Combined Cognitive Remediation and Functional Skills Training for Schizophrenia: Effects on Cognition, Functional Competence, and Real-World Behavior
Abstract
Objective:
Method:
Results:
Conclusions:
Method
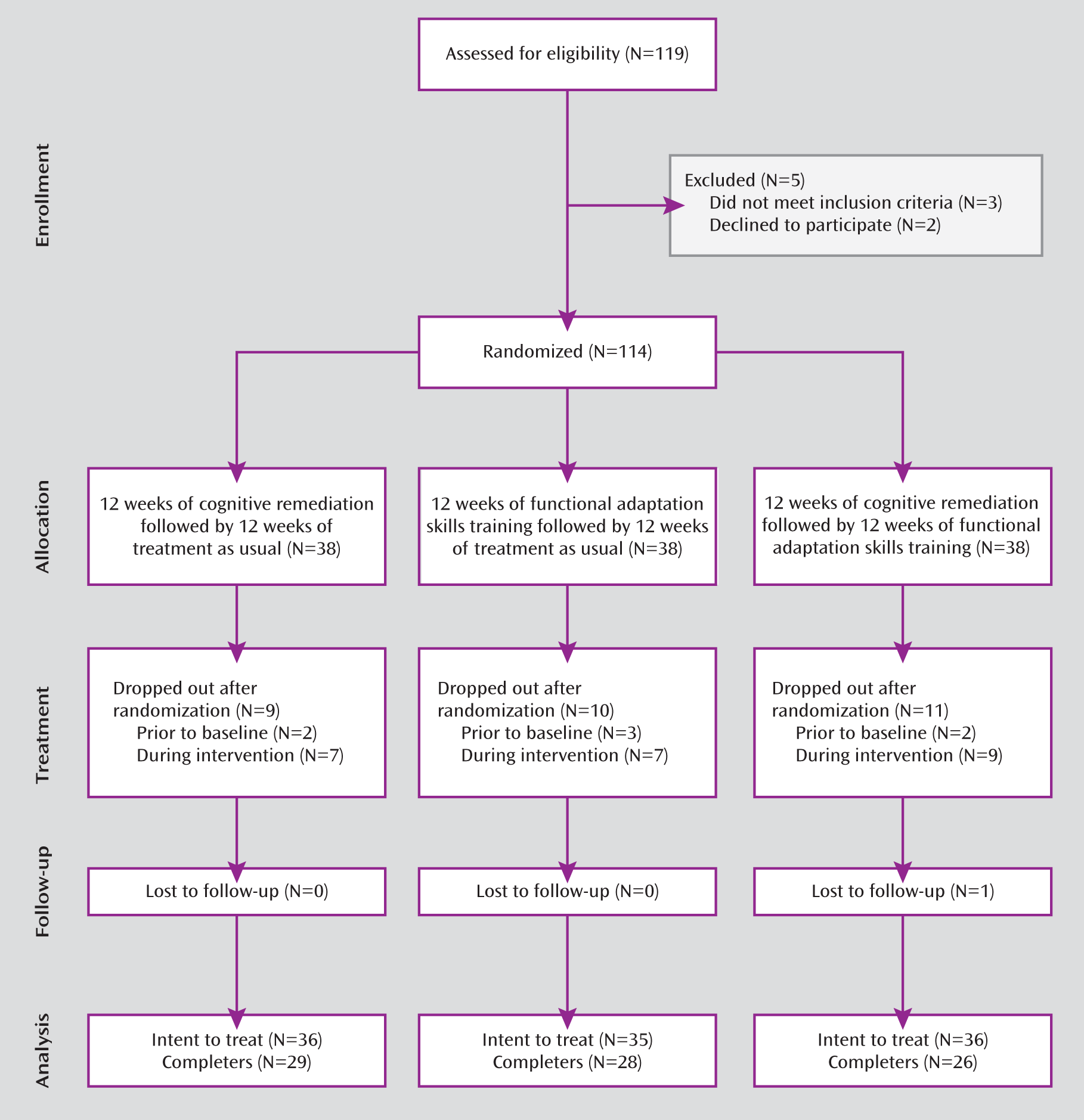
Participants
Measures
Cognition.
Clinical symptoms.
Social competence.
Functional competence.
Real-world functional behavior.
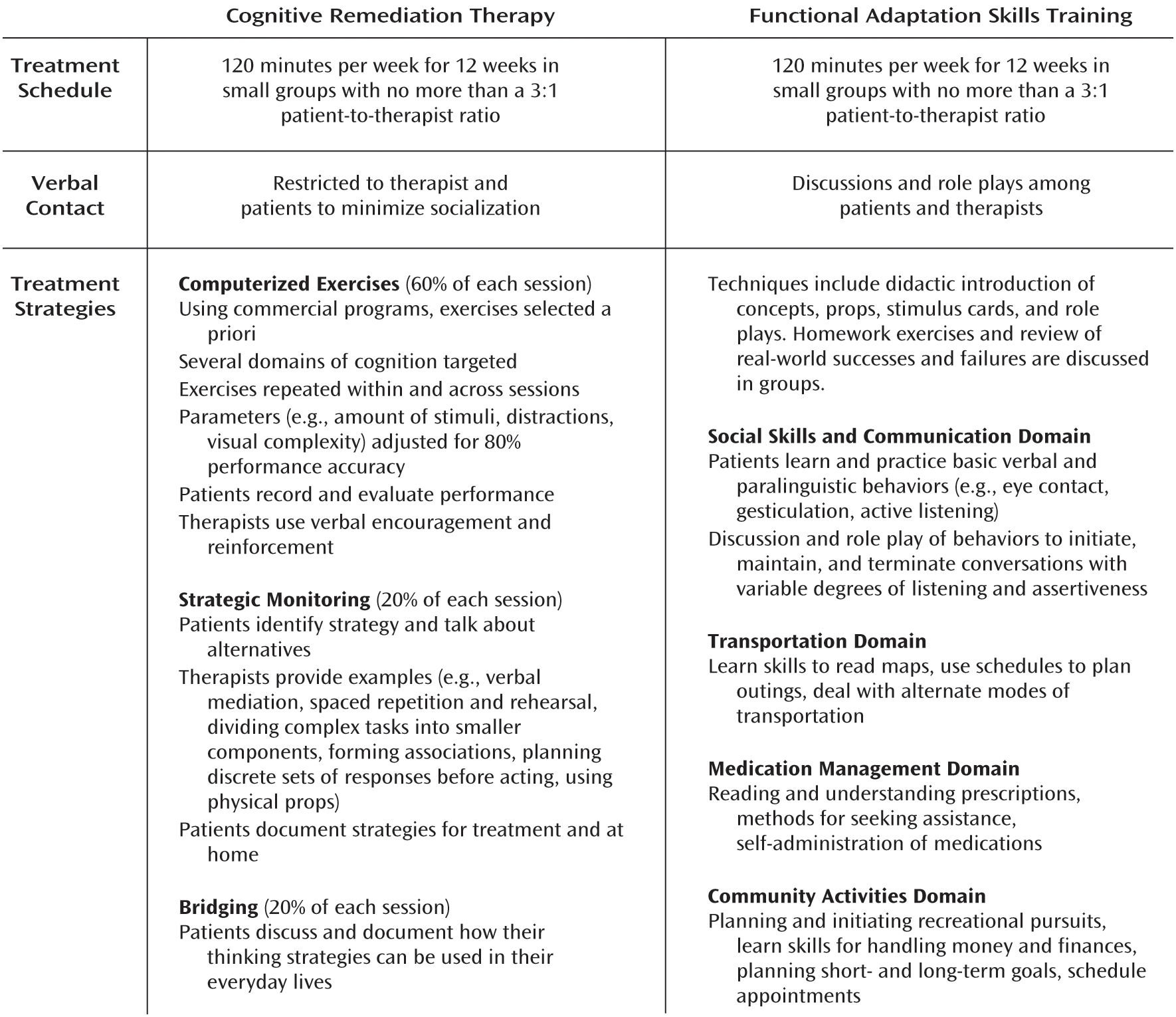
Treatment
Data Analysis
Results
Baseline Analyses
| Cognitive Remediation (N=36) | Functional Adaptation Skills Training (N=35) | Combined Treatment (N=36) | ||||
|---|---|---|---|---|---|---|
| Characteristic | Mean | SD | Mean | SD | Mean | SD |
| Age (years) | 39.1 | 10.5 | 42.7 | 9.7 | 39.9 | 8.5 |
| Education (years) | 13.3 | 1.8 | 13.1 | 1.7 | 12.9 | 1.1 |
| Wide-Range Achievement Test reading score | 44.5 | 4.3 | 44.6 | 4.7 | 46.1 | 5.2 |
| Age at first hospitalization (years) | 21.4 | 3.9 | 19.8 | 8.4 | 19.9 | 6.7 |
| Total time institutionalized (months) | 38.5 | 40.8 | 31.2 | 57.2 | 43.7 | 46.7 |
| Time since last hospitalization (months) | 50.8 | 57.0 | 61.9 | 64.0 | 39.7 | 51.0 |
| Time in current outpatient treatment (months) | 80.6 | 84.0 | 72.9 | 74.0 | 87.6 | 89.0 |
| Case management visits per monthb | 2.9 | 2.5 | 3.3 | 3.0 | 3.2 | 2.9 |
| Cognitive Remediation | Functional Adaptation Skills Training | Combined Treatment | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline (N=36) | Endpoint (N=29) | Baseline (N=35) | Endpoint (N=28) | Baseline (N=36) | Endpoint (N=26) | |||||||
| Medication Class | N | % | N | % | N | % | N | % | N | % | N | % |
| Atypical antipsychotic | 33 | 92 | 29 | 100 | 32 | 91 | 25 | 89 | 32 | 89 | 23 | 90 |
| Conventional antipsychotic | 3 | 8 | 0 | 0 | 5 | 14 | 3 | 11 | 4 | 11 | 3 | 10 |
| Benzodiazepine | 5 | 14 | 3 | 10 | 3 | 8 | 2 | 7 | 4 | 11 | 2 | 8 |
| SSRI | 10 | 28 | 5 | 17 | 5 | 14 | 3 | 11 | 4 | 11 | 2 | 8 |
| Lithium | 2 | 5 | 1 | 3 | 2 | 6 | 1 | 4 | 1 | 3 | 1 | 4 |
Intent-to-Treat Analysis
| Baseline | End of Active Treatment | 12 Weeks After End of Active Treatment | ||||||
|---|---|---|---|---|---|---|---|---|
| Measurea and Treatment Group | EMMb | SE | EMMb | SE | Cohen's dc | EMMb | SE | Cohen's dd |
| Brief Assessment of Cognition in Schizophrenia | ||||||||
| Composite score (z-score) | ||||||||
| Cognitive remediation | –1.60 | 0.15 | –0.90 | 0.15 | 0.77 | –0.88 | 0.15 | 0.72 |
| Functional skills training | –1.54 | 0.15 | –1.45 | 0.15 | 0.05 | –1.43 | 0.15 | 0.12 |
| Combined treatment | –1.70 | 0.15 | –1.01 | 0.15 | 0.73 | –1.12 | 0.14 | 0.71 |
| Adaptive composite (% of total) | ||||||||
| Cognitive remediation | 60.0 | 2.9 | 65.5 | 2.9 | 0.25 | 63.9 | 3.0 | 0.13 |
| Functional skills training | 60.8 | 2.9 | 68.5 | 2.9 | 0.51 | 65.9 | 3.0 | 0.41 |
| Combined treatment | 57.3 | 2.8 | 69.6 | 2.8 | 0.63 | 71.8 | 3.0 | 0.71 |
| Social Skills Performance Assessment total score (% of total) | ||||||||
| Cognitive remediation | 68.4 | 2.1 | 71.2 | 2.0 | 0.16 | 69.6 | 2.1 | 0.07 |
| Functional skills training | 69.2 | 2.2 | 76.9 | 2.0 | 0.52 | 76.1 | 2.1 | 0.60 |
| Combined treatment | 68.9 | 2.1 | 76.2 | 2.0 | 0.67 | 76.5 | 2.1 | 0.59 |
| Specific Levels of Functioning Scale | ||||||||
| Interpersonal subscale (% of total) | ||||||||
| Cognitive remediation | 57.3 | 2.4 | 58.5 | 2.4 | 0.12 | 55.5 | 2.3 | –0.08 |
| Functional skills training | 55.3 | 2.4 | 57.1 | 2.3 | 0.22 | 57.4 | 2.2 | 0.25 |
| Combined treatment | 53.5 | 2.2 | 55.5 | 2.2 | 0.21 | 54.9 | 2.4 | 0.15 |
| Community activities subscale (% of total) | ||||||||
| Cognitive remediation | 77.3 | 1.7 | 79.4 | 1.8 | 0.13 | 80.3 | 1.8 | 0.18 |
| Functional skills training | 78.8 | 1.7 | 81.1 | 1.7 | 0.21 | 81.0 | 1.7 | 0.17 |
| Combined treatment | 75.9 | 1.7 | 78.7 | 1.7 | 0.36 | 81.1 | 1.7 | 0.46 |
| Work skills subscale (% of total) | ||||||||
| Cognitive remediation | 73.8 | 2.3 | 75.8 | 2.4 | 0.19 | 75.0 | 2.4 | 0.14 |
| Functional skills training | 67.4 | 2.2 | 71.1 | 2.2 | 0.25 | 71.4 | 2.2 | 0.29 |
| Combined treatment | 71.7 | 2.2 | 79.1 | 2.3 | 0.44 | 85.8 | 2.3 | 0.92 |
| Positive and Negative Syndrome Scale | ||||||||
| Negative symptoms (mean item score) | ||||||||
| Cognitive remediation | 2.7 | 0.13 | 2.7 | 0.13 | 0.05 | 2.8 | 0.13 | 0.08 |
| Functional skills training | 2.4 | 0.13 | 2.3 | 0.13 | –0.03 | 2.2 | 0.13 | –0.11 |
| Combined treatment | 2.7 | 0.13 | 2.6 | 0.12 | –0.14 | 2.6 | 0.12 | –0.13 |
| Positive symptoms (mean item score) | ||||||||
| Cognitive remediation | 2.3 | 0.13 | 2.2 | 0.16 | –0.10 | 2.3 | 0.14 | –0.04 |
| Functional skills training | 2.6 | 0.12 | 2.8 | 0.14 | 0.12 | 2.6 | 0.12 | 0.02 |
| Combined treatment | 2.4 | 0.12 | 2.3 | 0.15 | –0.08 | 2.3 | 0.13 | –0.07 |
Discussion
Acknowledgments
Footnotes
References
Information & Authors
Information
Published In


History
Authors
Funding Information
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).