An estimated 500,000–2,000,000 tablets of 3,4-methylenedioxymethamphetamine (MDMA, or Ecstasy) are taken recreationally each week in England
(1). MDMA binds to the serotonin transporter (5-HTT), preventing reuptake and stimulating release of serotonin (5-HT), and causes long-term changes to the 5-HT system in rats, nonhuman primates, and humans
(2–
4). In view of the critical role of 5-HT in the regulation of mood and the importance of selective serotonin reuptake inhibitors (SSRIs) in the treatment of major depression, it has been suggested that Ecstasy users may be at greater risk for developing affective disturbance following chronic use
(5). However, the long-term psychiatric consequences of Ecstasy use are highly controversial
(6).
The gene coding for the 5-HTT contains a functional polymorphism in the promoter region, a 44-base-pair insertion/deletion approximately 1 kilobase upstream of the transcription initiator site, designated the 5-HTT gene-linked polymorphic region (5-HTTLPR). This polymorphism produces two alleles, designated
l (“long”) and
s (“short”), respectively
(7). Cells with the
l allele have been shown to express more 5-HTT than cells with the
s allele, and, concordant with this, reuptake of 5-HT in human lymphoblastoid cells homozygous for the
l allele has been shown to be approximately twice that of cells either heterozygous or homozygous for the
s allele
(7).
We investigated Beck Depression Inventory scores and performance on the Affective Go/No-Go test, which is sensitive to emotional processing, in Ecstasy users and comparison subjects. We stratified individuals by 5-HTTLPR genotype, since the 5-HTT is the primary site of action for MDMA and individuals with the
s allele are at greater risk for affective disorders
(8) and also show poor response to antidepressant treatment with SSRIs
(9). We hypothesized that the 5-HTTLPR
s allele would confer particular risk for emotionally related cognitive disturbance following Ecstasy use because this allele is associated with lower 5-HTT expression
(8) and because experimental animal models of Ecstasy use show increased anxiety and decreased 5-HTT levels
(2).
Method
Sixty-six Ecstasy users (48 men, mean age=24.2 years, SD=6.6, mean IQ=112, SD=6.9), 30 cannabis users (15 men, mean age=25.7, SD=8.9, mean IQ=112, SD=8.8) and 28 healthy volunteers with no history of illicit drug use (15 men, mean age=24.0, SD=3.7, mean IQ=114, SD=5.4) were recruited by advertisement from the community. The Ecstasy users had to have used Ecstasy on at least 30 separate occasions and were required to abstain from use for at least 3 weeks before testing. Neither the cannabis users nor the healthy comparison subjects had used Ecstasy. Premorbid IQ was estimated by using the National Adult Reading Test
(10). In addition, a 10-ml blood sample was taken, and all participants filled out a structured substance use questionnaire and the Adult Impulsiveness, Venturesomeness and Empathy Scale
(11), a widely used 54-item personality questionnaire producing three orthogonal constructs that relate in a factor analysis to impulsiveness (self-control), venturesomeness (risk-taking/sensation seeking), and empathy.
Participants reporting any drug use on the day of testing were excluded, as were any showing a positive plasma screen for MDMA/amphetamines (analysis carried out by enzyme assay followed by high-performance liquid chromatography/mass spectroscopy [Tricho-Tech, Cardiff, U.K.—www.tricho-tech.co.uk]). Genomic DNA was extracted from blood by using standard methods, and the 5-HTTLPR was determined by polymerase chain reaction followed by size separation of product
(8). All subjects provided written informed consent, and the study was approved by the Cambridge Local Research Ethics Committee.
Affective disturbance was examined by using the Beck Depression Inventory
(12) and the Affective Go/No-Go test
(13). The Beck Depression Inventory is a well-validated, 21-item, self-report rating scale for depression. The questions cover a variety of different symptoms of depression, and for each a score from 0 (no symptom) to 3 (severe symptom) can be recorded. Thus the maximum score is 63, although scores higher than 40 are rarely recorded. The Beck Depression Inventory manual recommends a cutoff point of 9 for mild depression.
The Affective Go/No-Go test is a computerized neuropsychological test, details of which have been described previously
(13). On each trial, a word that is either happy or sad appears briefly on the screen, and subjects must make or withhold a response on the basis of the emotion of the word within approximately 1 second. On each block of 18 trials, half the words are happy and half are sad, and subjects are instructed that they must respond either to the happy words or to the sad words. Every two blocks, the targets and the distractors change—words that were previously targets become distractors and vice versa. Such blocks are defined as “shift” blocks, and blocks where the targets and distractors are of the same emotion as in the previous block are defined as “nonshift.” Three measures are recorded for each block: mean correct response latency, total false alarms (commission errors), and total misses (omission errors).
In the Affective Go/No-Go test, healthy volunteers typically respond faster to happy words than sad words, depressed patients show the opposite pattern of results, and both groups reduce commission errors from shift to nonshift blocks
(13). The test is sensitive to monoamine depletions
(14–
16), and a neuroimaging version has been developed in which patients with depression show enhanced neural response to sad distractors
(17).
Results
The drug-naive comparison group and the cannabis-using comparison group did not differ on any behavioral measure, either overall or when genetic subgroups were compared directly, and for the purpose of analysis were pooled into a single comparison group. The genotype frequencies in the comparison group (ll N=21 [36%], ls N=26 [45%], ss N=11 [19%]) and the Ecstasy users (ll N=20 [30%], ls N=31 [47%], ss N=15 [23%]) did not differ from the values expected under Hardy-Weinberg assumptions (χ2=0.20, df=1, p=0.65, and χ2=0.34, df=1, p=0.56, respectively). There were no significant differences in 5-HTTLPR genotype frequency (χ2=0.56, df=2, p=0.75) and allele frequency (χ2=0.59, df=2, p=0.44) in the Ecstasy and comparison groups, suggesting that the 5-HTTLPR is not a major predictor of Ecstasy use. The genetic subgroups did not differ in terms of age, IQ, or any measure of illicit drug use in either the Ecstasy users or the comparison subjects.
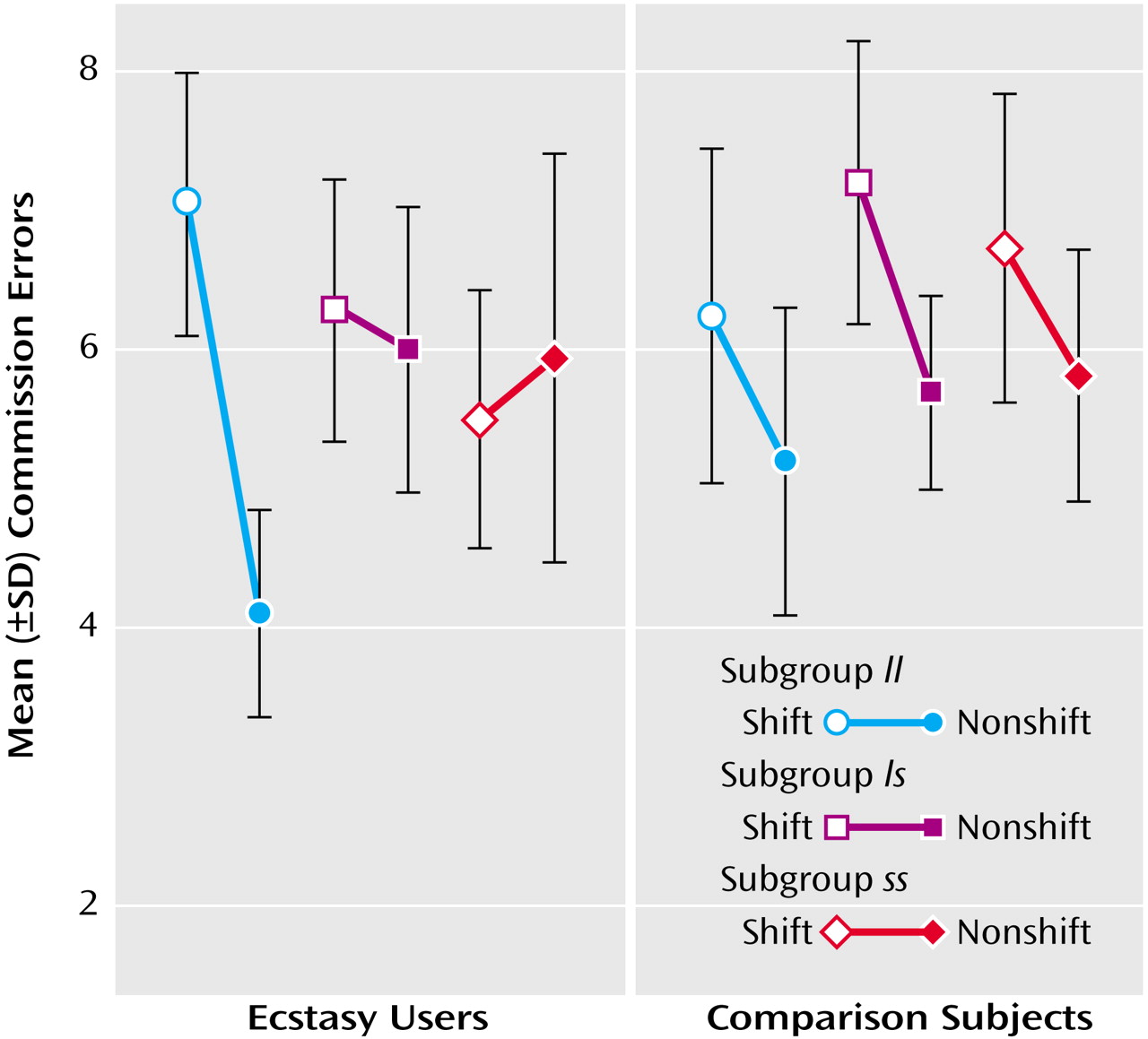
Repeated-measures analysis of variance (ANOVA) was used to examine data from the Affective Go/No-Go test. There was a highly significant shift-by-genetic-subgroup interaction for commission errors in the Ecstasy users (F=6.81, df=2, 64, p<0.003) but not in the comparison subjects (F=0.16, df=2, 55, p=0.85). In the
ll subgroup of the Ecstasy users, and in all genetic subgroups in the comparison group, commission errors declined as expected from shift to nonshift blocks. However, the
ls and
ss subgroups of Ecstasy users did not make the expected reduction in errors from shift to nonshift blocks (
Figure 1).
Since all Ecstasy users in this study also took other drugs, we conducted further analyses to control for the possible effects of non-Ecstasy illicit drug use. The ANOVA was repeated within the Ecstasy users, including non-Ecstasy illicit substance use (classed as either regular or rarely/never) as an additional between-subjects factor in separate analyses for psilocybin, LSD, amphetamine, amyl nitrate, ketamine, cocaine, and heroin. In no instance was the interaction term between drug use group, genotype group, and shift significant. However, because almost all Ecstasy users also used cannabis on a regular basis, this method was not appropriate to control for cannabis use. Instead, we conducted the analysis in the cannabis comparison subjects alone and did not find an interaction between genetic subgroup and shift.
Depression scores were not normally distributed and were analyzed in two ways. First, the Mann-Whitney U test was used to compare Beck Depression Inventory scores of the Ecstasy users and comparison subjects within each genetic subgroup. The Ecstasy users scored significantly higher on the Beck Depression Inventory than comparison subjects within the ss (Ecstasy group mean=11.8, SD=9.6; comparison group mean=3.9, SD=3.2) (z=2.4, p<0.02) and ls (Ecstasy group mean=8.1, SD=5.5; comparison group mean=5.2, SD=5.6) (z=2.4, p<0.02) genotype subgroups, but the difference in the ll subgroup was not significant (Ecstasy group mean=7.5, SD=6.0; comparison group mean=5.3, SD=3.1) (z=1.0, p=0.32).
Second, each individual was categorized as either not depressed or depressed on the basis of the accepted cutoff point of 9 on the Beck Depression Inventory. The proportions of individuals categorized as depressed or not depressed showed a strong tendency to differ in the Ecstasy users when classified by 5-HTTLPR genotype (χ2=5.95, df=2, p<0.06)—there were more individuals categorized as depressed in the ss subgroup of Ecstasy users. The proportions of depressed versus nondepressed individuals did not show this tendency to differ as a function of 5-HTTLPR genotype in the comparison group (χ2=0.55, df=2, p=0.76).
Adult Impulsiveness, Venturesomeness and Empathy Scale scores were analyzed in a univariate ANOVA with group and genetic subgroup as between-subjects measures. The Ecstasy users scored higher than the comparison subjects on impulsiveness (F=5.8, df=1, 118, p<0.02), with no effect of genetic subgroup and no group-by-genetic-subgroup interaction (F<1, df=2, 118, for both). However, amphetamine exposure correlated highly significantly with impulsiveness in the Ecstasy users (F=15.2, df=1, 56, p<0.001), and when those who had used amphetamine regularly were removed from the analysis, the remaining Ecstasy users (N=40) were not significantly more impulsive than the comparison subjects (F<1, df=1, 96). There were no differences between the Ecstasy and non-Ecstasy groups or genetic subgroups, and there were no interaction effects on venturesomeness or empathy (p>0.1 for all).
Discussion
We believe that these are the first data to suggest that the 5-HTTLPR genotype mediates emotionally related cognitive disturbance in Ecstasy users. Because Ecstasy causes long-term reductions in synaptic 5-HT release
(18), it is of interest to note the similarities of our current results to those seen in normal subjects after acute tryptophan depletion, a dietary manipulation that lowers availability of the precursor of 5-HT to the brain and temporarily reduces synthesis
(19). Healthy volunteers under conditions of acute tryptophan depletion show the same behavior on the Affective Go/No-Go test as the
ls and
ss groups of Ecstasy users—they fail to reduce commission errors from shift to nonshift blocks
(15). Moreover,
ss individuals who have never suffered from depression show the greatest mood change under acute tryptophan depletion, while
ll individuals show little or no mood change
(20), a result concordant with our finding that
ss Ecstasy users were the group that scored highest on the Beck Depression Inventory. It is possible that possession of the
s allele confers particular vulnerability to disturbances in emotional processing following 5-HT depletion, whether by acute tryptophan depletion or chronic Ecstasy use, perhaps due to low levels of tonic serotonergic neurotransmission.
This similarity with acute tryptophan depletion is intriguing, but it remains possible that the differences between the genetic subgroups among the Ecstasy users are caused by some other factor. Data from the Adult Impulsiveness, Venturesomeness and Empathy Scale did not provide evidence of personality differences between the genetic subgroups. In fact, our results suggest that the greater impulsivity in Ecstasy users found in other reports may be due to concomitant use of amphetamine. However, Soar et al.
(21) calculated that 34% of those in whom Ecstasy triggers a psychiatric disorder had a family history of psychopathology, and it may be that Ecstasy users carrying the
s allele have a family history of depression.
In summary, we have identified a test of emotional processing that is overtly abnormal in chronic Ecstasy users with specific 5-HTTLPR genotypes carrying the s allele. These data are compatible with the finding of a trend toward higher depressive scores on the Beck Depression Inventory in Ecstasy users with the ss genotype. Since such effects may have been overlooked if we had not stratified our samples by this genotype, future studies examining the long-term effects of Ecstasy use should consider the potential for gene-environment interactions at the 5-HTTLPR locus.