Excessive alcohol consumption has been associated with a wide array of adverse outcomes, including serious health problems, accidents, injuries, violence, social problems, disability, and death
(1). Annually, in the United States, alcohol misuse is estimated to be responsible for approximately 100,000 deaths
(2) and $185 billion in economic costs
(3).
Prevalence estimates of alcohol abuse/dependence among medical outpatients typically range from 2% to 9%
(4,
5). In addition, up to 10% have been found to engage in harmful drinking and up to 29% in risky drinking, that is, drinking enough to experience or to be at risk for experiencing harm from alcohol use but not enough to meet criteria for abuse/dependence
(4,
5). Given the seriousness and prevalence of alcohol problems, coupled with evidence that brief behavioral counseling interventions can be effective in reducing alcohol consumption and improving health outcomes
(4,
6), groups such as the U.S. Preventive Services Task Force and the National Institute on Alcohol Abuse and Alcoholism recommend screening of adults in primary care settings to reduce alcohol misuse
(1,
7).
Nevertheless, consistent with recommendations for screening, the Department of Veterans Affairs (VA), which operates the nation’s largest integrated health care system, requires annual alcohol screening and monitors screening as a quality measure
(9), although, here too questions have been raised about the appropriateness of translating general practice guidelines into performance measures
(10). With ongoing debate over routine screening for alcohol problems as a backdrop, we set out to examine the “real world” experience of the VA in implementing a large-scale, system-wide policy of screening. In this study, we used available data to follow the chain of events from initial screening to subsequent diagnosis of alcohol use disorder. Specifically, we sought to determine, in a large national sample of VA medical outpatients, the rates and predictors of 1) screening for alcohol problems, 2) positive screenings, 3) follow-up evaluation, and 4) subsequently confirmed diagnoses of alcohol use disorder. By determining the extent to which patients in the VA system are screened and later diagnosed with alcohol use disorders and by identifying factors associated with steps in the pathway, the results of this study are expected to improve our understanding of the screening process in actual, real-world clinical practice.
Results
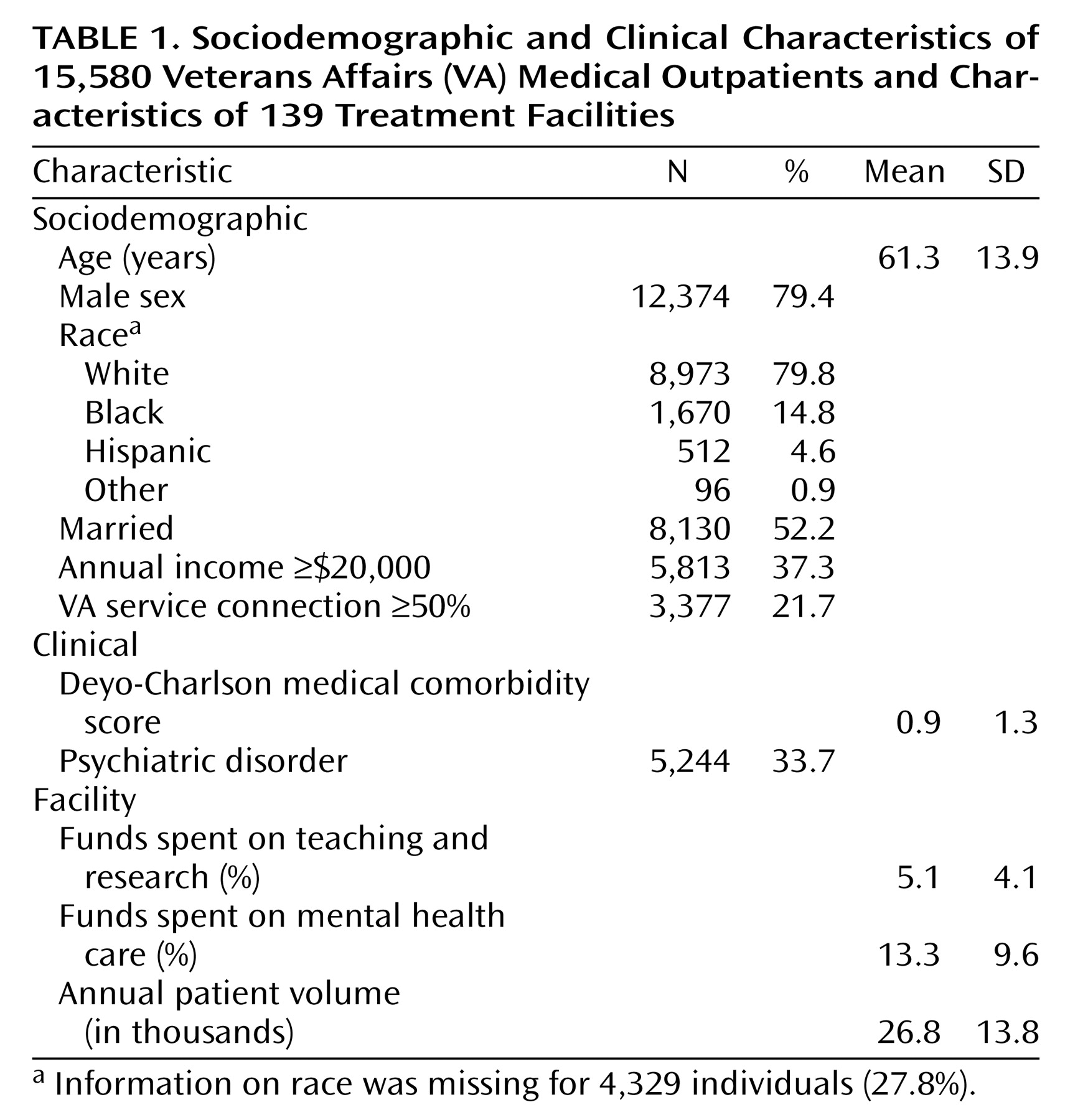
The sample for the present study included 15,580 patients drawn from 139 VA medical centers nationally. Distributions of both individual and facility characteristics are summarized in
Table 1. The sample had a mean age of 61.3 years (SD=13.9). The majority of the sample was male, white, married, and of relatively low income. A substantial proportion (21.7%) had at least 50% VA service connection.
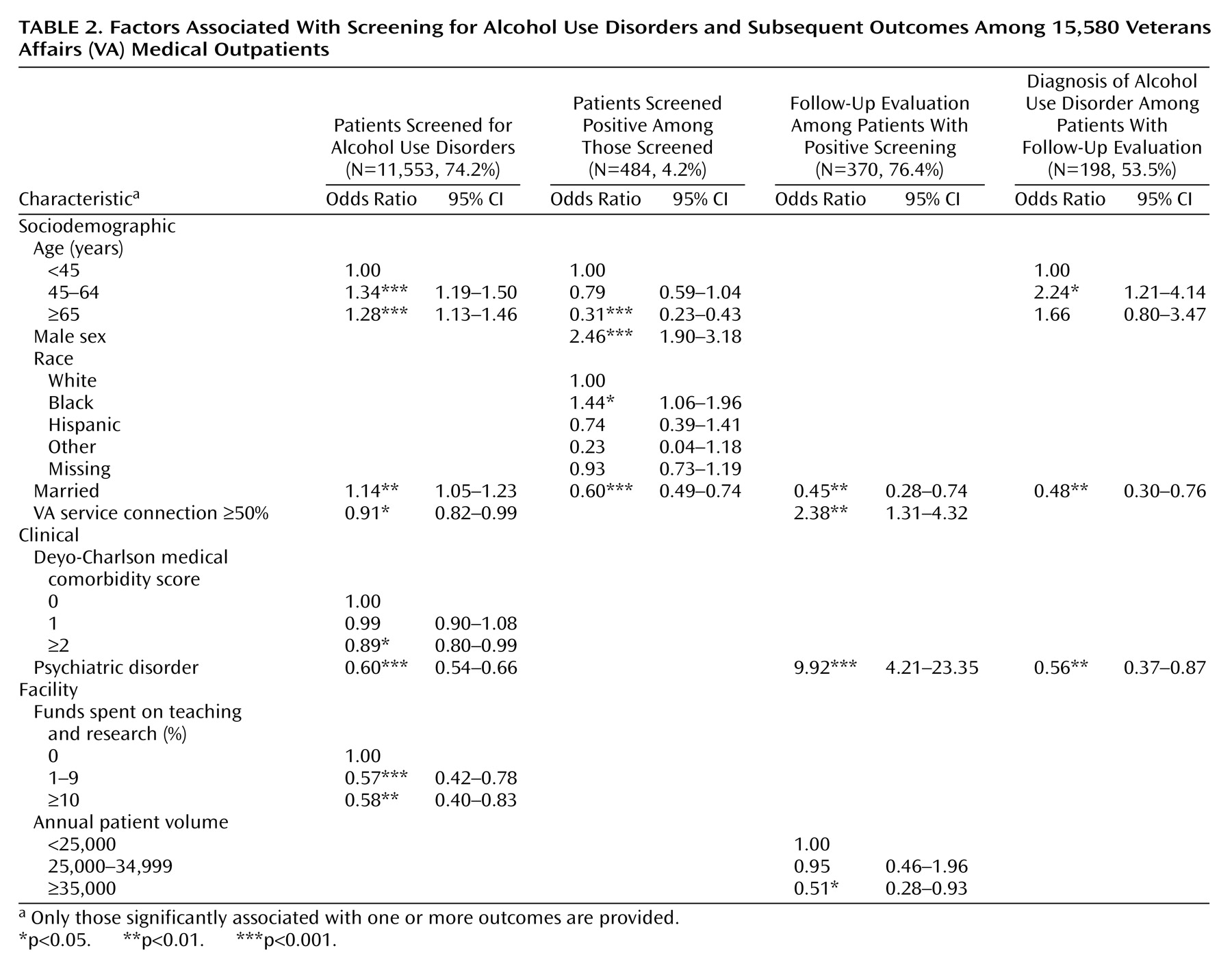
Nearly three-quarters of the eligible patients (N=11,553) were screened for alcohol use disorders in the past year (
Table 2). Of these, 4.2% (N=484) screened positive. Of those who screened positive, three-fourths (N=370) received follow-up evaluations. Of those followed up, 53.5% (N=198) were subsequently diagnosed with an alcohol use disorder—1.7% of the originally screened sample.
Results of the multivariate analyses are also presented in
Table 2. Compared with those age less than 45 years, older persons were significantly more likely to be screened for alcohol problems; however, if screened, they were less likely to screen positive, particularly those ages 65 years and over. The likelihood of being followed up after a positive screening did not differ across age groups, but if followed up, middle-age adults were significantly more likely than those ages <45 years to be diagnosed with an alcohol use disorder. The odds of alcohol screening and subsequent outcomes did not significantly differ by gender, race, or income level, with the exception of a greater likelihood of screening positive among men and black patients.
Married individuals were significantly more likely to be screened; however, they were less likely to screen positive, to be followed up, and to subsequently receive an alcohol use diagnosis. Conversely, veterans with greater service-connected disability and those with a psychiatric disorder were less likely to be screened but more likely to be followed up if they screened positive. Patients with greater medical comorbidity were also less likely to be screened for alcohol problems.
In terms of facility characteristics (
Table 2), the likelihood of being screened for alcohol problems was lower at academically affiliated medical centers. Follow-up evaluation of a positive screening was less likely at the largest facilities. Receipt of alcohol screening and subsequent outcomes did not significantly differ with level of funding for mental health care.
Discussion
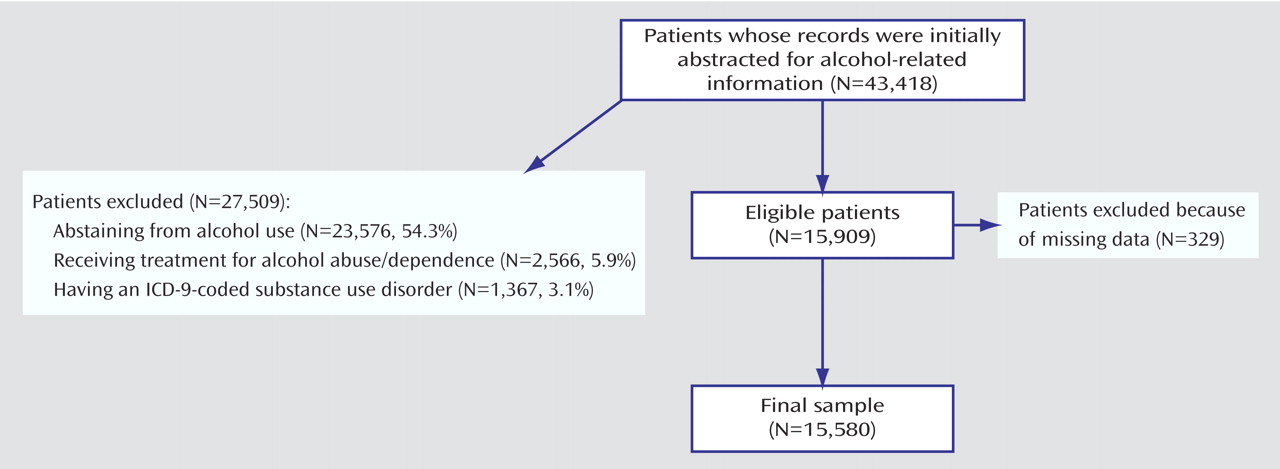
Using data from a national sample of medical outpatients in the VA system, we sought to evaluate the chain of events from alcohol screening to the diagnosis of alcohol use disorder. In total, three-fourths (74.2%) of the eligible patients had chart-documented alcohol screening in the past year. Of these, 4.2% screened positive. Of those who screened positive, 76.4% received follow-up evaluation, and of these, over half (53.5%) were subsequently diagnosed with an alcohol use disorder, representing 1.7% of the total sample that was screened. This overall rate of diagnosis is somewhat lower than the often-cited prevalence estimates of 2% to 9% for alcohol abuse/dependence in medical outpatient samples
(5). In this study, however, a total of 3,933 patients (9.0%) were excluded if they were already known to have a substance use diagnosis and/or were in treatment; thus, the focus was on identifying new cases among at-risk patients.
The relatively low yield raises questions regarding both the value of large-scale, routine screening to detect alcohol problems and the frequency of screening. Beich and colleagues
(8) argued that universal screening in general practice is not an effective case-finding strategy. In the present study, for every case that was identified, about 58 persons (11,553÷198) were screened, and nearly two (370÷198) received a follow-up diagnostic evaluation, either in primary care (59.2%) or by a mental health provider (40.8%). To crudely estimate the cost of identifying one case of alcohol use disorder, we assumed the following: 1) each screening cost $4.88, based on the estimate of Valenstein and colleagues
(20) for depression screening, and 2) subsequent diagnostic evaluations cost $33.68 if performed in primary care (CPT code 99213) or $138.77 if performed in a specialty mental health clinic (CPT code 90801) with information from the 2000 Medicare Physician Fee Schedule and total facility relative-value units. Under these assumptions, the estimated cost of identifying each case would be $428. Given the health, social, and economic burdens of alcohol misuse, this may well be justified. Unfortunately, detailed treatment and outcome data were not available; thus, a rigorous cost-effectiveness analysis was not possible. Nevertheless, targeted efforts aimed at high-risk patients may improve the overall effectiveness and yield of case-finding activities.
In addition, although the U.S. Preventive Services Task Force recommends screening, it notes that the optimal interval for screening is unknown
(7). The low rate of case identification observed in this study may suggest that less-than-annual screening may be a more cost-effective approach, particularly for lower-risk patients.
In the present study, we found that potential risk factors for alcohol problems, such as being younger, unmarried, and disabled, as well as having greater medical and psychiatric comorbidities, were paradoxically associated with a decreased likelihood of alcohol screening. Considerable epidemiological and clinical research has demonstrated strong associations between these characteristics and the prevalence of alcohol use disorders
(1,
21,
22). It thus appears that patients who may be at the greatest risk for alcohol abuse and dependence are, in fact, the ones least likely to be screened, and therefore, substantial numbers of cases may be missed.
These findings are consistent with the literature on “competing demands” in the primary care setting
(23,
24), which asserts that a patient with multiple problems may receive poorer quality care for a given individual problem because of the competing demands placed on the clinician’s attention. In this view, lack of time is one of the most common barriers to performing a variety of preventive and screening services. At each encounter, clinicians must prioritize the competing demands of acute treatment, clinical preventive services, and patient requests. Given the limited time typically allowed for medical visits, this may be particularly challenging for patients with chronic conditions and multiple complaints.
With respect to the facility characteristics examined, we found a strong negative association between spending on teaching and research and the likelihood of screening patients for alcohol use disorders. One explanation may be that residents, who provide much of the care at academically affiliated facilities, are less likely than attending physicians to adhere to the alcohol screening guideline. Indeed, consistent with this, Burns and colleagues found a similar pattern of association between level of physician training and women’s receipt of screening mammography
(25) and clinical breast examination
(26). In addition, research and teaching may in some way distract from the provision of clinical preventive services—another example of competing demands. In an earlier study by Linn and Yager
(27), the authors found that greater experience treating alcohol problems was associated with less academic work. Another possibility is that many primary care providers express skepticism about the effectiveness of screening and the adequacy of treatment resources
(28,
29), and in the present study, this may have been disproportionately true at more academically affiliated medical centers.
Follow-up evaluation of a positive screen is a critical step in properly identifying individuals who have alcohol problems and would benefit from treatment. In this study, we found that only three-fourths of those who screened positive were actually followed up. Facility size was negatively associated with follow-up evaluation of a positive screening. Patients at the largest medical centers may experience greater barriers in terms of factors, such as timely referral and coordination of care, thus decreasing the likelihood of appropriate follow-up.
This study had several limitations. First, our ability to examine variables, such as race, was limited by the quality of the available chart-review and administrative data. Second, the findings may not generalize to non-VA settings. The VA system is unique in several respects, including its use of electronic medical records and clinical reminders for performing preventive services. In addition, the VA is the largest integrated health care system in the country and is geared toward caring for patients with serious mental illness
(17), which may, in part, help to explain the lack of association between facility-level variation in mental health spending and the likelihood of alcohol screening and subsequent outcomes. Further studies are needed to determine whether our findings are replicated in non-VA settings.
Third, according to the EPRP chart-review data, over 90% (10,807 of 11,553) of the screenings were performed with the CAGE questionnaire
(30); thus, the focus of screening was to detect clinical alcohol abuse/dependence. The Alcohol Use Disorders Identification Test, however, has been shown to be more sensitive in terms of detecting less severe alcohol problems, such as risky and harmful drinking
(5,
31,
32). Indeed, the VA now mandates use of the Alcohol Use Disorders Identification Test, or the shortened version
(33), as the preferred screening instrument, which will likely increase the identification of patients whose levels or patterns of alcohol consumption do not meet the criteria for abuse/dependence but, nevertheless, place them at increased risk for adverse health and social outcomes. Future work will be needed to ensure that patients with alcohol disorders are not only identified but also followed up and treated appropriately by using therapies that have been shown to be effective in reducing alcohol consumption across the spectrum of alcohol disorders
(6). Receipt and adequacy of treatment—the lack of which following systematic identification of problems through screening may be considered unethical—were not assessed in the present study.
Fourth, information was not available on factors such as who performed the screenings. In practice, such screenings are often administered by a VA clinic nurse, which would tend to make screening more cost-effective and less burdensome on providers’ time. In addition, we could not evaluate whether being screened by a regular, familiar provider as opposed to another clinician influenced the likelihood of accurately reporting alcohol problems and of being followed up.
These limitations notwithstanding, the results of this study raise important issues regarding routine annual screening for alcohol problems among medical outpatients. Further work is needed to determine the cost-effectiveness of screening and intervention
(34,
35) and the optimal interval for screening in real-world clinical practice, particularly among lower-risk patients, in both VA and non-VA settings. To improve overall effectiveness, targeted strategies may be able to increase case-finding activities among patients who are at greatest risk for alcohol use disorders, as well as among those at more academically affiliated medical centers. Targeted efforts are also needed to ensure proper follow-up evaluation at larger facilities, where patients may experience greater system-level barriers.