Defining Recovery From Alcohol Use Disorder: Development of an NIAAA Research Definition
Abstract
Importance of Defining Recovery
| Primary Source | Year Disseminated | Abstinence Focused | Alcohol Specific | DSM-5 Remission Included | Well-Being Constructs Included | Description of Recovery Definition |
|---|---|---|---|---|---|---|
| Betty Ford Clinic | 2007 | Yes | No | No | Yes | A voluntarily maintained lifestyle characterized by sobriety, personal health, and citizenship |
| Substance Abuse and Mental Health Services Administration | 2012 | Yes | No | No | Yes | A process of change through which individuals improve their health and wellness, live a self-directed life, and strive to reach their full potential |
| Recovery Science Research Collaborative | 2017 | No | No | No | Yes | An individualized, intentional, dynamic, and relational process involving sustained efforts to improve wellness |
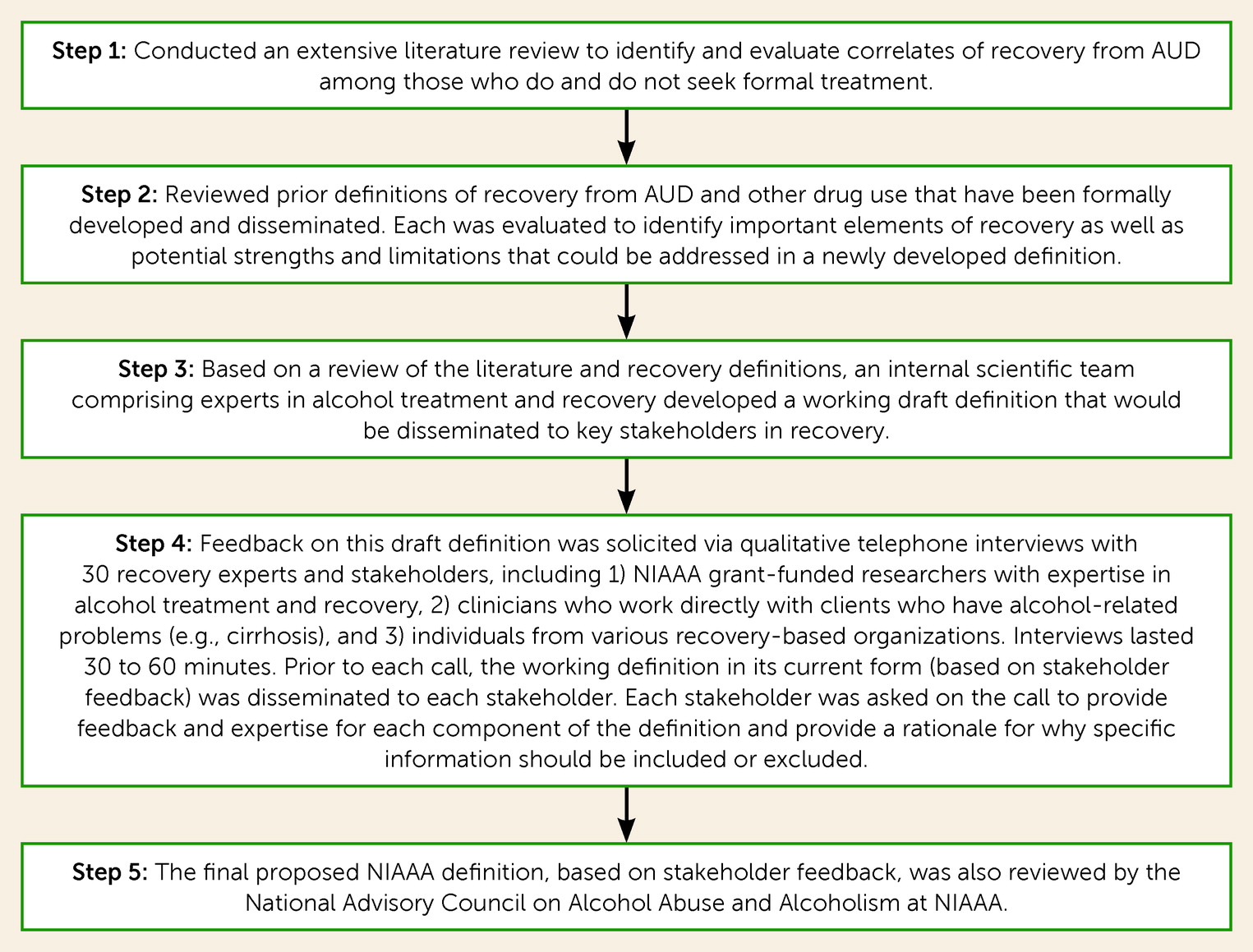
Methodology for Developing NIAAA Recovery Definition
The Final NIAAA Definition of Recovery From DSM-5 AUD

NIAAA Definition of Recovery
“Recovery is a process through which an individual pursues both remission from AUD and cessation from heavy drinking. Recovery can also be considered an outcome such that an individual may be considered ‘recovered’ if both remission from AUD and cessation from heavy drinking are achieved and maintained over time. For those experiencing alcohol-related functional impairment and other adverse consequences, recovery is often marked by the fulfillment of basic needs, enhancements in social support and spirituality, and improvements in physical and mental health, quality of life, and other dimensions of well-being. Continued improvement in these domains may, in turn, promote sustained recovery.”
Component 1: Definition of Remission From DSM-5 AUD
“Remission from alcohol use disorder (AUD), as defined by DSM-5 criteria, requires that the individual not meet any AUD criteria (excluding craving). Remission from AUD is categorized based on its duration: initial (up to 3 months), early (3 months to 1 year), sustained (1 to 5 years), and stable (greater than 5 years).”
Component 2: Definition of Cessation From Heavy Drinking
“Cessation from heavy drinking is defined as drinking no more than 14 standard drinks per week or 4 drinks on a single day for men and no more than 7 drinks per week or 3 drinks on a single day for women. Cessation from heavy drinking can be categorized based on the duration: initial (up to 3 months), early (3 months to 1 year), sustained (1 to 5 years), and stable (greater than 5 years).”
Primary Components of Recovery from AUD: Elaboration and Importance
Component 1: Remission From DSM-5 AUD in Recovery
Component 2: Cessation From Heavy Drinking in Recovery
Component 3: Biopsychosocial Functioning and Quality of Life in Recovery
Concluding Remarks
Supplementary Material
- View/Download
- 82.84 KB
References
Information & Authors
Information
Published In


History
Keywords
Authors
Funding Information
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).