The anxiolytic effects of training in aerobic exercise have been described in numerous studies in healthy volunteers
(1). In line with this, case reports
(2) and two clinical studies have suggested that exercise training may be used therapeutically in patients with anxiety neurosis
(3) and panic disorder
(4). In addition, studies in healthy subjects and two case reports
(5,
6) have suggested that an acute bout of exercise is anxiolytic as well. In contrast, exercise may induce acute panic attacks
(4,
7) or increase subjective anxiety in patients with panic disorder more than in other people
(8). To our knowledge, the potential acute antipanic activity of exercise has not been studied systematically.
Acute bouts of exercise have been shown to reduce symptoms induced by CO
2 and caffeine
(9,
10). However, CO
2 and caffeine primarily induce somatic symptoms of anxiety in healthy subjects but rarely panic attacks. In contrast, cholecystokinin tetrapeptide (CCK-4) dose dependently and reliably induces panic attacks in healthy comparison subjects
(11). Therefore, we studied the potential acute antipanic effects of aerobic exercise in healthy volunteers after CCK-4 administration and compared CCK-4-induced panic attacks with and without previous exercise.
Method
Fifteen healthy subjects (six women and nine men; mean age=26.4 years, SD=3.8) with no personal
(12) or family history of a psychiatric disorder were recruited for the study. The subjects did not take any medication and had undergone a thorough medical examination to rule out other illnesses, drug intake, and lifestyles (sleep deprivation, changes in the sleep-wake cycle) that could interfere with the study. The protocol was approved by the local ethics committee for human experiments. After a complete description of the study to the subjects, written informed consent was obtained. The subjects were paid for their participation. Before the experiment, a treadmill spiroergometry was performed to determine the subjects’ maximum oxygen consumption. Subjects were excluded if they were too physically fit (maximum oxygen consumption >55 ml/kg/min) or had signs of cardiovascular abnormalities during the ergometry. The subjects were told that the aim of study was to characterize the behavioral effects of exercise on CCK-4-induced symptoms.
All subjects were studied twice on different days separated by 1 week. From 9:30 a.m. to 12:00 noon, the subjects were studied in a supine position in a soundproof room with a single bed. On the first day, the subjects were randomly assigned to one of two conditions: quiet rest or exercise (treadmill walking for 30 minutes at 70% of maximum oxygen consumption from 10:20 to 10:50 a.m.); the other condition was used on the second study day. Each subject received a bolus injection of 50 g of CCK-4 (Clinalfa, Laufelfingen, Switzerland) dissolved in 2 ml of 0.9% saline solution at 11:00 a.m. The Acute Panic Inventory
(13) was administered at 10:00 a.m. (baseline), 10:55 a.m. (after rest or exercise), and 11:05 a.m. (after CCK-4 administration) by a rater blind to the procedure (A.S. or M.O.); the maximum intensity during the observation period was noted. To further characterize the possible effects of exercise, we used a previously described anxiety subscore (afraid of dying, general fear)
(14,
15) and a somatic subscore (palpitations, breathing, and nausea) of the Acute Panic Inventory. A panic attack was noted when the Acute Panic Inventory total score exceeded 20 and an increment of at least 14 points over the -10:00 score was observed
(13,
14,
16). The occurrence of a panic attack was confirmed by a trained psychiatrist. On the second study day, the subjects were additionally asked whether exercise reduced or increased CCK-4-induced symptoms or whether it had no influence at all.
The frequencies of panic attacks in the two treatment conditions were compared by using the McNemar paired chi-square test. The subjective experiences of whether exercise decreased, increased, or had no effect on CCK-4-induced symptoms were compared by using the chi-square test. For statistical comparison of mean Acute Panic Inventory scores and the subscores between the rest and the exercise conditions and among the three time points (10:00 a.m., 10:55 a.m., and 11:05 a.m.), a two-factor multivariate analysis of variance (MANOVA) with a repeated-measures design was performed. Treatment and time were the two within-subjects factors, with two or three levels. Hypothesis tests for the main and interaction effects of these factors were based on multivariate criteria, such as Wilks’s lambda and its approximated F value. When significant main or interaction effects were found, univariate F tests and/or tests with contrasts followed by MANOVA for investigating simple effects were performed. As a nominal level of significance, alpha=0.05 was accepted. To keep the type I error at ≤0.05, all post hoc tests (univariate F tests and tests with contrasts) were performed at a reduced level of significance (an adjusted alpha according to the Bonferroni procedure).
Results
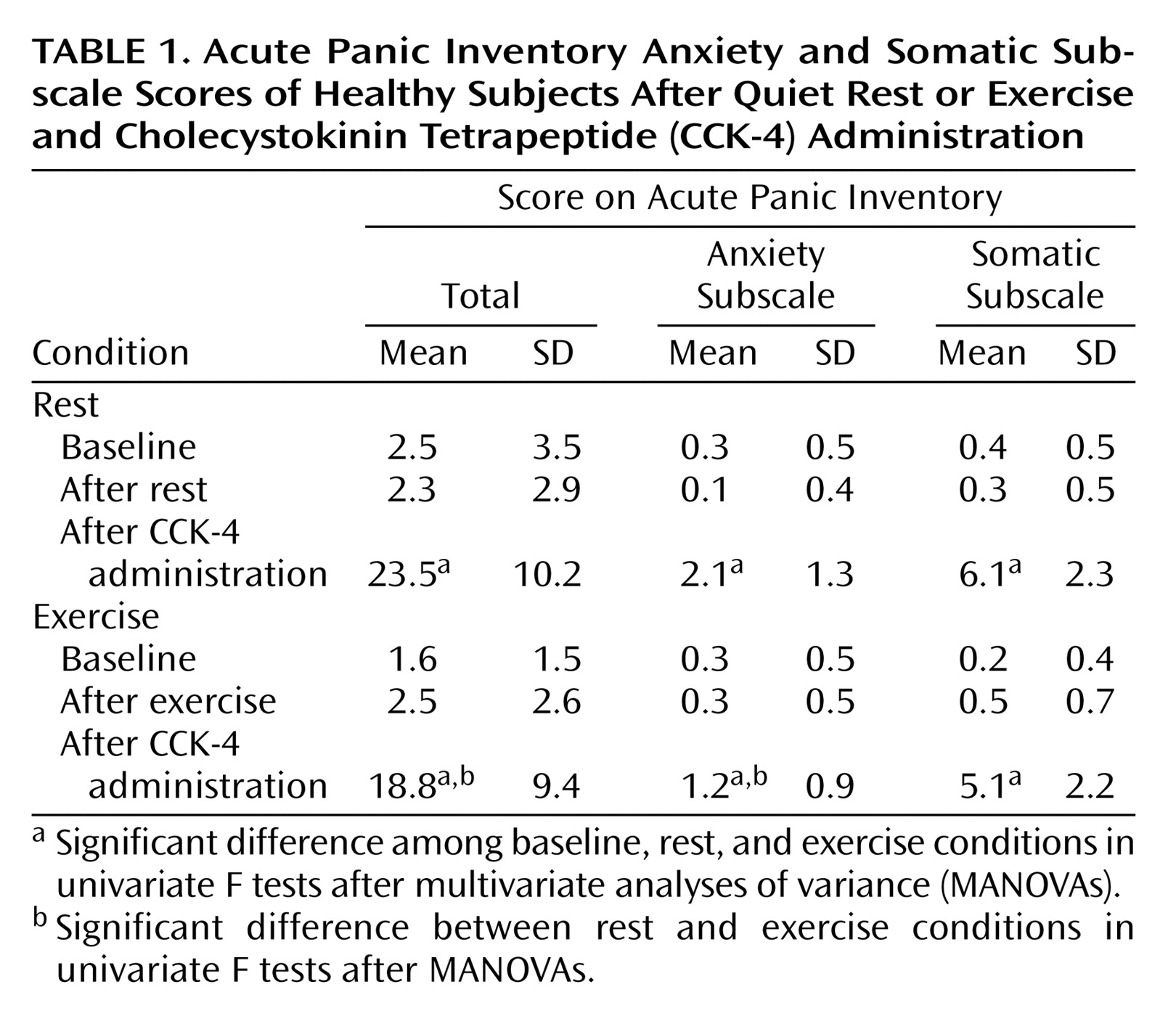
The rates of panic attacks were significantly higher in the quiet rest than in the exercise conditions (12 of 15 versus six of 15) (p=0.03, McNemar’s test) (
Table 1). Ten subjects estimated that exercise reduced CCK-4-induced symptoms, three did not experience a difference, and two subjects estimated that exercise increased CCK-4-induced symptoms (χ
2=7.60, df=2, p=0.02).
MANOVAs of the Acute Panic Inventory score and the subscores revealed significant main effects of time (F=15.60, df=6, 52, p=0.001) and a significant interaction effect of time by exercise (F=3.11, df=6, 52, p=0.01). Univariate F tests indicated that the interaction of time by exercise was significant for the overall Acute Panic Inventory score (F=6.73, df=2, 28, p=0.01) and the anxiety subscale score (F=8.67, df=2, 28, p=0.007) and nearly significant for the somatic symptoms subscore (F=3.04, df=2, 28, p=0.09). When analyzing the simple effects of time on the Acute Panic Inventory score and the anxiety subscales, i.e., the differences of the last variables between the three time points, we found that CCK-4 increased the Acute Panic Inventory score and the anxiety subscore score compared to baseline (tests with contrasts in MANOVA, p<0.05). Compared to quiet rest, exercise significantly reduced the CCK-4-induced increase in the total Acute Panic Inventory score and the anxiety subscore (tests with contrasts in MANOVA, p<0.05).
Discussion
The main finding of this exploratory study was that 30 minutes of aerobic exercise had an acute antipanic activity. In healthy volunteers, the frequency of panic attacks and CCK-4-induced symptoms was significantly decreased after exercise. Subscore analysis of the Acute Panic Inventory scores indicated that exercise decreased CCK-4-induced anxiety symptoms rather than somatic symptoms. Additionally, the subjective experience of CCK-4-induced symptoms was decreased after exercise in most subjects.
Exercise has been shown to reduce somatic symptoms of anxiety induced by CO
2 (9) and caffeine
(10) in healthy volunteers. Our results for the first time suggest that exercise has an acute antipanic activity. Although it has already been demonstrated that exercise training for 10 weeks is anxiolytic in patients with panic disorder
(4), our results suggest that acute exercise may have antipanic effects. If these effects are confirmed in patients with panic disorder, acute exercise may be used in the treatment of panic disorder as well. The optimum intensity and duration of acute exercise in achieving immediate antipanic effects will then have to be characterized in patients with panic disorder after prior exercise testing.
Numerous psychological and physiological mechanisms have been suggested to explain the beneficial effects of exercise on anxiety and depression (for a review, see reference
17). Experimental evidence suggests that the effects of exercise are on the synthesis and metabolism of monoamines. In addition, activation of β-endorphin secretion has been linked to the behavioral effects of exercise. The hypothalamic pituitary adrenocortical system
(18) and its modulators—for example, atrial natriuretic peptide
(16)—may be further involved in the antipanic effects of exercise.
In summary, our findings give evidence for an acute antipanic activity of exercise. If confirmed in patients, our results suggest that acute exercise may be used in the treatment of panic disorder as well. However, details about the optimum dosage (duration and intensity) remain to be characterized in patients.