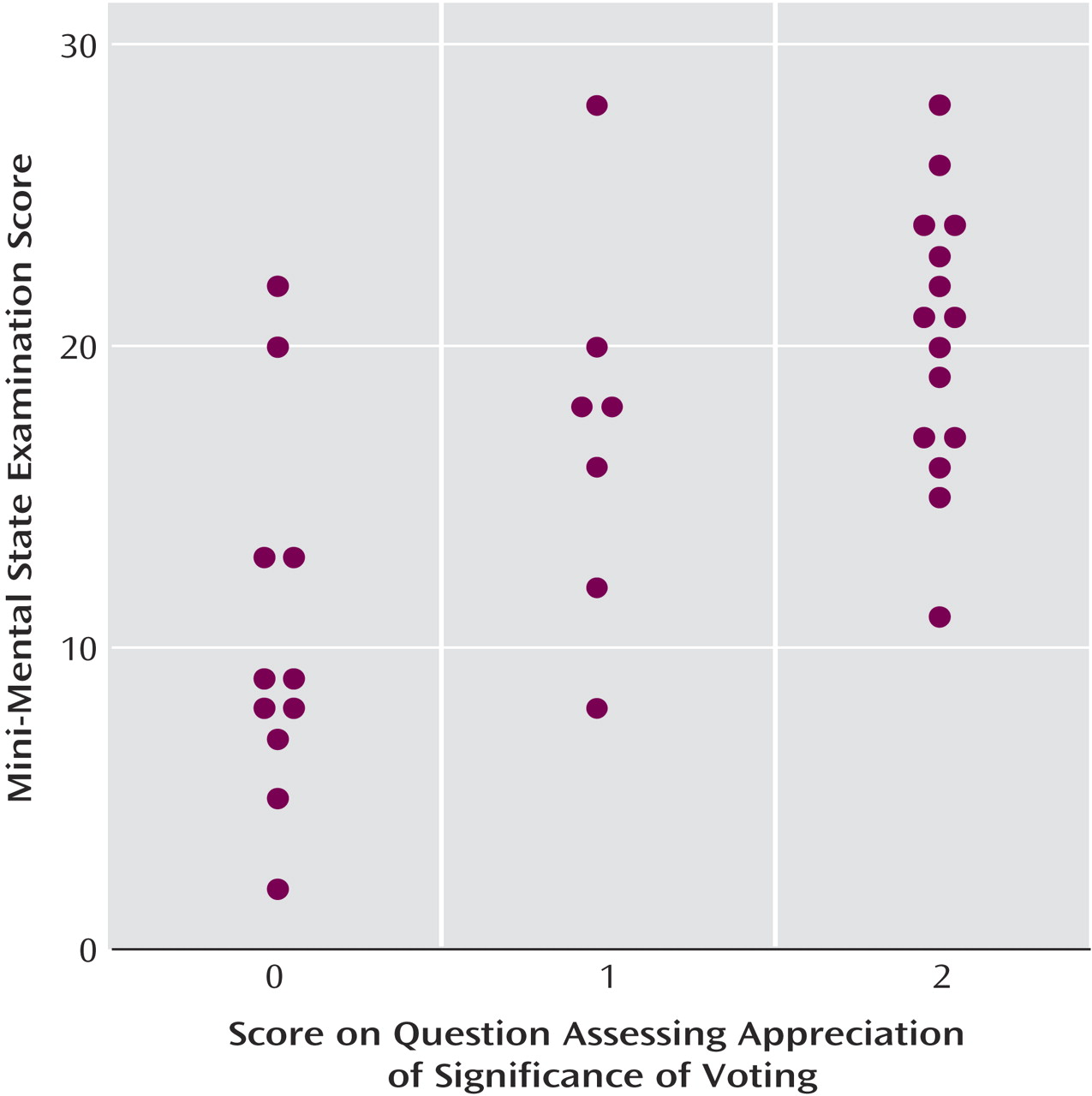
Figure 2 and
Figure 3 show associations between higher MMSE scores and better performance on the measures of reasoning (r
s=0.70, df=32, p<0.0001) and appreciation (Kruskal-Wallis test: χ
2=11.8, df=2, p=0.003). All subjects who scored the maximum of 4 on reasoning had an MMSE score of 15 or greater, and all who scored the maximum of 2 on appreciation had an MMSE score of 11 or greater. However, for both of these CAT-V measures, the figures show that some subjects whose MMSE scores were in the mild to moderate range had CAT-V scores less than either 4 on reasoning or 2 on appreciation.
The mean MMSE score of persons who did not want to vote was 13.0 (SD=7.2, range=2–20), and among those who wanted to vote it was 17.3 (SD=6.6, range=5–28). No relationship was found between the desire to vote and performance on the MMSE (rank-sum test: z=–1.3, p=0.20).
Discussion
Using a set of commonsense criteria for the capacity to vote that were elaborated by a federal court, this study demonstrates a strong correlation between dementia severity and the capacity to vote. The data exploring the relationship between the responses to the questions intended to operationalize the Doe voting capacity standard (understanding and choice) and the participants’ MMSE scores suggest that most (but not all) persons with very mild to mild dementia of the Alzheimer’s type retain adequate ability to vote and that most persons with severe dementia do not. The variability in scores on the Doe standard questions among persons with moderate dementia suggests the need for individualized assessments for these potential voters. In contrast to most types of capacity assessment, performance was independent of age and education, although the range of educational levels was compressed.
The Doe voting capacity standard, which emphasizes understanding of the nature and effect of voting and the ability to make a choice, reflects the tendency of American law to place few barriers in the way of citizens who desire to vote. For example, neither the ability to read nor knowledge of English is required of voters and probing a potential voter’s reasoning ability, understanding of the context in which the election is held, or understanding of the merits of any given ballot question would open the door to arbitrary (and possibly discriminatory) judgments reminiscent of the literacy tests used in the South to disenfranchise black voters until the middle of the 20th century
(1).
To allow a comparison of the Doe standard of competence with alternative approaches to determining decisional capacity, however, we also included in this study questions intended to address participants’ abilities to reason about and appreciate the significance of voting. Relationships between reasoning and appreciation scores and the MMSE score suggest that many persons with very mild to mild Alzheimer’s disease retain the abilities to reason and appreciate in the voting context. As expected, however, the data also confirm that a standard for voting capacity that measures the ability to reason or appreciate the significance of voting would likely disenfranchise some persons who retain the abilities to understand the nature and effect of voting and to make an electoral choice.
Because of concerns that the use of any test of voting capacity creates a risk of misuse and selective exclusion of persons who are in fact competent to vote, it is sometimes suggested that any person who expresses a desire to vote should be allowed to do so. It was clear from our data, however, that not all persons who say they want to vote understand the nature and effect of voting. Indeed, the majority of persons who scored 5 or below on the questions derived from the Doe voting capacity standard, including several who scored 0, expressed a desire to vote in the next election for governor of their state. In the absence of an objective criterion for judging capacity to vote, it seems likely that voters who do not understand what voting is may still cast ballots, potentially compromising the integrity of the electoral process.
The instrument we used to operationalize the Doe criteria was easy and efficient to administer. Only 3–4 minutes were required to ask the questions related to the Doe voting capacity standard. This suggests that those questions from the CAT-V or a similar interview could be used efficiently to screen persons whose voting capacity is in question. Since the appreciation and reasoning questions do not reflect judicially approved criteria, we do not recommend their use for this purpose. Given that the Doe questions are drawn directly from the court’s criteria, they appear to have face validity, and the correlation with severity of dementia suggests validity for the construct as well. Whether other courts and legislatures embrace the Doe court’s criteria (the decision was not appealed) remains to be seen.
On the basis of this relatively small study group, we are inclined to think that responses on the two understanding items can be objectively scored as adequate or inadequate, without any intermediate score. Further thought may need to be given to whether the item assessing the ability to choose (which functions clearly as a binary variable) is needed in the interview. Including this item would increase the time needed to administer the interview, and it could be argued that a person who is unable to make a choice will not be able to cast an effective ballot in any event. On the other hand, identifying such potential voters in advance may save the time and difficulties associated with getting them to the polls or attempting to assist them in completing absentee ballots. If the choice item is retained, the scoring should acknowledge that being undecided is a choice too.
Using a structured interview, such as the CAT-V, offers advantages over unstructured or clinical assessments. It focuses an assessor on the specific abilities needed for the capacity to vote and also may provide a basis for educating the person being evaluated so that he or she might acquire sufficient understanding to achieve capacity. What an instrument cannot do is determine which scores represent adequate capacity. The extremes of performance are not controversial: a 0 clearly indicates lack of ability and a 6 (or 4, depending on whether the ability to choose is necessary) on the Doe questions indicates adequate capacity. But intermediate scores require a judgment to be made, the basis of which at this point is not clear. Data on the performance of nondemented subjects may be helpful in identifying appropriate cutoffs.
These preliminary data also suggest that persons with severe Alzheimer’s disease as measured by the MMSE are likely not competent to vote and that persons with very mild to mild Alzheimer’s disease are likely competent to do so (although the latter may benefit from memory aids when casting their ballots). For persons with moderate Alzheimer’s disease, no presumption seems warranted one way or the other. For these individuals, a screening tool such as the relevant sections of the CAT-V may be useful for caregivers who are wondering whether they should try to encourage voting or assist with it. In the absence of a clear indication of incapacity, however, the fundamental nature of voting rights suggests that such a person should be regarded as eligible to cast a ballot. The use of MMSE cutoff points for persons with Alzheimer’s disease, of course, may not be material to assessments of persons with other causes of dementia.
The limitations of this study relate to the relatively modest number of subjects, who were not drawn randomly and may not be fully representative of persons with Alzheimer’s disease (e.g., the range of educational achievement was narrow). Additional research might examine performance on the CAT-V or similar interviews by persons with more diverse kinds of cognitive impairments and lesser degrees of education and literacy. This could assist in identifying groups at higher risk for voting incapacity and thus permit more targeted assessment of such persons. Closer study of the cognitive correlates of performance in persons with mild to moderate Alzheimer’s disease may be helpful in better characterizing the persons in that mixed group who are likely not to be competent voters. Comparisons of CAT-V scores with judgments of clinicians, caregivers, and others involved with Alzheimer’s disease patients would help to determine the unique contribution of a structured assessment of this sort.
With the growing number of elderly persons with dementia
(16), the high voting rates among elderly groups
(17), and the recent attention to variables that may affect close races, further refinement of approaches to identifying potential voters with inadequate capacity will become increasingly important to our electoral system.