Age at onset variation may similarly reflect underlying genetic heterogeneity in bipolar disorder. Recent studies have suggested that there may be a mixture of overlapping distributions of age at onset in bipolar disorder
(7,
8), while other studies have shown that the clinical presentation of bipolar disorder, such as the occurrence of comorbid psychiatric disorders, may vary considerably with age at onset
(9–
12). In addition, some studies have reported that age at onset aggregates within bipolar disorder families
(13,
14), and a segregation analysis has found that the transmission of bipolar disorder may differ in early- versus late-onset bipolar disorder
(15).
We sought to extend these findings by using data from the NIMH Genetics Initiative for Bipolar Disorder to answer the following questions: 1) Can we replicate the finding that there is a mixture of overlapping age-at-onset distributions that define subgroups of bipolar disorder? 2) Does the clinical presentation of bipolar disorder differ across these age-at-onset subgroups? 3) Do the age-at-onset subgroups aggregate within families? 4) Does age at onset co-aggregate in families with other clinical features? Our goal was to assess the clinical evidence that variation in age at onset along with other clinical features reflects the underlying genetic heterogeneity of bipolar disorder and may be used to identify more homogeneous subgroups of families to facilitate mapping susceptibility genes that contribute to this disorder.
Results
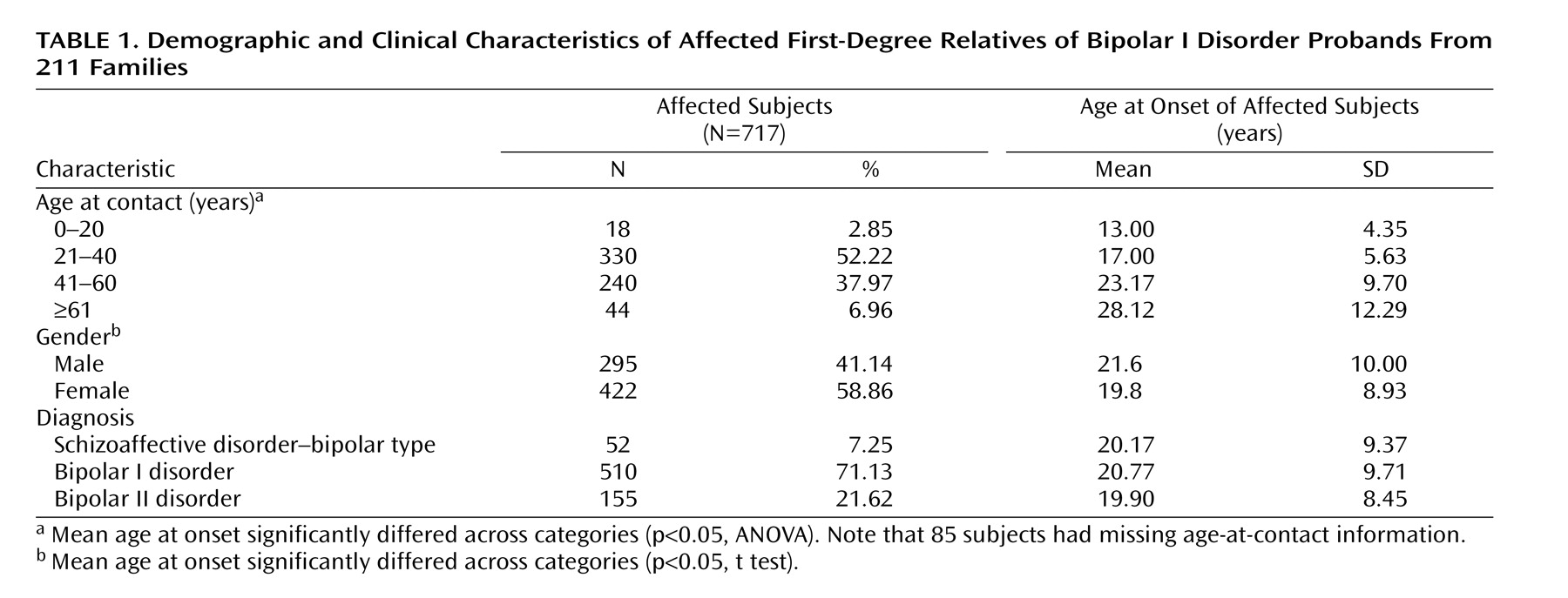
Table 1 shows the characteristics of the 717 subjects diagnosed with bipolar disorder in this study. The mean age at onset was significantly younger for female relative to male subjects, and the mean age at onset increased in relation to the age of contact. The mean ages at onset for subjects with schizoaffective disorder–bipolar type, bipolar I disorder, and bipolar II disorder were very similar.
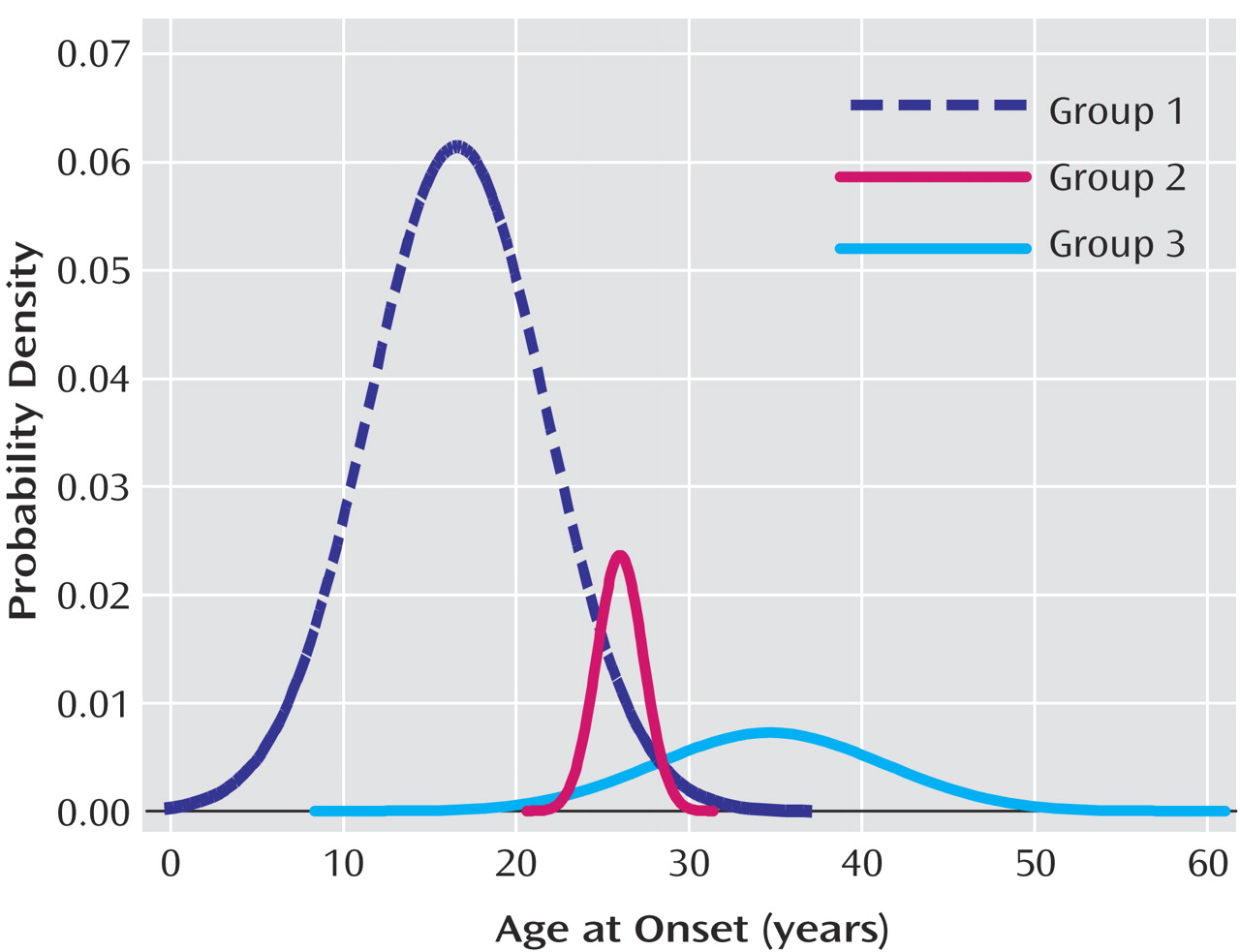
The distribution of age at onset in the probands from the 211 families was skewed. Admixture analysis yielded a best fitting model (based on Akaike’s information criterion) that suggested the observed distribution could be decomposed into a mixture of three normal distributions (
Figure 1). The three component age-at-onset distributions had means of 16.6 (SD=5.1), 26.0 (SD=1.4), and 34.7 (SD=6.6) years and comprised 79.7%, 7.2%, and 13.1% of the group, respectively. On the basis of these results, we divided the group into three age-at-onset subgroups with cutoff points at ages 21 (mean of the youngest group plus one standard deviation) and 28 (mean of the oldest group minus one standard deviation). Alternatively, since the youngest group occupied a substantially greater proportion than the sum of the other two groups, we combined the second and third age-at-onset subgroups to dichotomize early- and late-onset subjects at a cutoff point of age 21.
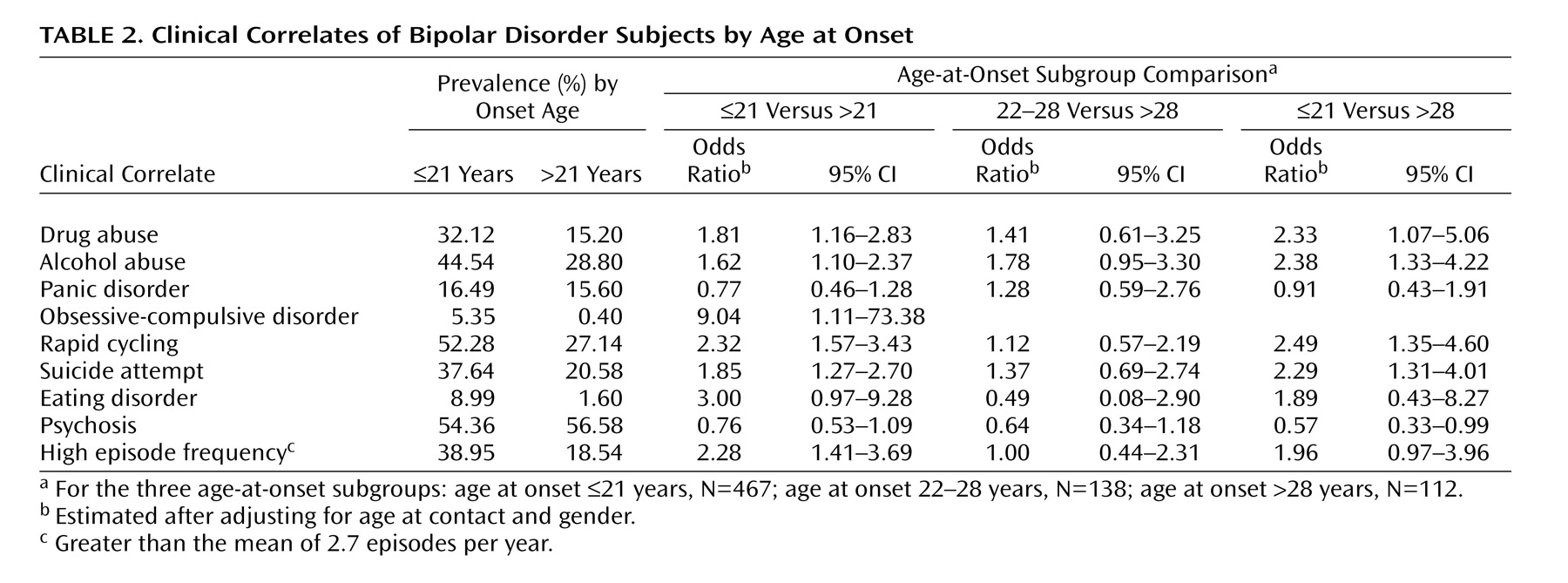
Table 2 shows the prevalence rates of each clinical correlate among the affected subjects by age at onset. Relative to subjects with a late onset, those with early-onset bipolar disorder were found to have significantly higher rates of drug abuse (z=4.73, p<0.001), alcohol abuse (z=4.08, p<0.001), obsessive-compulsive disorder (z=2.59, p<0.001), rapid cycling (z=5.81, p<0.001), suicide attempt (z=4.40, p<0.001), and episode frequency (z=3.90, p<0.001), with a higher rate of eating disorders that was nearly significant. Typically, the onset of the comorbid disorders occurred after the onset of bipolar disorder. For example, in over two-thirds of the cases the onset of drug or alcohol abuse was after the onset of bipolar disorder. Logistic regression analyses confirmed that early-onset subjects were at a higher risk of having these clinical correlates even after gender and age at contact were controlled. In general, subjects with an age at onset between 22 and 28 had similar, albeit slightly higher, risks relative to subjects with an age at onset >28. There were no apparent differences among the age-at-onset subgroups in the rates of panic disorder or mood-congruent psychosis. Conversely, early-onset subjects tended to have lower rates of psychosis, especially when comparing those with an onset of bipolar disorder ≤21 versus >28.
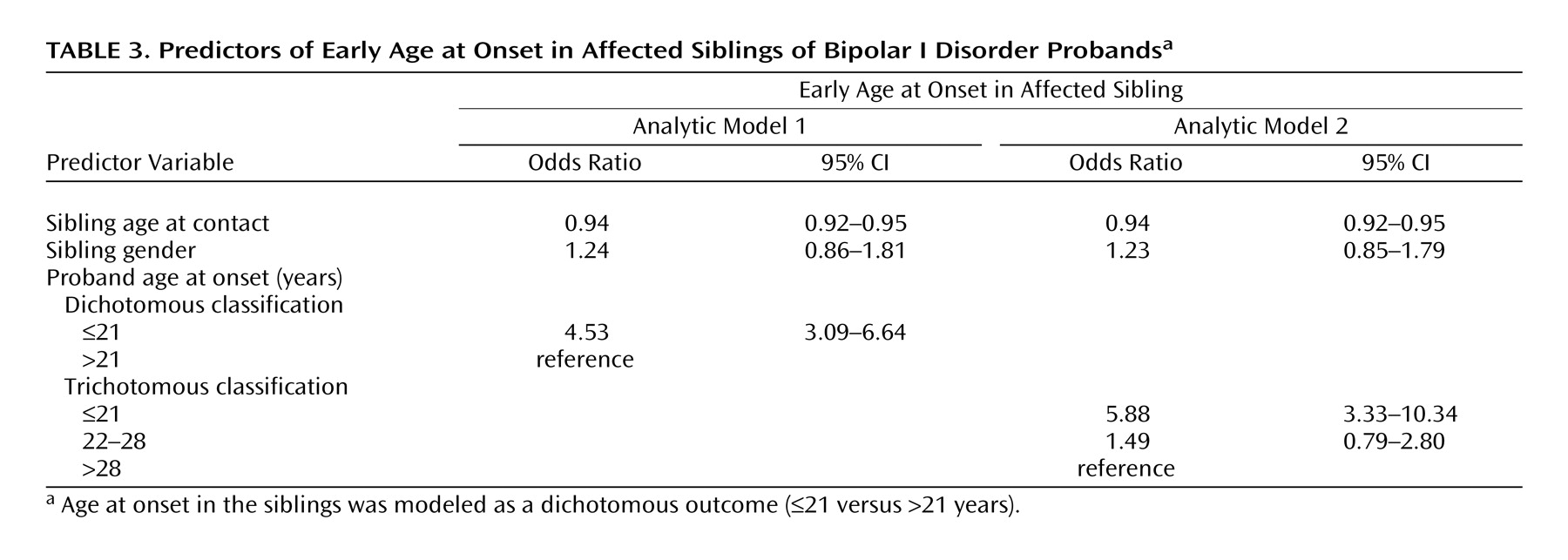
We used proband-predictive logistic regression models to examine whether age at onset aggregated in these families. Specifically, we tested if age at onset in the probands predicted age at onset in the siblings after age at contact and gender were controlled (
Table 3). Affected siblings of early-onset probands were over four times more likely than others to have an early onset. When we trichotomized age at onset in the probands (model 2), we found that compared with siblings of probands in the oldest age-at-onset group (>28), those in the youngest age-at-onset group (≤21) were significantly more likely to have an early onset. By contrast, siblings of probands in the middle age-at-onset group were no more or less likely to have an early onset.
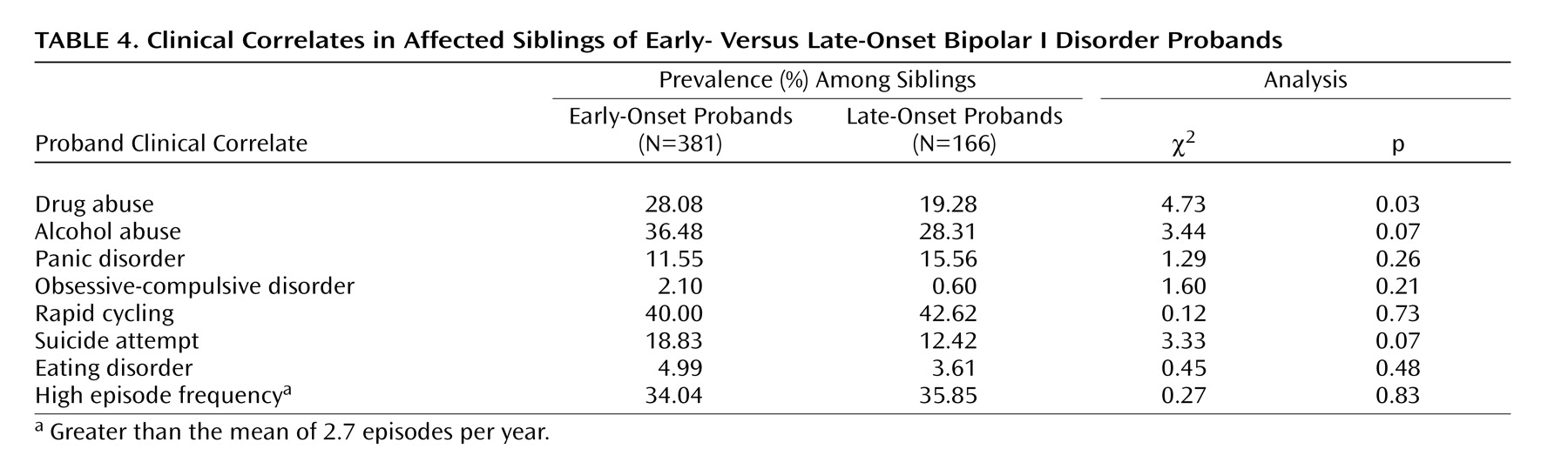
We then compared the prevalence rates of different clinical features among siblings of early- versus late-onset probands (
Table 4). The rates of suicide attempts and alcohol abuse were marginally higher in siblings of early-onset probands. However, the most compelling difference was observed for drug abuse. Prevalence rates of the other clinical features did not differ significantly among siblings of early- versus late-onset probands.
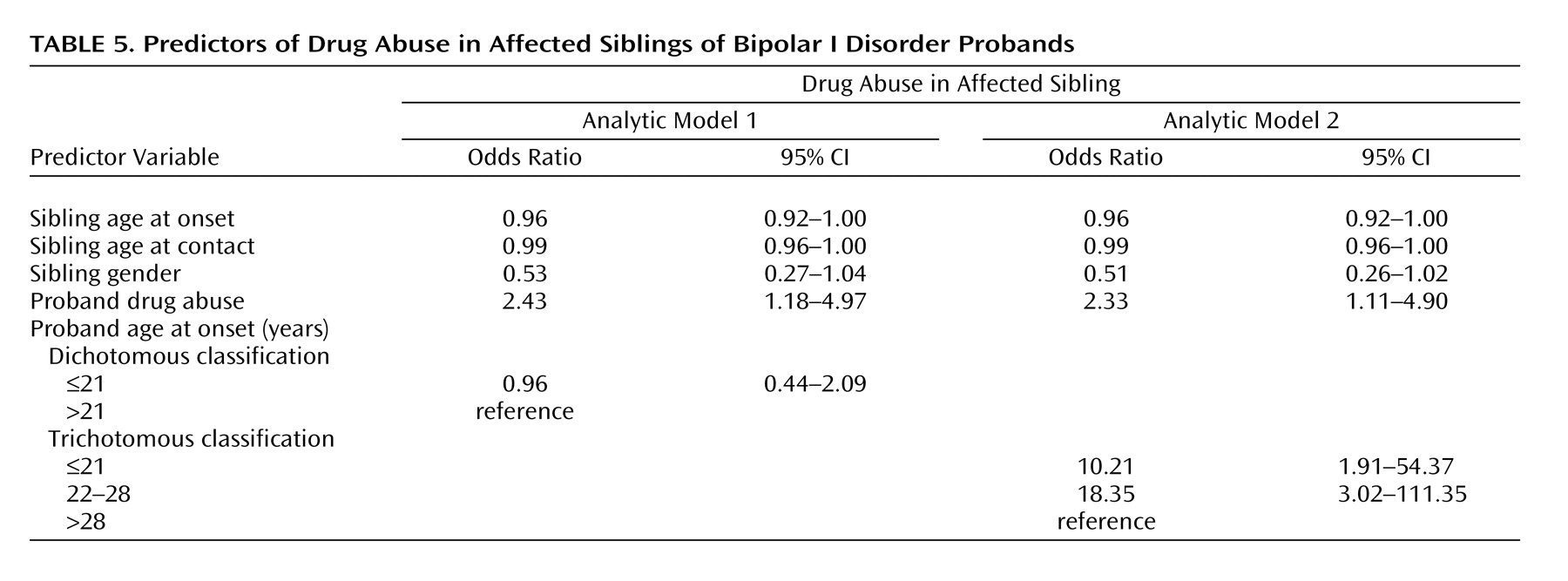
On the basis of these initial comparisons, we used a modification of the proband-predictive logistic regression model to more closely examine the familial co-aggregation of age at onset and drug abuse. Specifically, we tested whether age at onset in the probands predicted drug abuse in the siblings after we controlled for drug abuse in the probands as well as age at onset, age at contact, and gender of the siblings (
Table 5). In model 1 with dichotomous onset classification, proband age at onset did not appear to predict drug abuse in the siblings (odds ratio=0.96, 95% CI=0.44–2.09). However, in model 2 which had a trichotomous classification of proband age at onset, a significant association with drug abuse in the siblings was revealed. Compared with siblings of probands in the oldest age-at-onset group, those in the youngest age-at-onset group were over 10 times more likely to have drug abuse, and those in the middle age-at-onset group were over 18 times more likely. Because of the similar increase in risk, we collapsed the middle and youngest age-at-onset categories and found that siblings of probands with age at onset ≤28 were over 11 times more likely to have drug abuse (odds ratio=11.62, 95% CI=2.16–62.56) than siblings of probands with age at onset >28.
We reran the aforementioned models and controlled for disease duration (age at contact minus age at onset) instead of age at contact. Like age at contact, disease duration was correlated with age at onset (Pearson correlation r=–0.16, p<0.001) and may have also been an important potential confounder of the relationships we observed. However, the results with disease duration controlled were not meaningfully different (data not shown).
Discussion
We found that the skewed distribution of age at onset in our bipolar I disorder subjects could be decomposed by admixture analysis into three normal distributions with means of 16.6 (SD=5.1), 26.0 (SD=1.34), and 34.7 (SD=6.6) years that comprised 79.7%, 7.2%, and 13.1% of the group, respectively. Although there were differences in the estimated means and proportions of the component distributions, our findings were largely consistent with those reported by Bellivier et al.
(7,
8) in their studies of age at onset with two independent samples.
We used the results from our admixture analysis to empirically define cutoff points at ages 21 and 28 for distinguishing age-at-onset subgroups. We then examined if the clinical presentations of bipolar disorder differed across the age-at-onset subgroups. Consistent with previous studies, we found that early-onset subjects (age at onset ≤21) had higher risks of clinical features such as comorbid substance abuse
(19,
20), suicidality
(11,
20–23), rapid cycling
(11,
24), and increased episode frequency
(25). We also found that early-onset subjects were at greater risk for eating disorders (although this difference did not quite reach significance after gender and age at contact were controlled), an association that to our knowledge has not been previously examined. In general, subjects with an age at onset between 22 and 28 years were relatively similar in presentation to late-onset subjects (age at onset >28), albeit with slightly higher risks of the various features examined. These findings appear to suggest that early-onset bipolar disorder has a more severe course leading to the manifestation of numerous clinical complications. However, in contrast to previous studies, we did not find any association between early-onset bipolar disorder and higher risks of comorbid panic disorder
(10,
26). Furthermore, we found that early-onset bipolar disorder tended to be associated with lower rates of mood-congruent psychotic symptoms. Such findings contradict some earlier studies of mood-congruent psychosis
(27).
As noted by Bellivier and colleagues
(7), “if age at onset is a marker for biologically different subtypes of bipolar disorder, then age-at-onset subgroups should have separate normal distributions with different means, variances, and population proportions as well as different clinical characteristics.” Our results, therefore, would appear to support the conclusion that age at onset is a clinical marker of biological heterogeneity in bipolar disorder.
In order to assess whether the suggested biological heterogeneity of bipolar disorder may be due to genetic heterogeneity, we examined whether the age-at-onset subgroups aggregated in these bipolar disorder families. Using a proband predictive model, we showed that affected siblings of early-onset probands were over four times more likely than others to have an early onset as well, even after we controlled for age at contact, which was highly correlated with the self-reported age at onset in this sample. Several previous studies have reported similar observations, which suggests that age at onset aggregates in families. Such findings are consistent with the notion that age at onset is a heritable trait within bipolar disorder reflecting the underlying genetic heterogeneity of the disorder. However, it should be noted that the findings do not prove this, since familial aggregation may be due to nongenetic as well as genetic factors.
We further noted that siblings of early-onset probands tended to have higher risks of certain psychiatric disturbances, including alcoholism, drug abuse, and suicidality. It is interesting that several previous studies also found that these same disturbances occurred more frequently in relatives of early-onset subjects
(19,
28–30). Because our results were most compelling with drug abuse, we sought to examine more closely the evidence that it co-aggregates with age at onset in our families. Using a modification of the proband-predictive model, we found that siblings of probands with an age at onset <21 were over 10 times more likely to have drug abuse problems than siblings of probands with an age at onset >28. This association persisted even after we controlled for age at onset in the siblings and drug abuse in the probands, which could confound the relationship. In contrast to our other findings, the siblings of probands with ages at onset between 22–28 were more similar to the early-onset than the late-onset groups. It is unclear why this is the case. Nevertheless, the findings suggest age at onset and drug abuse may share a common genetic etiology that warrants further investigation.
The current study has several limitations. Most notably, age at onset was assessed by retrospective self-report. The most accurate way to assess age at onset would be to prospectively follow normal subjects until they develop bipolar disorder. However, this is impractical in most situations. By default, the next best approach is self-report. The quality of such data is potentially degraded by recall or information bias. Indeed, it is arguable whether subjects can accurately tell whether their disorder started when they were 16 or 18 years old. Consequently, the true variation in age at onset of bipolar disorder may not be validly captured by a self-reported continuous variable. It seems more reasonable to assume that subjects are better able to distinguish whether their disorder started when they were 16 versus 30 years old. In this case, capturing age at onset in broad categories may be the best that can be validly differentiated.
The difficulty with a categorical variable is determining where to make the cutoff points between age-at-onset subgroups. Previous studies have used a variety of cutoff points
(10,
15,
31), often with little justification. We decided to empirically define the cutoff points using the “points of rarity” in the observed age-at-onset distribution. Such an approach has a certain intuitive appeal, but it too may lead to misclassification of subjects, especially among those who have an age at onset where the subgroups may overlap. Misclassification of this sort would tend to introduce noise into the analyses and likely bias observed associations toward the null. Despite this, we were still able to observe robust patterns of differences between the age-at-onset subgroups.
The current study also has several important strengths. The families used in this study were ascertained through a common set of criteria, and the subjects were all assessed with the Diagnostic Interview for Genetic Studies, a widely used and well-validated instrument that collects information on a wide range of psychopathology. Furthermore, diagnoses of mood disorders and other comorbid conditions were assigned by experienced clinicians using best estimate procedures, thus minimizing concerns about misclassification of affection status. Finally, the study group was sufficiently large to allow examination of a variety of hypotheses related to the clinical and familial features of age at onset in bipolar disorder.
In summary, we found that 1) the distribution of age at onset in bipolar disorder revealed several subgroups of patients, 2) the clinical presentation varied significantly across these subgroups, and 3) the subgroups aggregated within families. These results, which are consistent with several other lines of evidence, provide further support for the conclusion that variation in age at onset is an important clinical marker of the underlying genetic heterogeneity in bipolar disorder. Thus, age at onset may conceivably be used to identify more homogeneous groups of bipolar disorder families and thereby facilitate the mapping of bipolar disorder susceptibility genes. Some investigators have started to consider age at onset in genetic studies of bipolar disorder
(32–
34), but the current findings suggest further investigation is warranted. Finally, our novel finding that drug abuse may co-aggregate with early age at onset requires further investigation.