For many medical conditions, early treatment often confers better prognosis, since the available effective treatments restore homeostasis, arrest the pathophysiological processes, and prevent further damage to healthy tissues. Such a paradigm of prevention is well demonstrated in cancer treatments. However, whether this approach is applicable in schizophrenia remains an area of intensive research.
Because many schizophrenia patients delay seeking treatment for 1–2 years after psychosis onset, an increasing number of health care delivery systems have dedicated resources to reduce this lengthy duration of untreated initial psychosis
(1). Another argument in support of reducing treatment delay has been the premise that early treatment prevents further neurobiological damage and translates into better outcome. However, the evidence for this second rationale remains mixed
(2).
We and others have previously found no significant associations between a variety of MRI brain morphometric measures (global and lobar brain volumes, indices of brain surface anatomy) and duration of untreated initial psychosis
(3,
4). The aim of this report was to extend these studies by examining the relationship between hippocampal volumes and duration of untreated initial psychosis. Not only is diminished hippocampus volume well replicated in schizophrenia
(5), at-risk individuals also have smaller hippocampi
(6). More important, the hippocampus is highly neuroplastic and is susceptible to damage from a wide variety of insults, including hypoxia and stress-induced glucocorticoid hypersecretion
(7). Therefore, if untreated psychosis were to induce neuronal damage through hypercortisolemia, excitotoxicity, or other as yet unknown mechanisms, the hippocampus would likely be a sensitive brain region for testing the “toxic psychosis” hypothesis.
Method
One hundred five subjects (64 male, 41 female) with DSM-IV schizophrenia (N=73), schizophreniform disorder (N=28), or schizoaffective disorder (N=4) were evaluated during their first episode of psychosis with the Comprehensive Assessment of Symptoms and History. The patient group had minimal prior neuroleptic exposure: 84 were neuroleptic naive, and no subject had >3 months of cumulative lifetime antipsychotic treatment (mean=0.35 months, SD=0.54). The mean age at illness onset was 23.2 years (SD=6.94), and the mean age at assessment was 26.6 years (SD=9.03). After a complete description of the study to the subjects, written informed consent was obtained.
As previously described
(8), duration of untreated initial psychosis was the time period between onset of full positive syndrome and initiation of antipsychotic treatment. “Full positive syndrome” was defined as the presence of any positive symptom (i.e., delusions, hallucinations, bizarre behaviors, positive formal thought disorder, or catatonic motor behavior) rated moderately severe or worse.
Images of the whole brain were obtained on a 1.5-Tesla GE Signa MR scanner (GE Medical Systems, Milwaukee). Three MR sequences—T
1-weighted spoiled grass, proton density, and T
2-weighted images—were acquired. Imaging parameters have been previously described
(9). Images were processed by using the BRAINS software package. Descriptions of image analysis methods have been provided elsewhere
(9). In this study, hippocampal volume was measured by using a reliable and validated semiautomated artificial neural network
(9,
10). Interrater reliability overlap values (i.e., the intersection of the two technicians’ traces divided by the union of their traces) for the left and right hippocampus were 0.75 and 0.74, respectively. Mean interclass correlation coefficients for the left and right hippocampal volumes were 0.92 and 0.83, respectively.
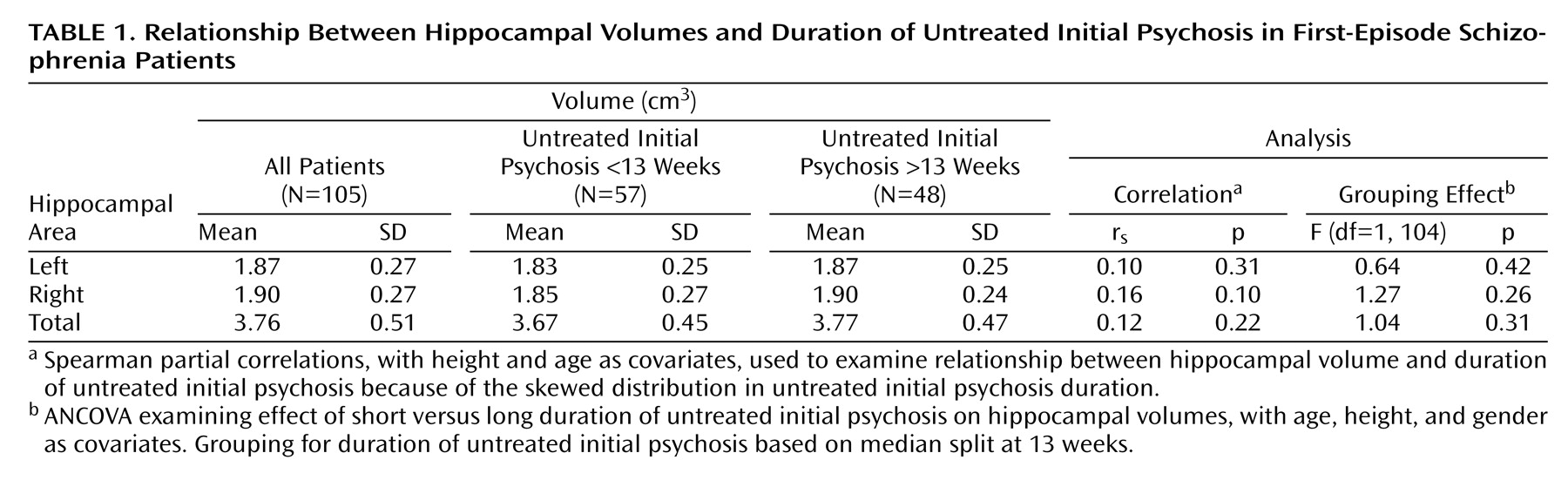
Because of the skewed distribution in duration of untreated initial psychosis, Spearman partial correlations (with height and age as covariates) were used to examine the relationships between duration of untreated initial psychosis and hippocampal volumes. In addition, subjects were also divided into two groups on the basis of median duration of untreated initial psychosis. Analysis of covariance—with height, age, and gender as covariates—tested the effects of short versus long duration of untreated initial psychosis on hippocampal volumes. Results were considered statistically significant if at or below the 5% probability level (two-tailed).
Results
The mean duration of untreated initial psychosis was 59.9 weeks (SD=118.0, median=13.0, 25th and 75th interquartile range=46.0). Results are summarized in
Table 1. No statistically significant correlations were seen between duration of untreated initial psychosis and left, right, or total hippocampal volume. When the patient group was split around the median duration of untreated initial psychosis (i.e., 13 weeks), no statistically significant grouping effects were observed on any of the three hippocampal volume measures.
Discussion
Our finding of no significant associations between treatment delays and hippocampal volumes is consistent with the only two other studies in the literature that focused on the relationship between duration of untreated initial psychosis and MRI brain volumes
(3,
4). Together with studies examining the effects of duration of untreated initial psychosis on neurocognition, which have also been mostly negative
(3,
4,
11), the weight of the evidence suggests that treatment delays may not be neurobiologically deleterious to the brain. Nonetheless, in studies that have examined the association between duration of untreated initial psychosis and clinical outcome, many reports
(12), but not all (8), have found longer duration of untreated initial psychosis to be related to poor outcome in schizophrenia. Furthermore, among programs in which dedicated early identification teams actively seek out psychotic patients for treatment, shortening duration of untreated initial psychosis is associated with better clinical outcome
(13).
These two sets of findings—1) paucity of significant associations between brain volumes/neurocognition and duration of untreated initial psychosis and 2) the fairly well replicated relationship between long duration of untreated initial psychosis and poor clinical outcome—remain difficult to reconcile. One explanation for this discrepancy may be that untreated psychosis has no direct neurotoxicity. Instead, the negative impact that treatment delays have on clinical outcome may be mediated through psychosocial factors, such as disruption of education and employment and reduced self-esteem. An alternative explanation for these conflicting results could also be that our current available treatments do not radically alter the neuropathophysiology of schizophrenia. While antipsychotics are efficacious in reducing psychotic symptoms and preventing symptom recurrence for schizophrenia patients as well as prodromal patients
(14), their role in restoring CNS homeostasis and preventing disease progression in schizophrenia remains controversial
(15). Recent longitudinal MRI studies have provided increasingly convincing evidence that despite adequate antipsychotic treatment, there are progressive brain volume reductions during the lifelong course of schizophrenia
(16). These ongoing neural changes suggest a need to develop more effective treatments for schizophrenia. If antipsychotics do not arrest disease progression in schizophrenia, the timing of antipsychotic treatment initiation, whether immediately following the onset of psychotic symptoms or deferred for 1–2 years, may have little impact on brain volumes or on neurocognition.
In conclusion, this study does not support the hypothesis that psychosis is neurotoxic. Reducing treatment delays is prudent and appears to enhance short-term treatment response. However, the treatments presently available have psychosis as their primary targets. Developing new therapeutics that fundamentally interrupt the neuropathophysiology of schizophrenia must remain as the goal for managing this devastating group of disorders. Primary and secondary prevention still offers hope that outcome in schizophrenia patients will eventually improve.