Losing a close relative in childhood may cause mental health problems (
1,
2). An estimated 5%−10% of children and adolescents experience depression, posttraumatic stress disorder (PTSD), and/or prolonged grief disorder following bereavement (
3). Prolonged grief disorder, newly included in ICD-11 (
4), involves persistent separation distress (e.g., yearning, preoccupation) and accompanying symptoms (e.g., avoidance, anger, difficulties moving on) that are present to a disabling and distressing degree beyond the first 6 months of bereavement. The condition resembles persistent complex bereavement disorder, which is included in section III (“Emerging Measures and Models”) of DSM-5 (
5), although there is evidence that ICD-11 prolonged grief disorder yields higher prevalence rates than DSM-5 persistent complex bereavement disorder in children and adolescents (
6) and in adults (
7), because ICD-11 prolonged grief disorder requires fewer symptoms to establish the diagnosis.
There is accumulating evidence that in adults and children/adolescents alike, prolonged grief disorder (with separation distress as the key symptom) is distinct from—and conveys functional impairment beyond—bereavement-related PTSD (the key symptoms of which are fear, reexperiencing, and hypervigilance) and depression (characterized by low mood and anhedonia) and has specific maintaining mechanisms (
8,
9). Therefore, psychological interventions are needed that specifically target prolonged grief disorder. There is little knowledge about treatments successfully alleviating prolonged grief disorder in children and adolescents. Over a decade ago, meta-analytic reviews (
10,
11) indicated that interventions for bereaved children and adolescents were moderately successful and lacked a clear theoretical basis, and that studies evaluating interventions were limited because they mostly evaluated changes in general distress rather than in disturbed grief and had poor methodology (e.g., absence of control group, nonrandom assignment to conditions).
More recently, several lines of research have enhanced knowledge in this area. First, seminal research on the Family Bereavement Program (FBP) has shown that immediate and long-term emotional problems in children and adolescents confronted with parental loss can be effectively prevented by improving family-level (e.g., parenting skills) and child-level (e.g., coping skills) processes (
12). Second, research evaluating trauma and grief component therapy—a group treatment for adolescents confronted with loss during civil war—has shown that this approach effectively reduces grief, depression, and anxiety symptoms (
13). Third, uncontrolled studies (
14,
15) have indicated that cognitive-behavioral therapy for childhood traumatic grief, targeting both traumatic stress and grief following unnatural deaths, successfully alleviates disabling grief. More recently, an uncontrolled pilot study showed that multidimensional grief therapy yielded promising effects (
16).
Notwithstanding the importance of the treatments that have been developed so far, they are limited in their focus on prevention (e.g., FBP), their reliance on group-based formats (e.g., FBP, trauma and grief component therapy), and their focus on specific groups (parentally [e.g., FBP] or traumatically [e.g., trauma and grief component therapy, cognitive-behavioral therapy for childhood traumatic grief] bereaved children and adolescents) (
17,
18). In adults, CBT is a promising treatment for reducing prolonged grief disorder and associated psychopathology (
19–
21). An understanding of whether CBT is effective in treating childhood prolonged grief disorder is needed. In the present study, we tested CBT Grief-Help, a manualized individual treatment for prolonged grief disorder in bereaved children and adolescents who are confronted with natural or unnatural deaths, combined with parental counseling. As described in the study protocol (
22), CBT Grief-Help was compared with supportive counseling. We expected CBT Grief-Help to yield greater reduction of prolonged grief disorder symptoms and other symptoms at posttreatment and follow-up assessments compared with supportive counseling.
Methods
Patients
Patients were recruited from eight outpatient clinics in the Netherlands from 2010 through 2015. Patients were self-referred or referred by local professionals. Inclusion criteria were age between 8 and 18 years; loss of a close relative; distressing and disabling prolonged grief disorder symptoms as the primary problem and reason for seeking treatment; no intellectual disability, developmental disorders, or severe conduct disorder; no concurrent psychological/psychopharmacological treatment; and, among participating children and adolescents as well as their parents or caretakers, no current substance abuse or dependence, psychotic symptoms, or severe depression with risk of suicide.
Procedure
Ethical approval for the study was obtained from an independent medical ethics committee (Central Committee on Research Involving Human Subjects, no. NL30528.041.09), and we followed CONSORT guidelines for reporting on this randomized controlled trial. Participants underwent an intake interview following standard procedures at their institution to screen for conduct, developmental, and substance use disorders and to assess other inclusion and exclusion criteria. After eligible children and adolescents and their parents or caretakers were informed about the study, written informed consent was obtained from parents and caretakers and assent or consent was obtained from the children and adolescents, depending on their age. Next, patients and their parents or caretakers completed pretreatment measures in the presence of a therapist. This included the administration of the Inventory of Prolonged Grief for Children (IPG-C), on which participants had to have a score >40 to be enrolled in the study. Care as usual was offered for patients whose IPG-C scores were lower. After completion of pretreatment measures, participants were assigned in a 1:1 ratio, by computer-generated simple randomization, to CBT Grief-Help or supportive counseling. Additional assessments were conducted at the completion of treatment and at 3-, 6-, and 12-month follow-ups. For posttreatment assessments, participants completed the self-report questionnaires during telephone calls with trained master’s-level assistants who read the questions out loud and provided further explanation as needed.
Primary Outcome Measure
The Inventory of Prolonged Grief for Children (IPG-C), a 30-item child/adolescent version of the Inventory of Complicated Grief (
23), measures prolonged grief disorder symptoms as described by Prigerson et al. (
24) and other symptoms of disturbed grief. Respondents rate past-month symptom frequency on a 3-point scale (1=almost never, 2=sometimes, 3=always). A score >40 indicates clinically relevant prolonged grief disorder.
Secondary Outcome Measures
Children’s Depression Inventory (CDI).
The CDI is a 27-item measure of depression (
25). Each item contains three statements representing depressive symptoms at increasing severity, and respondents select the statement that best describes their state during the preceding week.
Child PTSD Symptom Scale (CPSS).
This 17-item measure (
26) taps DSM-IV PTSD symptoms (
27). Participants rated the occurrence of symptoms with the loss as the anchor event (e.g., “Having upsetting thoughts or images about the event that came into your head when you didn’t want them to”) on a 4-point scale (0=not at all/only once a week through 3=almost always/five or more times a week). We examined total PTSD severity, plus the severity of the DSM-IV-based clusters (reexperiencing, avoidance, and hyperarousal).
Child Behavior Checklist (CBCL).
The CBCL is a 118-item measure of emotional and behavioral problems completed by parents or caretakers (
28). Items (e.g., “trouble sleeping”) are rated on a 3-point scale (0=not true, 1=somewhat/sometimes true, 2=very true/often true). Scores can be used to obtain indices of internalizing problems, externalizing problems, and total problem behavior.
All questionnaire measures used in this study have sound psychometric properties for our sample’s age group (
23,
25,
26,
28).
Treatments
Participants received a maximum of nine individual 45-minute sessions of CBT Grief-Help or supportive counseling, planned for once every 1 or 2 weeks if possible. Five 45-minute sessions with parents or caretakers were planned in parallel with these nine sessions.
CBT Grief-Help.
CBT Grief-Help was delivered as described elsewhere (
17,
18). It is a manualized treatment based on a cognitive-behavioral model postulating that three processes maintain acute grief: insufficient integration of the loss with preexisting knowledge (fueling separation distress); rigid negative thinking about oneself, life, and one’s ability to deal with the loss; and a propensity to fear and avoid reminders of the loss (termed “anxious avoidance”) and to withdraw from normal routines and activities that could foster adjustment (“depressive avoidance”) (
29). CBT Grief-Help includes exposure interventions, including imaginary exposure (telling the story of the loss event, elaborating painful aspects), in vivo exposure (visiting the scene of the death), and writing (writing a letter to the lost person about what is missed most). Socratic questioning and behavioral experiments are used to curb maladaptive thinking. Patients are taught specific skills to replace maladaptive with helpful ways of coping.
The treatment was divided into five main parts, all described in a detailed client workbook. The first part of treatment (titled “Who died?”) invited participants to talk about the circumstances of the loss, what they missed, and what they wished they could still share with the lost person. This part encouraged confrontation with the reality of the loss and aided therapists in identifying possible maladaptive thinking and behavioral patterns. In the second part of treatment (“What is grief?”), adjustment to bereavement was explained as encompassing four tasks: facing the reality and pain of the loss; regaining confidence in yourself, other people, life, and the future; focusing on your own problems and not on those of others; and continuing activities that you used to enjoy. The third part (“Cognitive restructuring”) focused on task 2. In the fourth part (“Maladaptive behaviors”), exposure was used to address task 1, problem-solving skills were taught to address task 3, and behavioral activation was employed for task 4. In the fifth and final part of treatment (“Moving forward after loss”), skills learned were reviewed. During treatment, participants wrote three letters to an imaginary or real friend to summarize things learned.
Supportive counseling.
Supportive counseling is based on nondirective treatments for grief and PTSD in children and adolescents (
30,
31). As a rationale, it is explained that difficulties in recovery from loss may coincide with emotional, social, and practical problems and that talking about these problems could bring relief to, and improve coping skills to deal with, the consequences of bereavement. Participants are supported in sharing all the feelings and thoughts that they want, through talking, playing, or creative activities. Therapists are unconditionally supportive of issues that the participants bring up and their attempts at problem solving, without addressing cognitions and exposure. Supportive counseling was divided into three parts, also described in a client workbook. In the first part (with no predefined number of sessions), participants were invited to list problems and issues they faced since the loss. In the second part, therapists and participants reviewed these problems and issues in more detail, in a manner and at a pace they felt comfortable with. In the third part, they prepared for the ending of treatment.
Parental Counseling
The five parental counseling sessions aimed to help parents and caretakers in supporting their children during the therapeutic process. In the parental sessions paralleling CBT Grief-Help, the client workbook (describing CBT Grief-Help) was reviewed and maladaptive thinking and behavioral patterns that parents and caretakers thought blocked their children’s grief were discussed. Parents and caretakers were given assignments to spend more quality time with their child to strengthen the parent-child relationship. In the parental sessions paralleling supportive counseling, the client workbook (describing supportive counseling) was reviewed and themes on which the parents and caretakers wanted to reflect were listed. Therapists guided them in considering solutions for problems they encountered.
Therapists and Treatment Fidelity
Treatments were conducted by 30 licensed (post-master’s-level) therapists. All had received basic training in CBT and supportive counseling and had undergone 6 hours of training in CBT Grief-Help and supportive counseling (from M.S. and P.B.). When possible (depending on the number of children applying for help) therapists delivered both treatments. Different means were used to promote and evaluate treatment integrity. First, both treatments were described in detailed session-by-session protocols. Second, regular supervision sessions (with M.S.) were held to promote adherence to the protocols. From every therapy, one session was audiotaped (provided permission was given) and reviewed during supervision sessions to ensure, and discuss challenges with, adherence to the protocols. Third, therapists kept logbooks of all therapies, in which they rated how satisfied they were with their application of the interventions described in the protocols (on scales with anchors 1=unsatisfied, through 5=very satisfied); for all sessions, mean satisfaction scores did not differ significantly between the two conditions (all t values <1.53, all p values >0.13). Therapists were instructed to report particularities in the logbooks; no particularities pointing at deviations from the protocols were mentioned. In the CBT Grief-Help condition, therapists also rated the extent to which they achieved the goals described in the protocol (e.g., challenging unhelpful thoughts with questions and/or behavioral experiments, in sessions 4–5) on a 5-point scale (1=not at all, 2=a little, 3=fair, 4=a lot, 5=completely). For each of the nine sessions, goals were achieved at least “a little” in 87.0%−98.4% of the sessions.
Statistical Analysis
We based the sample size on calculations presented previously in the study protocol (
22). Analyses were conducted using SPSS (IBM, Armonk, N.Y.). Sociodemographic and loss-related variables and baseline symptom levels were compared between conditions using chi-square tests and analyses of variance. Treatment effects were evaluated using a prespecified multilevel modeling approach, following guidelines from Snijders and Bosker (
32). Missing data were handled with maximum likelihood functioning. First, a random-intercept-only model was built for each outcome measure to calculate the intraclass correlation, and then time was included as linear predictor in the model, followed by a model with dummy-coded time, using the pretreatment assessment as the reference category. The statistical fit of these two models (with categorical versus dummy-coded time) was compared. The model with the lowest Akaike information criterion was preferred. In addition, condition effects and time-by-condition interaction effects were added to the models. To examine whether inclusion of interaction effects improved model fit (compared with a model with main effects for time and condition only) we used deviance tests; these are based on the differences between the models in the −2 log likelihood values and accompanying difference in degrees of freedom, which has a chi-square distribution. Alpha was set at 0.05. Following recommendations (
32), we chose the most restrictive models for the random parts (i.e., models with the smallest number of parameters) and excluded random slopes when these were not significant. Effect sizes (Cohen’s d) were calculated for within- and between-group differences by dividing the unstandardized regression coefficient by the pooled standard deviation of the pretreatment score (
20,
33). These analyses were based on the intent-to-treat sample. At the pretreatment, posttreatment, 3-month follow-up, 6-month follow-up, and 12-month follow-up, a maximum of 4%, 3%, 2%, 5%, and 4% of item responses were missing, respectively. These missing data were replaced by the mean.
Next, for all participants, reliable change indices (RCIs) were calculated for changes in IPG-C scores from pretreatment to posttreatment and 3-, 6-, and 12-month follow-up assessments. We used Jacobson and Truax’s (
34) formula,
where
X2 represents a participant’s score at the posttreatment or 3-, 6-, or 12-month follow-up assessment,
X1 represents the score at the pretreatment assessment, and
Sdiff represents the standard error of the difference. We then counted the number of participants who showed reliable changes on the IPG-C (i.e., RCI >1.96). We used data from treatment completers to calculate the number needed to treat (NNT) as 1/(proportion of participants responding in CBT Grief-Help − proportion responding in supportive counseling). We calculated four NNTs, comparing pretreatment with posttreatment, 3-month, 6-month, and 12-month follow-up assessments, respectively, with treatment response defined as reliable changes on the IPG-C. The NNT provides an estimate of the number of children and adolescents who would need to receive CBT Grief-Help instead of supportive counseling to get one additional response (
35,
36).
Lastly, we explored whether changes in the primary outcome measure (IPG-C) were moderated by gender (0=boy, 1=girl), age (in years), time since loss (in months), relationship with the deceased (0=other than parent, 1=parent), and cause of death (0=illness, 1=unexpected/violent cause). For each moderator, a separate model was run that included the main effect of the moderator plus the interaction terms between that moderator, condition, and time.
Results
Sample Characteristics and Retention
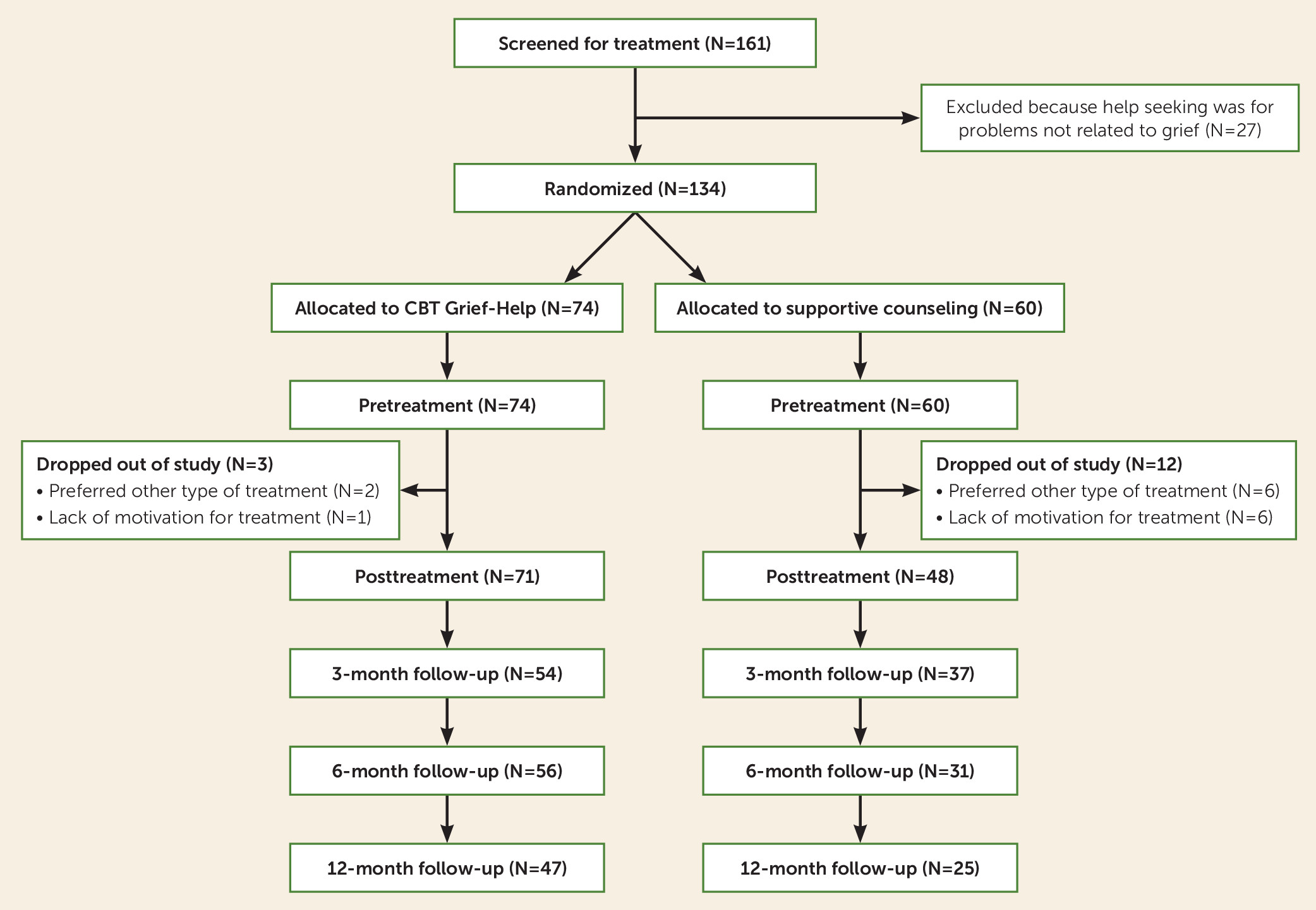
Figure 1 illustrates the flow of participants through the study. In total, 161 children and adolescents completed the pretreatment assessment. Of these, 27 were excluded because prolonged grief disorder symptoms were not the primary problem and reason for seeking treatment, and 134 underwent randomized assignment to CBT Grief-Help (N=74) or supportive counseling (N=60). The two randomized groups did not differ in sociodemographic or loss-related variables, or prolonged grief disorder, depression, and PTSD symptom severity at the pretreatment assessment (
Table 1). No adverse effects of treatments were reported. Three participants dropped out of the CBT Grief-Help group and 12 dropped out of the supportive counseling group, for different reasons (
Figure 1). The dropout rate was higher in the supportive counseling group (20.0%) compared with the CBT Grief-Help group (4.1%; Fisher’s exact test, p=0.005). Participants who dropped out did not differ significantly from those who continued treatment in baseline sample characteristics, except that the former group had higher baseline depression (p=0.003). Therefore, pretreatment depression was included as covariate in multilevel analyses. From the posttreatment to the 12-month follow-up assessment, 47 participants dropped out—32 because they started a different treatment and 15 because they were unable or unwilling to complete follow-up measures.
Treatment Outcome Analyses
The models for prolonged grief disorder (Δ Akaike information criterion=158.75), depression (Δ Akaike information criterion=32.85), and PTSD (Δ Akaike information criterion=106.08) with dummy-coded time fit better than models with categorical time, and therefore models with dummy-coded time were retained. Random slopes were not significant and were excluded from the models.
Primary Outcome: Prolonged Grief Disorder Severity
Adding time-by-condition interaction effects to the model that only included main effects for baseline depression, time, and condition significantly improved model fit (Δχ
2 =20.05, df=4, p<0.001). Interaction terms were all significant, indicating that reductions in prolonged grief disorder severity were stronger for participants who received CBT Grief-Help compared with those who received supportive counseling.
Table 2 presents parameter estimates of the final model, and
Table 3 lists effect sizes for all outcome measures. Tables S1–S3 in the
online supplement list observed mean scores for each measurement occasion.
The percentages of participants in the CBT Grief-Help and supportive counseling groups, respectively, who showed a reliable change on the IPG-C were 76.1% and 57.4% from pretreatment to posttreatment assessment, 72.2% and 54.1% from pretreatment to 3-month follow-up assessment, 71.4% and 54.8% from pretreatment to 6-month follow-up assessment, and 78.6% and 60.0% from pretreatment to 12-month follow-up assessment. Using these numbers, the NNTs were 5.37 for pretreatment versus posttreatment assessment, 5.52 for pretreatment versus 3-month follow-up assessment, 6.02 for pretreatment versus 6-month follow-up assessment, and 5.34 for pretreatment versus 12-month follow-up assessment.
Secondary Outcomes
Depression severity.
Adding time-by-condition interaction effects to the model including only main effects significantly improved the model fit (Δχ
2=10.45, df=4, p<0.05). Reductions in depression were greater in the CBT Grief-Help group compared with the supportive counseling group from pretreatment to 6-month follow-up assessment and from pretreatment to 12-month follow-up assessment, but not from pretreatment to posttreatment assessment or from pretreatment to 3-month follow-up assessment (
Table 2).
PTSD severity.
Adding time-by-condition interaction effects improved model fit compared with a model including only main effects, but fell short of statistical significance (Δχ
2=8.83, df=4, p<0.10). Reductions in PTSD were larger for participants in the CBT Grief-Help group from pretreatment to 6-month follow-up assessment and from pretreatment to 12-month follow-up assessment, but not from pretreatment to posttreatment assessment or pretreatment to 3-month follow-up assessment (
Table 2).
For PTSD clusters, 65.7%, 73.0%, and 64.9% of the variance in reexperiencing, avoidance, and hyperarousal, respectively, was at level 1 and 34.3%, 27.0%, and 35.1% at level 2. Compared with models including main effects only, adding time-by-condition interaction effects significantly improved the fit of the model for reexperiencing (Δχ2=11.40, df=4, p<0.01), but not avoidance (Δχ2=3.26, df=4, p>0.05) and hyperarousal (Δχ2=7.32, df=4, p>0.05). Table S4 in the online supplement shows that CBT Grief-Help more strongly reduced reexperiencing from pretreatment to 3-month, 6-month, and 12-month follow-up assessments.
Parent/caretaker-rated internalizing, externalizing, and total problem behavior.
Table 4 summarizes the outcomes for CBCL scores. For CBCL internalizing behaviors, adding time-by-condition interaction effects to the models with only main effects significantly improved the model fit (Δχ
2=15.01, df=4, p<0.01). Reductions in internalization were stronger for participants in the CBT Grief-Help group compared with those in the supportive counseling group for all comparisons except pretreatment versus posttreatment assessment. For CBCL externalizing behaviors, adding time-by-condition interaction effects to the models with main effects did not improve model fit (Δχ
2=7.37, df=4, p>0.05). For CBCL total scores, again, adding time-by-condition interaction effects to the models with main effects did not improve fit (Δχ
2=8.63, df=4, p>0.05).
Moderators of Treatment Effects
For prolonged grief disorder, we found that age moderated treatment effects for pretreatment versus posttreatment assessment (B=0.36, SE=0.17; t=2.08, df=404.28, p=0.039) and for pretreatment versus 3-month follow-up assessment (B=0.48, SE=0.19; t=2.52, df=411.53, p=0.012), such that older participants benefited more from CBT Grief-Help (compared with supportive counseling) than younger participants. Moderation effects were also found for kinship, for pretreatment versus posttreatment assessment (B=2.84, SE=1.06; t=2.68, df=407.75, p=0.008), pretreatment versus 3-month follow-up assessment (B=4.28, SE=1.21; t=3.52, df=411.17, p<0.001), pretreatment versus 6-month follow-up assessment (B=3.85, SE=1.22; t=3.17, df=418.25, p=0.002), and pretreatment versus 12-month follow-up assessment (B=5.09, SE=1.25; t=4.06, df=419.07, p<0.001); participants who lost a parent benefited more from CBT Grief-Help (compared with supportive counseling) than those who lost another relative. No moderation effects for gender, time since loss, and cause of death were found. Tables S5–S9 in the online supplement include all models for all moderation analyses.
Discussion
We compared CBT Grief-Help with supportive counseling for bereaved children and adolescents with disabling prolonged grief disorder symptoms. To our knowledge, this is the largest randomized controlled trial to date in this population and the first to compare two active treatments (
10,
11). A main finding was that CBT Grief-Help led to significantly greater improvements in prolonged grief disorder symptoms from pretreatment assessment to posttreatment assessment and 3-, 6-, and 12-month follow-up assessments. Effect sizes were small to medium for between-group comparisons. The findings complement evidence from uncontrolled studies (
17,
18) and mirror evidence that CBT effectively reduces prolonged grief disorder in adults (
19–
21). Although mechanisms of change are still to be researched, it is conceivable that CBT Grief-Help more effectively alleviates prolonged grief disorder by yielding positive changes in negative thinking patterns, decreasing maladaptive coping, increasing pleasant activities, and strengthening social problem-solving skills. In addition, whereas supportive counseling leaves room to avoid the reality of the loss and associated feelings, CBT Grief-Help encourages emotional processing of this reality.
Interestingly, whereas improvements in prolonged grief disorder were consistently stronger for participants assigned to CBT Grief-Help from pretreatment to all posttreatment assessments, improvements in depression symptoms and PTSD symptoms differed between the two conditions only when comparing changes from pretreatment to 6- and 12-month follow-up assessments. Changes in parent-rated outcomes present a similar picture: from pretreatment to posttreatment assessment, parents or caretakers reported equal improvements in functioning in both conditions, with moderate effect sizes. Beyond the posttreatment assessment, declines in internalizing problems were rated as steeper for participants in the CBT Grief-Help group. This indicates that, in terms of child-rated depression and PTSD symptoms and parent/caretaker-rated internalizing problems, CBT Grief-Help does not outperform supportive counseling in the short run but does yield better long-term effects. This echoes evidence supporting the long-term effectiveness of CBT for children’s anxiety, depression, and traumatic stress (
37). It is conceivable that skills learned during CBT Grief-Help confer protection to the sequalae of the loss after the termination of treatment and thus have considerable incremental value beyond nondirective therapeutic support.
Dropout rates were higher in the supportive counseling group than in the CBT Grief-Help group. This indicates that explicitly addressing thoughts, feelings, and memories connected with the loss is acceptable for children and adolescents and may in fact be more tolerable than exploring one’s experiences without being guided in a specific direction. Although there still exists some reluctance to apply CBT interventions in children and adolescents, the present findings accord with theorizing and research indicating that this reluctance is not justified (
38).
Although CBT Grief-Help was superior to supportive counseling, both treatments were associated with large reductions in prolonged grief disorder severity. Research on psychological treatments for bereaved children and adolescents has so far focused exclusively on group-based rather than individual treatments (e.g.,
12) and on specific groups (e.g., traumatically and/or parentally bereaved children or adolescents; e.g.,
13). The present findings contribute to this literature by showing that relatively brief treatments employing conventional CBT and nondirective interventions achieve positive treatment gains.
Several limitations of the study must be considered. First, although different methods were used to evaluate treatment integrity, and altogether they indicated that therapists implemented the protocols as intended, we did not use independent rating of treatment integrity (e.g., with independent raters scoring tapes of sessions). Second, both treatments were implemented with carefully prepared and well-conceived rationales, manuals, and supervision. However, although our monitoring of treatment fidelity did not produce any indication of it, we cannot rule out the possibility that the credibility of the treatments was experienced differently between treatments or that therapists identified more with one of the treatments than the other. Third, the extent to which treatment effects were affected by parental counseling and parent characteristics (e.g., adjustment levels) remains unknown. Fourth, we were unable to disentangle which elements of CBT Grief-Help and supportive counseling yielded the strongest effects; dismantling studies are needed to clarify that. Lastly, because our study started before DSM-5 was published, caution should be applied in generalizing the outcomes to DSM-5-based disorders. Although clinical interviews tapping disturbed grief as defined in DSM-5 and ICD-11 are still to be developed, it is recommended that they be used in future studies, once available.
Bereavement may have significant health consequences, in adults and children alike. The novelty of this study is that it provides evidence that disturbed grief can be successfully reduced using clearly defined CBT interventions. The promising long-term effects of CBT Grief-Help relative to supportive counseling suggest that CBT successfully strengthens children and adolescents in facing the challenges brought about by bereavement. Considering that many bereaved children and adolescents who need help likely receive no treatment, or no evidence-based treatment (
10,
11), disseminating CBT Grief-Help is a key challenge for bereavement care. There is recent evidence that similar interventions for children and adolescents who experienced parental death can be successfully delivered by lay counselors in lower-resource areas (
39). The specifically described protocol of CBT Grief-Help potentially allows a similar delivery by a variety of caretakers.
Acknowledgments
The authors thank Elise Bakker, Kim Idenburg, and Jolanda Zijderlaan for their help with the collection of data, and Mirjam Moerbeek for statistical advice.