Introduction
On May 25, 2020, George Floyd was killed in Minnesota by police officers.
1 The Minneapolis Police have cited that he was intoxicated, agitated, and resisting arrest.
1 The bystander video footage shows Mr. Floyd being killed brutally on the scene under physical restraints.
2 Imagine, instead, if the scenario had developed differently: The paramedics, accompanied by police, bring in a middle-aged Black man for “agitation and intoxication” to a busy emergency department (ED). He is cuffed to the gurney, struggling with the restraints, and screaming to be released. Would medical professionals treat him as every other patient, regardless of race?
This scenario, in which an individual is determined to be agitated by authorities and placed in restraints, is not uncommon in EDs across the country. In fact, agitation is a routine and increasingly frequent presentation, with 1.7 million events occurring annually in U.S. EDs,
3 representing 2.6% of all presentations.
4 Restraints, whether chemical or physical, were used in the management of over 80% of these cases, impacting over 2% of all ED patients.
4 While the racial breakdown of restraint use is not clearly understood on a systemic scale, racial biases are generally well documented in the medical system and likely influence how agitation is managed in the ED.
5–7 Several recent regional studies have found that Black patients were 13% to 22% more likely to be restrained when compared to White patients, suggesting racial differences in chemical and physical restraint use.
5–7Although agitation is a common occurrence, the specific clinical scenarios can be as unique as the patients themselves. The management can be nuanced, oftentimes aimed at addressing potential threats of violence for staff as well as other patients.
8 In fact, compared to the general population, health care providers are at high risk of workplace violence, with 75% of all workplace violence incidents found in the health care field.
9 Compared to other health care specialties, emergency medicine practitioners are especially vulnerable.
10 As such, in these difficult scenarios of heightened emotions and desire for self-protection, biases may easily influence the management of agitation.
11In caring for the agitated patient, verbal deescalation is the preferred primary intervention.
12 However, when deescalation fails, providers may be required to employ physical and chemical restraints for patient and staff safety.
13 Although safety is a common rationale for the use of restraints, they are not without potential harm. Restraints, both chemical and physical, can result in serious complications, including asphyxiation and death.
4,14,15 Aside from potential physical risks, restraints can have lasting psychological effects as well.
16 During interviews discussing their ED experiences, patients reported feeling dehumanized and a loss of dignity.
16 Restraint experiences also resulted in lasting patient mistrust and future avoidance of the health care system.
16 To reach the decision to restrain, the individual provider must weigh these potential harms against the need to ensure safety, all while under significant situational and time pressure.
Mr. Floyd's death incited protests across the nation, inspiring conversations about racism and police use of force.
17 As emergency physicians often continue the work of the police and paramedics in managing agitation, this national reflection must extend into the realm of emergency medicine. Although there are important differences in the roles inhabited by police and physicians in managing agitation, many similar challenges exist as well. For example, deaths have been reported during restraint use in the medical field.
15,18 To provide the best care for the agitated patient, considerations must be given to the ethical and legal aspects of restraint, the biases which influence these decisions, and the important next steps in mitigating these biases and minimizing harm.
Overview of the Ethical and Legal Frameworks Around Restraining an Agitated Patient
The decision to restrain an agitated patient has ethical, legal, and practical dimensions. There are multiple manners of restraint—often categorized as either chemical and physical restraints.
12,13 Chemical restraints involve the use of medications to calm a patient by decreasing their level of consciousness or awareness.
13 Physical restraints act to manually restrict movement, primarily by limiting repositioning of their limbs.
15 For both chemical and physical restraints, the aim is ostensibly for temporary deescalation of agitation until previously ingested drugs are metabolized, moods are stabilized, or other management is initiated.
12 The practical manner of restraint use must fit within the overarching goal of protection for staff and patients, while limiting its harm. In this balance between the need for restraint and its potential harms lays potential ethical and legal complexities.
Ethics of Agitation Management
The American Medical Association (AMA) Code of Ethics notes that “when a patient poses a significant danger to self or others, it may be appropriate to restrain the patient involuntarily. In such situations, the least restrictive restraint reasonable should be implemented and the restraint should be removed promptly when no longer needed.”
19 These guidelines underscore the deeper ethical tensions between the need for acute medical care and patient autonomy. The core ethical framework of medicine may be generally stated as to value and protect human life and dignity. This manifests in medicine as an obligation to improve individual health and well-being, while limiting harm (nonmaleficence) and respecting autonomy.
20 In the setting of the acutely agitated patient, the dual goals of helping the patient and adhering to their wishes can be in direct conflict.
20 Patient autonomy, in this situation, may lead to self-harm or the harm of others, violating the founding principle of “first, do no harm.” Depending on the specific scenario, the balance can tip in favor of nonmaleficence versus respecting patient autonomy, leading to the decision to restrain. These ethical tensions are complicated and often without simple answers, yet must be processed rapidly and under pressure.
Legal Framework of Restraint Use
In those strained few minutes of assessing an agitated patient, physicians must also be aware of the legal dimensions to the management of acute agitation. They must judge the patient's capacity to consent, defined as the patient's ability to make a decision on their own behalf.
21 Capacity involves the ability to understand information presented, to appreciate the consequences of action, and to make and communicate a decision.
21 The question of capacity is central to the process of restraint. If a patient is deemed by the clinician to have capacity to consent, they may choose to refuse evaluation and treatment. In patients without capacity, as most likely determined by clinicians when deciding to use restraint, clinicians must turn to surrogate channels to identify the desires, needs, and best care for the patients.
22 These channels include family, the medical chart, and cultural guidance. More often than not, in these acute settings of agitation, the medical decisions are left in the hands of the clinician with very limited information.
At the core of these ethical and legal considerations, the decision to restrain often comes down to the individual clinician's personal experience and judgment. While patient autonomy and nonmaleficence are considerations, the well- being of the individual and the health care worker are paramount in the decision-making process. When clinical decisions may be based primarily on personal judgment, physician variability and personal bias are inevitably introduced into the decision making. Grounded in these ethical, legal, and practical understandings of restraint use, we aim to understand how providers’ implicit biases may impact the management of the agitated patient in the ED. By exposing and understanding the anatomy of our own biases, we have the ability to improve care of our patients.
Implicit Bias
Implicit bias is a normal behavioral phenomenon, influencing many social interactions.
23 Human beings use implicit bias to navigate the world and understand complex cognitive inputs. These biases are often beyond the individual and result from a lifetime of experiences, shaped by one's larger cultural context and social institutions.
24 Although the term, “bias,” carries a negative connotation in daily discussion, they are common and inherent to many social encounters, including encounters within health care.
23,25 It may be difficult, even impossible, to be free of all implicit biases; however, medical professionals can work to improve awareness of both implicit and explicit prejudices and potentially mitigate their deleterious effects.
The roots of health disparities are often multifactorial, but provider bias can be a profound contributor.
26 The attitudes of health care professionals, and their resulting behaviors, have a significant impact on all aspects of a patient's care including patient–provider communications, diagnosis, treatment decisions, and adherence.
27 When compared to interactions with White patients, physicians have been found to be more verbally dominant and less engaged in patient-centered communications with Black patients.
28 Physicians have been found to recommend thrombolysis less often to Black patients compared to White patients in the treatment of acute coronary syndrome.
29 Black patients, when treated by providers with pro-White bias, were less likely to fill prescriptions.
30 These cumulative and oftentimes subtle biases contribute measurably to patient outcomes.
Much like in other areas of medicine, implicit biases result in patient outcome differences in emergency medicine. In a review of 5 years of CDC surveys involving over 6,000 ED visits, White patients were found to receive pain medications more frequently than non-White patients for abdominal pain.
31 When evaluating chest pain, Black patients, particularly Black female patients, had significantly fewer diagnostic tests ordered.
32 When compared to White patients, non-White patients were also found to have longer ED wait times and decreased admission rates for similar clinical presentations.
31 Implicit bias, which plays a tangible role in many other aspects of ED provider–patient interactions, also likely influences how agitation is managed in the ED.
Although there is no definitive national data for racial or gender differences in ED restraint practice, some preliminary evidence has emerged. A study from Massachusetts General Hospital in 2020 found that Black patients were more likely to be restrained when compared to White and Asian patients.
6 Similar findings were reported in a cross- sectional study at Yale New Haven Health System of nearly 7,100 physician restraint orders in the ED from 2014 to 2018.
7 Male gender and insurance status were also found to impact the odds of restraint use. These studies suggest the need for future research to identify the magnitude of the issue at stake.
In the ED setting of increased stress and time pressure, one can hypothesize how bias may configure into the decision for restraint. Reliance on implicit bias has been found to increase with increased cognitive load,
33 such as when health workers are busy or managing complicated conditions.
11 The complexity of these situations is often further exacerbated by increased rates of violent acts in overcrowded EDs,
34 potentially resulting in increased need for restraint use. The compounding effects of both provider and patient factors in these high-stress settings can create a health care ecosystem ripe for inequities in health delivery and outcomes.
Recommendations
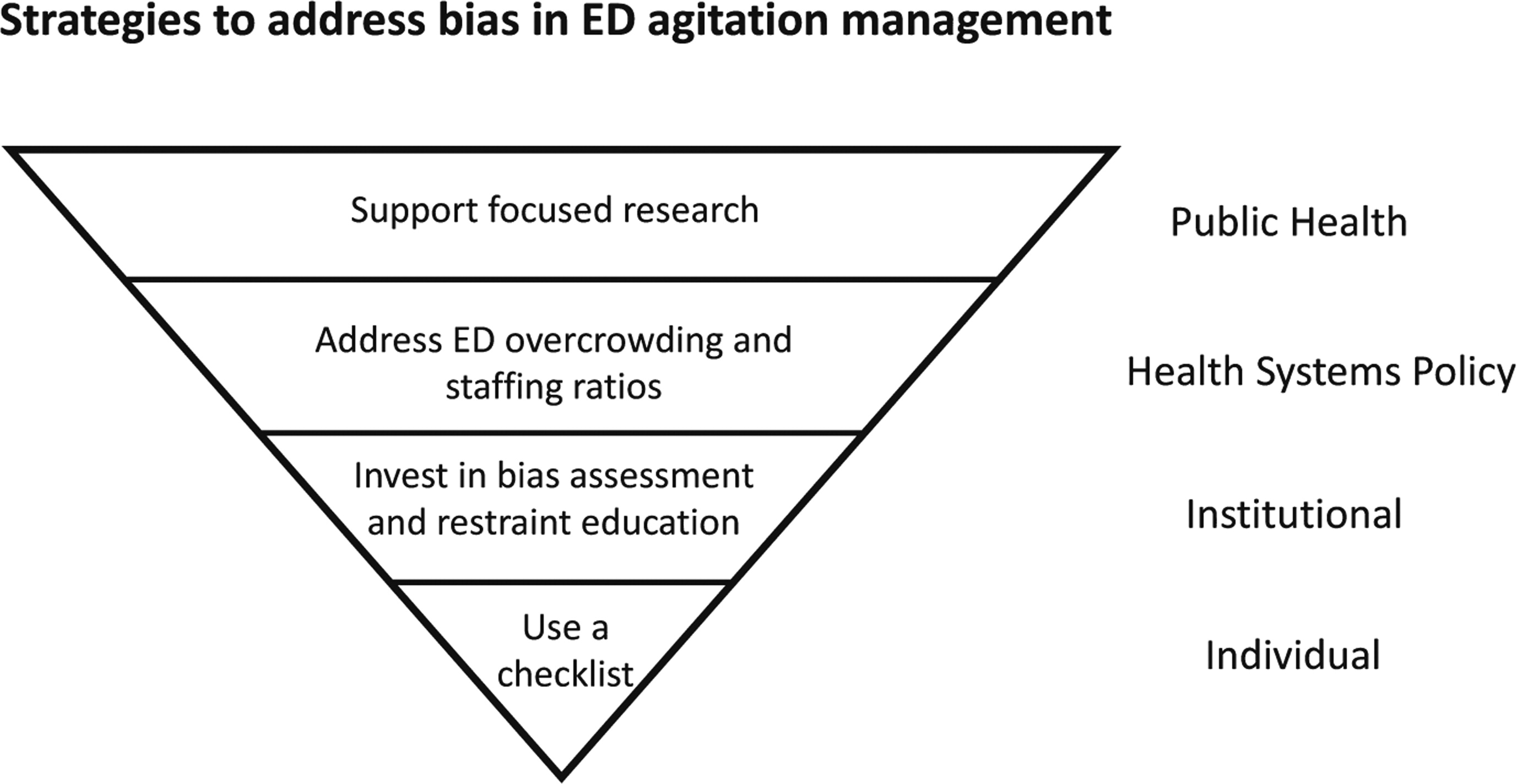
To provide constructive guidance for medical professionals caring for agitated patients in the ED, the authors developed the four strategies as noted below. These recommendations are based on a synthesis of an extensive literature review on applied health equity, clinical experiences with agitation care, expertise in human rights and bioethics, and personal experiences with racism.
A first pass of recommendations was generated by one author (TCA) after review of existing best practices in agitation management, implicit bias mitigation, and general behavior change strategies in psychology and medicine.
25,35–37 All three authors conferenced on multiple occasions and reviewed the recommendations until the group reached consensus on the top evidence guided, practical strategies on mitigating bias in ED agitation care. The authors applied a health systems approach to their recommendations to identify potential redress at the broader systemic, institutional, and individual levels (
Figure 1).
At the Public Health Systems Level: Support Focused Research
The prevalence of agitation among ED patients is increasing and characterization of medical professional restraint use in the ED setting has been limited.
6,38 To our best knowledge, there are only a few studies that look for meaningful demographic group differences in restraint use in the ED.
5–7 To better understand and improve care of agitated patients, more collective data are needed about patient, provider, and situational variabilities which may influence care. An example of this include the National Database of Nursing Quality Indicators (NDNQI), the largest database of unit-level, nurse-sensitive performance data in the United States, collecting data on nursing ratio and restraint use from 869 U.S. hospitals on the care of more than 923,000 patients from 2006 to 2010.
33 We can expand on large-scale databases, such as the NDNQI, to include physician behaviors and collect information about how we are restraining and who we are restraining.
36 This would allow for identification of any large-scale differences in practice pattern, potentially identifying racial and other differences in overall restraint use and types of restraint used. Certain factors, such as provider-to-patient ratios, may appear as potential targets for decreasing disparities in care.
At the Health System Policy Level: Address ED Overcrowding and Staffing Ratios
Overcrowded conditions and understaffed EDs—particularly with poor nurse–patient ratios—can exacerbate cognitive stress and amplify implicit bias.
11,36 The NDNQI found that the higher the average percentage of nurses on shift, the less likely restraints would be used.
36 Furthermore, when assessing implicit bias in resident physicians, Johnson et al.
11 found increased bias in those working in higher stress environments, such as when the ED was overcrowded. Stress can lessen providers’ ability to self- regulate, confront, and override their implicit bias.
11,35 In a less crowded, better staffed ED, there may be more opportunity to identify and pay closer attention to an agitated patient, optimize patient privacy, and employ strategies such as verbal deescalation.
36 Interventions focused on creating better spaces for patients and ED providers can improve patient throughput and decrease clinician cognitive load, which may be useful in promoting unbiased agitation management.
11At the Institutional Level: Invest in Bias Assessment and Restraint Education
Institution-based efforts on individual bias can provide space for nonjudgmental dialogue and concrete systemic improvements.
39,40 An introductory assessment of bias can start the conversation on implicit bias. One of the most studied tools in measuring unconscious bias, the Implicit Association Test (IAT), was developed in 1998 to measure how quickly people associate different terms with one another as a measurement of individual biases.
41 The IAT is effective in increasing self-awareness and generating small-group discussion about bias.
39,40 However, changes in the score may not necessarily translate to actual behavioral and clinical change.
35,37 Implicit bias training focused solely on recognizing bias may fall short by not providing its participants with the necessary tools to interrupt and remodel their habitual responses.
35 Moving beyond increasing awareness, programs can assist participants in developing practical strategies, such as using checklists during agitation management, to respond to their recognitions of bias and modify their verbal and nonverbal communications.
35To provide equitable and improved care to patients, institutions must identify eliminating disparity in restraint use as a priority. An initial step can include collection of individualized and departmental restraint data, similar to other prioritized quality and productivity metrics, such as left without being seen rates, median length of stay, and specifics of sepsis care.
42 This targeted feedback on restraint use can be used to identify opportunities for improvement.
43 If carefully aligned with structured metrics, incentives can be employed to encourage meaningful change.
44 Individualized data should be coupled with reporting on institutional factors that may contribute to the variabilities in restraint use, such as availability of security, fluctuations in patient volume, specific shift times, and incidence of violence.
34 This will allow for more holistic assessment of the clinical environments contributing to employment of restraints.
At the Individual Level: Employ a “Restraint Checklist”
Checklists are used commonly in medicine and are arguably one of the most effective methods for improving performance under pressure and reducing medical error.
45,46 Through deliberative reflection and motivated self-regulation, a checklist is a potential tool for remodeling of habitual responses, as noted in the previous recommendation.
45 They provide an opportunity to slow down and review an approach to care, especially in settings of heightened emotions. Restraints are sometimes necessary in the management of agitation, for the safety of patients and those around them. To assure that restraints are reserved primarily for these purposes, each provider or institution can create their own short mental checklist to stop, recognize, and potentially circumvent bias in these stressful encounters.
The following restraint checklist was developed by the authors, after a review of the literature yielded no other checklists that addressed bias in agitation care. The preliminary checklist questions were developed by one author (TCA) after a literature review on checklists in medicine and lessons from deescalation strategies used in personal patient care experiences.
45–49 The initial list was reviewed and further refined by all coauthors. Each iteration of the list was based on author consensus about structure, order, content, and number of checklists questions that could prove practical in a real-world clinical scenario.
Five restraint checklist questions:
1.
Have I tried to listen to the patient's desires, employ verbal deescalation, and other alternatives to chemical/physical restraints (such as offering food/drink)?
2.
Is a different staff member, outside of myself or the patient's primary care team, better at deescalating this patient based on demographic similarities (or differences, such as agitated male patient who responds better to female staff
50)?
3.
Is my fear of this patient exaggerated by their appearance?
4.
Are there cultural differences in the patient's expression of frustration and control?
5.
Am I using racial, gender, socioeconomic, or other potentially harmful bias in determining my agitation care plan for this patient?
These, or an abbreviated version of these questions, may be helpful in creating new cognitive habits by allowing for a group or individual internal “timeout”—allowing for an intentional pause in patient treatment and bringing awareness to potential bias.
Conclusion
Emergency medical professionals are frontline workers who are responsible for caring for all patients, regardless of presenting complaint and irrespective of descriptors such as socioeconomic and insurance status, gender preference, primary language, and race.
51,52 This unselective care is a common draw for health professionals to emergency medicine, which may make it difficult for providers to recognize that implicit bias can play a role in their care. We should acknowledge that bias may not always be harmful in the ED, as career survival often depends on taking mental shortcuts and making quick decisions for patients in the absence of complete information and without previous doctor–patient relationships.
53 By accepting and recognizing the ubiquitous nature of implicit bias, we can actively make
explicit these
implicit biases and intervene in some of their detrimental effects on the care of our patients.
Bias in health care does not exist in a vacuum; it results from and perpetuates larger systemic biases. Similar to interactions with law enforcement, encounters with the medical system are often more impactful than any routine interaction—they can be moments of transformation for an individual. The use of physical and chemical restraint, though sometimes necessary to promote safety, is not without potential physical and psychological harm.
4,14,16 For some people, such as George Floyd and Elijah McClain (Elijah McClain is a 23-year-old in Aurora, Colorado, who died in 2019 after being physically restrained and injected with ketamine by law enforcement and paramedics), bias and restraint misuse can result in death. As physicians, it is our duty to understand and address our implicit biases, as well as the systems that amplify them, to provide equitable care for the agitated patient. As the nation reckons with its history and current state of racism, we as medical professionals must be at the forefront in acknowledging our own biases and improving our care.