The Middle East is the scene of persistent military violence, human rights abuses, and subsequent family tragedies. However, few local epidemiological data are available on the prevalence of traumatic events, mental health symptoms, and acute responses to trauma. This study focuses on gender-specific trauma exposure, mental health, and peritraumatic dissociation among Palestinians living in the Gaza Strip.
Studies of the general population in North America show that both genders are exposed to multiple traumas but of a different nature: men to direct threats and military and civilian violence and women to indirect, sexual, and domestic violence
(1–
4). Although women are exposed to less severe direct trauma, they show more posttraumatic stress disorder (PTSD) than men do
(5–
7). For instance, a prospective study of 2,181 participants in the Detroit metropolitan area showed that among 18–45-year-olds, the prevalence of DSM-IV PTSD was 13% among the women and 6.2% among the men
(1). Women also suffer more often from chronic PTSD
(8). Results on gender differences are not, however, unanimous. Some studies have shown higher PTSD rates among men than women, especially in veteran samples
(9,
10). Kulka et al.
(9) found a PTSD prevalence of 15% among male and 8.5% among female American Vietnam veterans. The result can be explained by direct exposure to combat experiences, which made men more vulnerable. Also, only few gender differences have been found in the context of natural disasters
(11,
12). Gender differences in PTSD may thus be trauma specific, and unique social and biological underlying mechanisms may explain their variation. This study focuses on one potential explanation for the greater female susceptibility to trauma-related symptoms in a community setting: peritraumatic dissociation.
The way people respond during acute exposure to trauma is crucial in explaining whether they recover or develop mental health symptoms. It is generally agreed that showing dissociation, i.e., losing sense of time, behaving mechanically (“like a machine”), or feeling like a bystander watching events occur is a risk for PTSD. Shalev and his team
(13–
15) in their prospective studies confirmed that peritraumatic dissociation predicts PTSD among accident victims. Positive associations between peritraumatic dissociation and PTSD have also been found in retrospective study settings among war veterans
(16–
19), disaster and accident survivors
(20–
22), and emergency workers
(23).
It is not yet fully understood why dissociation constitutes a risk for posttraumatic symptoms and what function it serves. One may suggest that, analogously with abnormal startle responses
(24–
26), dissociative states may serve a survival purpose at some level. Peritraumatic dissociation can be beneficial in the short run because it enables victims to dissociate themselves from overwhelming feelings of fear, horror, and revulsion
(27). On the other hand, peritraumatic dissociation may prolong physiological and neurobiological stress reactions and subsequently sensitize victims and increase susceptibility to disorders. However, there is no systematic research available on the risk versus protective functions of peritraumatic dissociation. Only one study could be found suggesting that peritraumatic dissociation may moderate the negative mental health consequences of military combat
(28).
Research shows no gender differences in the level of peritraumatic dissociation during traumatic events
(17,
19,
23). However, no research is available on the gender-specific mental health role of peritraumatic dissociation. Women and men show unique ways of responding to danger and expressing distress
(29), and therefore, we may expect gender differences in peritraumatic dissociation moderating the association between trauma exposure and mental health symptoms.
In this article, we study exposure to trauma, mental health symptoms, and the moderating role of peritraumatic dissociation in a Palestinian community sample. We formulated three gender-specific hypotheses: first, that men report higher frequencies of traumatic events in conditions of military violence; second, that we expect higher levels of psychiatric disorders among traumatized women than among traumatized men; and third, that we expect equal levels of peritraumatic dissociation between both genders. Furthermore, we explored whether peritraumatic dissociation moderates the impact of traumatic events on posttraumatic, depressive, somatic, and hostility symptoms in the same ways in men and women. The moderating effect of peritraumatic dissociation may either protect mental health from the negative impact of trauma or make people more vulnerable to mental health problems.
Method
Sampling and Procedure
The sample consisted of 585 subjects. The mean age was 31.6 years (SD=11.6), and the age ranged between 16 and 60 years. Fifty-three percent of the respondents (N=311) were female, and 47% of them (N=274) were male. A multistage sampling procedure, combining both nonprobability (selecting representative communities) and probability (selecting random households within the selected community), was used. This ensured a representative sample of the heterogeneous population in Gaza. The cities, refugee camps, and resettled areas were randomly chosen. Out of eight refugee camps, three were randomly selected. All three cities were selected. Of the five resettlement areas, two were selected that had heterogeneous populations.
The neighborhoods in each selected area were randomly assigned. The interviewers used random-direction number lists to choose the direction of the movement, starting from mosques and crossroads. Another random-number list was used to select the third house in that direction. The mosques were chosen because they are the most common and obvious landmarks and are equally distributed all over the populated areas. When there was more than one mosque in a neighborhood, they were all taken as starting points, and the number of subjects to be interviewed was divided among them.
The participants were interviewed in their homes by trained interviewers. The interviewers (N=8) used another random-number list to select one subject from the household who fulfilled the sample criteria. One member from each household who fulfilled the age criterion (16–60 years) was interviewed. The criterion for exclusion was severe cognitive impairment or severe psychosis. Verbal consent was obtained because the suspicion caused by the harsh sociopolitical situation in Gaza made signed consent almost impossible. For the same reason, the participants responded anonymously. If the subject was not available at the time of the first visit, a message was left, and two more contact attempts were made. Dropouts were 15 people (2.5%) from the original sample (N=600); five declined to participate, and 10 could not be interviewed because of illness or absence. All of these were young men. The data were collected in July to October 1997.
Measures
Traumatic events were evaluated by an adapted version of the Life Events and Social History Questionnaire
(30). The 13-item version consists, first, of family-related traumatic events, such as death or separation in the family, youth domestic events, and general life events, and second, of traumatic events that people typically face in military and political conflicts (e.g., witnessing killing and being the target of injury, shelling, and imprisonment). The participants were asked whether they had been exposed to each event (0=no, 1=yes) either in childhood (<12 years) or later in adulthood (>12 years). The total score of lifetime trauma ranged between 0 and 26 and had an average of 2.79 (SD=3.49). A dichotomous score was also constructed by giving the value 0 to those with no traumatic experiences (N=213) and 1 to those with one or more traumatic experiences (N=372).
Peritraumatic dissociation was assessed with the revised Peritraumatic Dissociative Experiences Questionnaire
(31). This is an eight-item questionnaire for assessing retrospective reports of depersonalization, derealization, out-of-body experiences, and altered time perception during a traumatic event. Two items stressed in the literature
(32) were added: 1) difficulty in making sense of what was happening and 2) feeling disoriented. The participants were asked to remember the worst, most distressing traumatic event and then to report whether they had (rating=1) or had not (rating=0) experienced described dissociations during that event. Internal consistency has been found to be good among Vietnam veterans
(17). Cronbach’s alpha in this sample was 0.94. We used the method described by Tichenor et al.
(19) to calculate the total score for peritraumatic dissociation.
PTSD was evaluated in relation to experienced adverse events from the aforementioned life events interview. The PTSD section of the World Health Organization Composite International Diagnostic Interview 2.1
(33) was used to assess lifetime PTSD according to DSM-IV criteria. Although the Composite International Diagnostic Interview/DSM-IV PTSD diagnosis has not been validated in a general population sample, good agreement between the Composite International Diagnostic Interview and independent clinical reinterviews has been found
(34). Other Composite International Diagnostic Interview sections were used to assess mood disorder, somatoform disorder, and (“other”) anxiety disorder. In our analyses, mood disorder covers DSM-IV dysthymia and major depressive disorder. Somatoform disorder contains DSM-IV somatization disorder, conversion disorder, hypochondriasis, and pain disorder. (“Other”) anxiety disorder encompasses DSM-IV panic disorder with or without agoraphobia, agoraphobia without history of panic disorder, social phobia, and specific phobia. We used two measures for the disorders: a total score that refers to the number of symptoms of the disorder and a variable that refers to the presence of the DSM-IV lifetime diagnosis of the disorder. A score for symptoms of hostility was derived from the Revised SCL-90-R Symptoms Checklist
(35).
Instruments were translated focusing on content, criterion, technical, conceptual, and semantic equivalence. The process of translation and adaptation involved 1) examination of the instruments by bilingual experts (Arabic and Dutch), 2) translation into Arabic, 3) literal back-translation by different translators, 4) examination of the back-translation by monolingual experts, 5) back-translation of all items changed by the monolingual experts, 6) examination of the back-translation by a bilingual group informed by the discussion of the monolingual experts, and 7) pilot testing
(36).
Statistical Analysis
We used chi-square analysis and Student’s t test to examine univariate differences in psychiatric disorders and sociodemographic variables between the men and women and chi-square analysis to test the hypothesis on gendered associations between trauma and psychiatric disorders. We report two-tailed test values, and we present Yates-corrected chi-square values for all two-by-two tables. Values for Student’s t tests are reported according to the results of testing the equality of variance assumption.
We assessed the following possible factors associated with different indicators of psychiatric disorders: lifetime traumatic events, peritraumatic dissociation, refugee status, family history of mental illness, and age. Main effects of factors on indicators of psychiatric disorders and moderator effects were identified by the following steps in hierarchical multiple regression analyses. First, we created the interaction term of the factors for lifetime traumatic events and peritraumatic dissociation. Next, we used hierarchical multiple regression analyses to estimate, as the first and second steps, the main effects of the lifetime traumatic events and peritraumatic dissociation on mental health symptoms. In the third step, we estimated the effect of the interaction term. A moderator effect was found when the estimate of the interaction term was significant
(37,
38). In the fourth step, we estimated the main effects of the other factors on mental health symptoms. For all analyses, we centered the data to prevent possible multicollinearity between the factors. Standardized variables (z scores) and interaction terms (computed from the z scores of the factors) were entered in the regression analyses.
Results
Demographic Factors
The women and men did not differ in age, marital status, number of children, refugee status, place of residency, and family history of mental illness (all comparisons between women and men on these variables had p>0.05). The men estimated their socioeconomic status to be better than that of the women (χ2=83.89, df=1, p<0.0001). Almost two-thirds (62%) of the men and 24% of the women reported their socioeconomic status to be above average, whereas 37% of the men and 74% of the women reported average socioeconomic status. The number of participants estimating their socioeconomic status as below average was small (1.5% of the men and 2% of the women). More women (8%) had not attended school than men (3%) (χ2=9.87, df=1, p<0.002). However, gender did not affect literacy (90% of the total sample was literate).
Gender, Trauma, and Mental Health
The results show that the lifetime prevalence of traumatic events was higher among the men (mean=4.68, SD=3.92) than the women (mean=1.13, SD=1.85) (t=13.70, df=378.79, p<0.0001; no equal variances were assumed). Eighty-six percent of the men (N=235) and 44% (N=137) of the women had experienced at least one traumatic event during their lifetimes (χ2=29.72, df=1, p<0.0001).
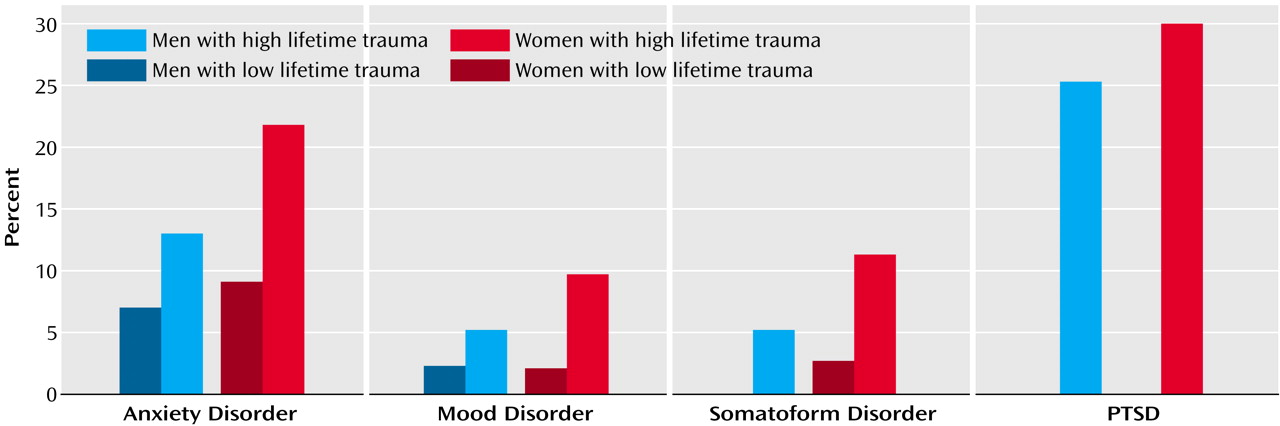
Figure 1 presents the results of gender-specific associations between exposure to lifetime trauma and mental health. They substantiate the hypothesis that when traumatized, women show higher levels of psychiatric distress than men, except for PTSD. Exposure to lifetime trauma was associated with anxiety disorder among women (χ
2=9.85, df=1, p<0.002) but not among men (χ
2=1.24, df=1, n.s.) and with mood disorder among women (χ
2=8.68, df=1, p<0.003) but not among men (χ
2=0.66, df=1, n.s.). The significant association was found between trauma and somatoform disorder among the women (χ
2=9.65, df=1, p<0.002) but not among men (χ
2=0.13, df=1, n.s.).
The association between lifetime trauma and PTSD did not differ between genders. Thirty percent of the women and 25% of the men who had experienced lifetime trauma had also been diagnosed with PTSD (χ2=1.62, df=1, n.s.). This indicates that although the men generally had a higher level of PTSD (24%) than the women (16%), the gender differences diminished when exposure to lifetime trauma was taken into account.
The Moderating Role of Peritraumatic Dissociation
We found no difference between women (mean 2.94, SD=1.21) and men (mean 2.73, SD=1.25) in the total score for peritraumatic dissociation (t=–1.57, df=583, n.s.).
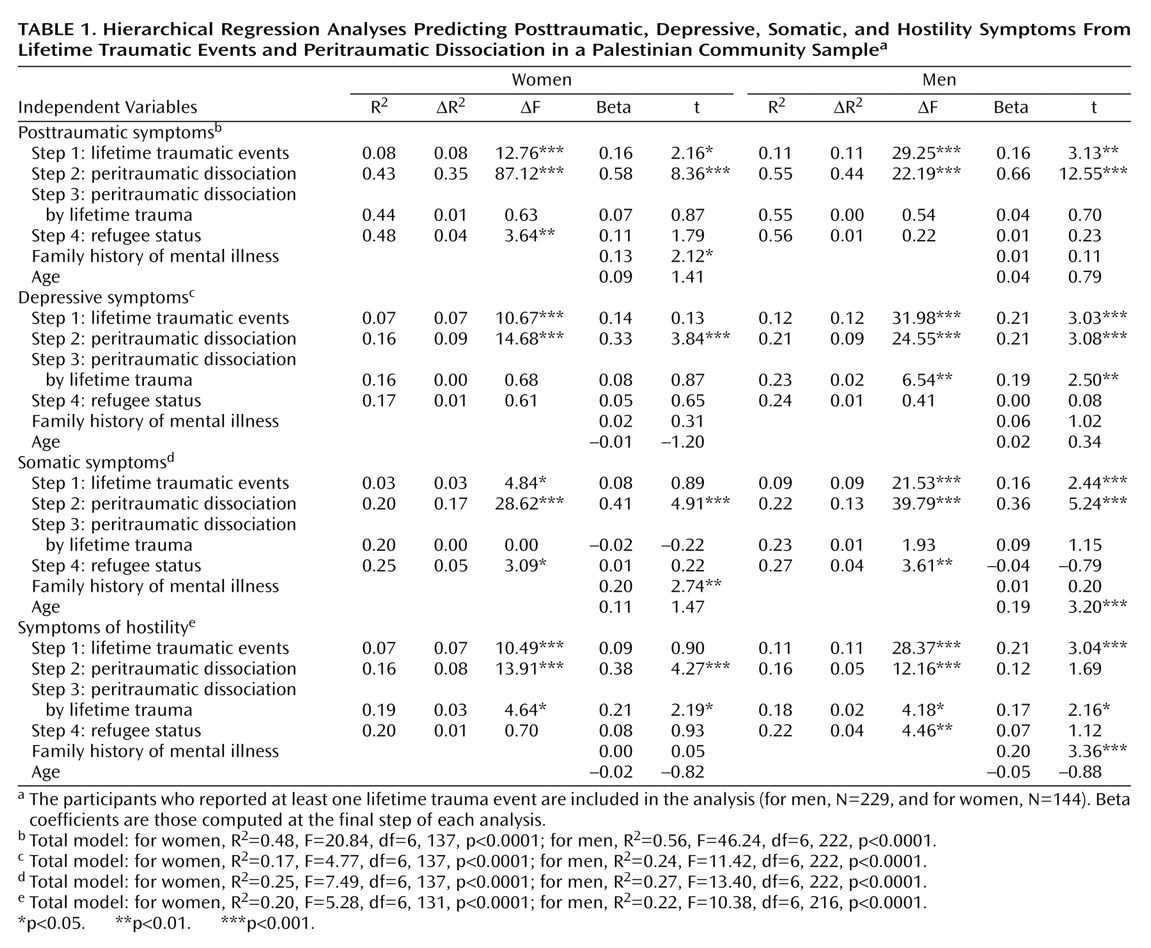
Table 1 shows the hierarchical multiple regression analyses, main and interaction effects of lifetime trauma and peritraumatic dissociation and demographic variables on mental health symptoms among women and men. The results revealed significant trauma-by-dissociation interaction effects (step 3) on depressive symptoms among men and on hostility symptoms among both genders. The positive moderating effects indicate that trauma was relatively less associated with these symptoms if the persons reported low levels of peritraumatic dissociation during the most severe trauma.
The hierarchical multiple regression analyses accounted for 48% of the variance in the women’s and 56% in the men’s posttraumatic symptoms. Peritraumatic dissociation did not have any moderating (either protective or risk) effect on posttraumatic symptoms, as the absence of significant interaction effects indicates. In both genders, lifetime trauma and peritraumatic dissociation were associated with high levels of posttraumatic symptoms (main effects). Among the women, having a history of mental illness in the family was further associated with posttraumatic symptoms.
The hierarchical multiple regression analyses accounted for 17% of the variance in the women’s and 24% in the men’s depressive symptoms. The models for depressive symptoms differed among the men and the women. Among women, only peritraumatic dissociation accounted for depressive symptoms: high dissociation was associated with a high level of depressive symptoms. Among men, there were significant main and interaction effects of both lifetime trauma and peritraumatic dissociation. These results indicated that exposure to lifetime trauma was relatively more associated with depressive symptoms, especially if the men had shown peritraumatic dissociation.
The hierarchical multiple regression analyses accounted for 25% of the variance of the women’s and 27% of the variance of the men’s somatic symptoms. Peritraumatic dissociation did not have any moderating (risk or protective) effect on somatic symptoms, as the absence of interaction effects indicated. Among the women, those who had shown peritraumatic dissociation and had mental illness in their family reported the highest level of somatic symptoms. Among the men, lifetime trauma, peritraumatic dissociation, and age predicted the level of somatic symptoms, i.e., the older men with high levels of lifetime trauma and peritraumatic dissociation reported the highest level of somatic symptoms.
Finally, the regression models of hostility accounted for 20% of the variance in the women’s and 22% in the men’s hostility symptoms. In both genders, the significant positive lifetime trauma-by-peritraumatic dissociation interaction effects indicated that lifetime trauma was relatively more associated with symptoms of hostility if the participants had shown peritraumatic dissociation. Among the women, peritraumatic dissociation had also a main effect on symptoms of hostility, and among the men, lifetime traumatic events and family mental illness were associated with a high level of hostility symptoms.
Discussion
Contemporary trauma research has focused on the complex moderating factors between exposure and psychopathology. Our study contributes to this by examining gender-specific trauma exposure and mental health consequences and the moderating role of peritraumatic responses in a Palestinian community sample.
Our results confirmed a higher lifetime prevalence of exposure to trauma in men than in women living in conditions of military violence. However, women were more vulnerable than men, as indicated by only women suffering from anxiety, mood, and somatoform disorders when traumatized. No gender differences were found in the association between lifetime trauma and PTSD diagnosis. Thus, our results show more similarities than differences between the conflict-ridden Middle East and more peaceful societies regarding the gender-specificity of exposure to trauma and female vulnerability to psychiatric disorders.
As hypothesized, we found no gender differences in peritraumatic dissociation during the most severe trauma. Peritraumatic dissociation was positively associated with posttraumatic symptoms, which concurs with earlier research
(15,
19,
20). We additionally showed that peritraumatic dissociation was also associated with depressive and somatic symptoms among both men and women and with symptoms of hostility among women. Shalev and Yehuda
(28) reminded us that PTSD is no longer considered a unique consequence of trauma. Research confirms that depression and somatic disorders are common among female rape
(39) and male torture
(40) victims. Likewise, we suggest that PTSD may not be the unique consequence of peritraumatic dissociation, and future studies should conceptualize a wide range of peritrauma-related symptoms.
We examined whether peritraumatic dissociation functions as a moderating factor (risk or protective) among trauma victims. The results revealed only a negative function of peritraumatic dissociation among both men and women. Lifetime trauma was associated with a relatively higher level of hostility if persons reported a high level of peritraumatic dissociation during the most severe trauma. The findings do not explain the greater female vulnerability to trauma-related symptoms because peritraumatic dissociation amplified the negative effect of trauma exposure in both genders. In fact, dissociation made men even more vulnerable because they also showed relatively more depressive symptoms when exposed to a high level of lifetime trauma.
Middle Eastern culture and politics constitute a special context for female and male vulnerability. Male heroism and sacrifice were highly appreciated during the Palestinian Intifada, as in any struggle for independence
(41). This may explain that the peritraumatic dissociation formed a risk for depressive symptoms among traumatized men. Dissociative responses apparently connoted loss of control, shame, weakness, and subsequent low self-esteem, all promoting depressiveness. Women’s dissociative and uncontrollable responses in a trauma scene are more easily accepted, especially in a culture that encourages strong and visual female emotional expression, for example, at funerals and other good-byes. The gender-specific roles of peritraumatic symptoms compel us to consider the symbolic, cultural, and social meanings of trauma and the ideological norms shaping people’s responses
(29,
41).
We applied a geographical random-sampling method, which is not without problems. The sample excluded individuals who were residing in institutions such as hospitals and prisons. The population density in Gaza is one of the highest in the world, and the population is evenly distributed in refugee camps and towns but not in resettled areas
(42). The choice of the mosque as a locator point for sample collecting was based on the consideration that neither population density nor social status differs according to mosque location in Gaza.
There is ample evidence that trauma victims tend to distort, narrow, and repress their memories of painful and often shameful scenes
(26). Subsequently, our research deserves criticism for using single-source information and relying on retrospective reporting. The research setting could be strengthened by applying observation methods for peritraumatic dissociation during traumatic events and archiving material regarding exposure to lifetime trauma.