Patients with alcohol dependence can be clinically clustered into heterogeneous groups. Cloninger
(1) identified two genetic subtypes of alcoholics. Individuals with type I (milieu-limited) alcoholism have characteristics that include a later onset of alcohol-related problems, the development of psychological rather than physical dependence, and guilt related to their alcohol use. Subjects with type II (male-limited) alcoholism, on the other hand, manifest alcohol problems at an earlier age, show spontaneous or compulsive alcohol-seeking behavior, and are socially disruptive when drinking.
Although the pathogenesis of each clinical syndrome has not been clearly elucidated, it is likely that variation in alcohol elimination and acetaldehyde oxidation, genetically determined by alcohol dehydrogenases 1–3 (ADH1, ADH2, and ADH3) and aldehyde dehydrogenase (ALDH2), plays a central role
(2). High blood concentration of acetaldehyde causes extremely unpleasant symptoms. Individuals possessing high-active ADH2*2 and ADH3*1 alleles generate acetaldehyde much more rapidly after alcohol consumption and are thus less tolerant of alcohol
(3). The inactive ALDH2*2 allele, discovered only in Orientals, delays the clearance of acetaldehyde and protects against alcohol abuse
(3).
To determine the genetic characteristics of alcohol metabolism in Cloninger’s type I and type II alcoholism, we analyzed the polymorphisms of ADH2, ADH3, and ALDH2 genes in healthy men and in men with type I or type II alcoholism.
Method
The subjects were 72 Korean male patients (mean age=45 years, SD=9) who met DSM-IV criteria for alcohol dependence and were classifiable definitely into type I (mean age at onset=36 years, SD=7) and type II (mean age at onset=22 years, SD=2) alcoholism according to the criteria of Cloninger
(1). The patients had been admitted to Han-Gang Sacred Heart Hospital, Seoul National Mental Hospital, or Yong-In Mental Hospital. The comparison subjects were 38 unrelated healthy Korean men (mean age=34 years, SD=10) who visited the Health Screening Center in Han-Gang Sacred Heart Hospital. After a complete description of the study to the subjects, written informed consent was obtained.
The patients and comparison subjects were carefully assessed for their drinking patterns, alcohol-related problems, and psychiatric diagnoses by psychiatrists’ interview. The subjects had no major medical or psychiatric illnesses other than alcohol-related disorders in the patients.
Genomic DNA was extracted from peripheral blood leukocytes by using a standard phenol-chloroform method. We genotyped ADH2, ADH3, and ALDH2 by polymerase chain reaction amplification of DNA fragments containing targeted differences in base pairs. The positions and sequences of primers to amplify DNA fragments were based on minor modifications of the methods described by Xu et al.
(4) for ADH1–3 and Crabb et al.
(5) for ALDH2.
Genotype and allele frequency comparisons were performed by using the chi-square method with Monte Carlo simulation
(6) as implemented by a computer program developed by Dave Curtis (http://www.mds.qmw.ac.uk/statgen/dcurtis/software.html).
Results
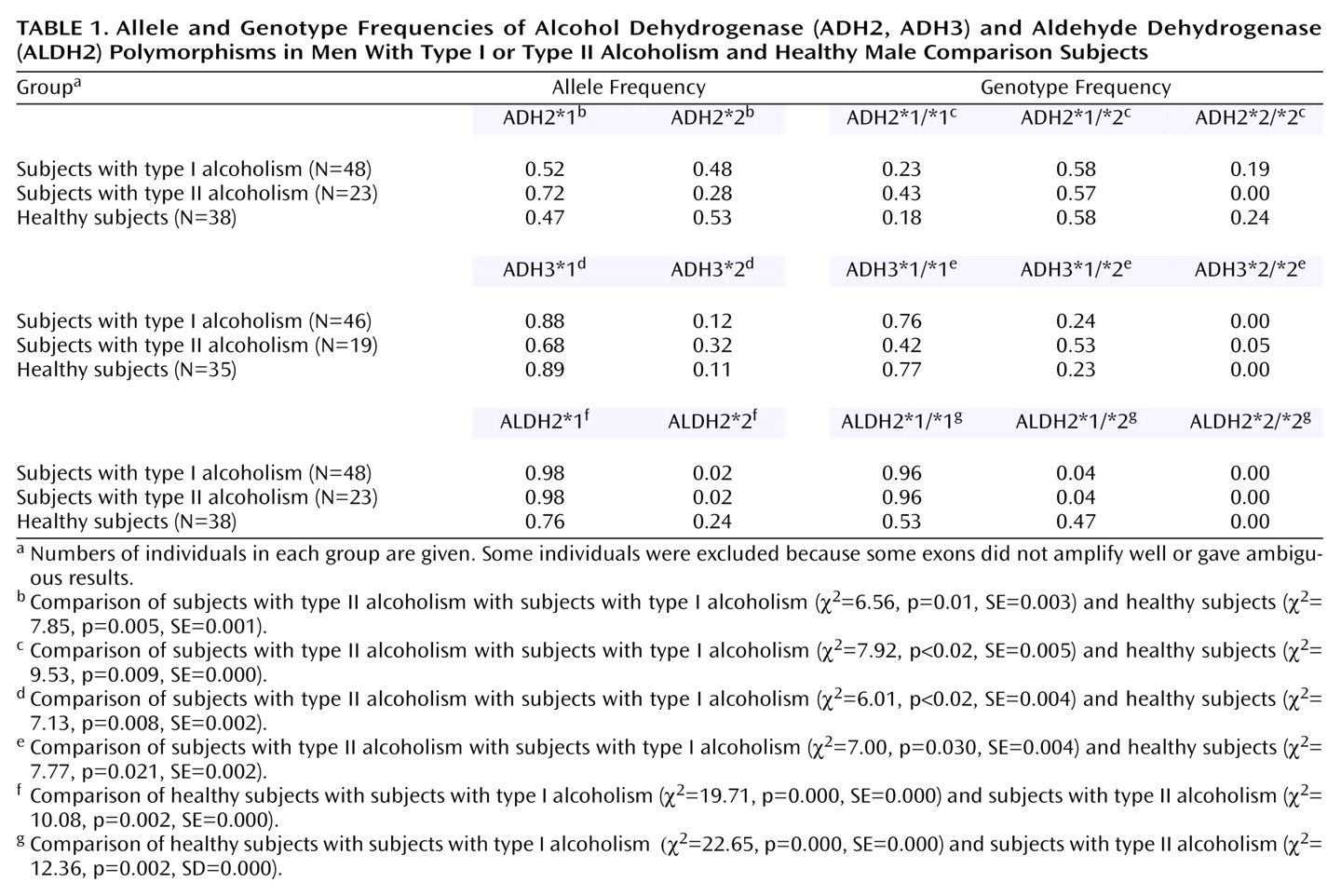
The frequencies of low-active ADH2 (ADH2*1/*1) and ADH3 (ADH3*1/*2 or ADH3*2/*2) genotypes were significantly higher in men with type II alcoholism (43% and 58%, respectively) than in men with type I alcoholism (23% and 24%, respectively). The allele and genotype frequencies of ADH2 and ADH3 were not different between men with type I alcoholism and healthy men (
Table 1).
The frequency of active ALDH2 (ALDH2*1/*1) genotype was significantly higher in men with alcohol dependence than in healthy men (96% versus 53%, respectively). Inactive ALDH2 (ALDH2*1/*2 or ALDH2*2/*2) genotype was present in only 4% of men with alcohol dependence, whereas 47% of the healthy men had inactive ALDH2. The frequencies of ALDH2 alleles and genotypes were not different between men with type I and type II alcoholism (
Table 1).
The subjects in the overall study group, and in each comparison group, were in Hardy-Weinberg equilibrium.
Discussion
To our knowledge, this paper is the first report of a significant difference in allele and genotype frequencies of ADH2 and ADH3 between patients with type I and type II alcoholism. The allele and genotype frequencies of ADH2 and ADH3 were similar in men with type I alcoholism and healthy men. Healthy nonalcoholic men and men with type I alcoholism might retain high-active ADH2*1/*2, ADH2*2/*2, and ADH3*1/*1 genotypes that produce and cumulate acetaldehyde more rapidly, thus delaying or preventing the development of an alcohol problem.
The frequencies of ALDH2 alleles and genotypes were significantly different between men with alcohol dependence and healthy men. Healthy nonalcoholic men might retain an inactive ALDH2*1/*2 genotype that delays the clearance of acetaldehyde and protects against alcohol dependence.
The subjects included only a small number of Korean men, limiting generalizability of the findings. In addition, this is an association study, showing an association between certain genetic polymorphisms and diagnostic subgroups. This does not establish causality. The results suggest that the genotype that is expected to either metabolize ethanol to acetaldehyde more rapidly or slow the conversion of acetaldehyde to acetate protects against an alcohol problem, mitigating the development of early-onset, severe alcohol dependence rather than decreasing the risk for developing alcohol dependence.
Subjects with type II alcoholism are genetically less likely to experience adverse physiological consequences of alcohol consumption than those with type I alcoholism. Schuckit et al.
(7) suggested that the early ability to tolerate consumption of large quantities of alcohol in the sons of alcoholics is a specific risk factor for later alcoholism. Heritable metabolic differences might contribute to type-related differences in ability to tolerate alcohol consumption. The results of our study suggest that type I alcoholics had genetic characteristics of alcohol dehydrogenases similar to those of normal comparison subjects and genetic characteristics of aldehyde dehydrogenase similar to those of type II alcoholics. The ALDH2 gene may play a major role in developing alcohol dependence, and both ADH2 and ADH3 genes may play the role in severity of alcohol dependence. We presume that the genetic characteristics of alcohol metabolism of type I alcoholism fall between nonalcoholism and type II alcoholism.