Even though schizophrenia affects only 1% of the total population, the economic burden of schizophrenia in the United States was estimated at $155.7 billion in 2013, with $9.2 billion of the total costs attributed to medications (
1). Although most individuals with a diagnosis of schizophrenia qualify for government-provided health insurance (Medicaid and Medicare), studies conducted before passage of the Affordable Care Act (ACA) estimated that 7%–20% of affected individuals lacked any form of health insurance (
2,
3). Implementation of the ACA improved insurance coverage for individuals with mental health conditions in general; however, data specific to patients with schizophrenia are not yet available (
4).
A recent study found that after implementation of ACA coverage of dependents under age 26 on their parents’ insurance plans, hospitalizations of individuals in this age group who were experiencing early psychosis were more likely to be paid for by private insurance and less likely to be paid for by public insurance, with no difference in overall insurance coverage, compared with the pre-ACA period (
5). This shift from public to private insurance may be costly because individuals covered by private insurance continue to face costs from increasing insurance deductibles (
6). Access to antipsychotic medications is imperative in preventing disease relapse and the emergence of psychotic symptoms. Consistent and transparent pricing of medications is essential to accessing critical medication in this population.
Patent expiration for newly developed (brand) medications allows additional manufacturers to develop generic equivalents of those medications. As the number of manufacturers of a generic medication increases, the cost of the medication decreases (
7). A Department of Health and Human Services report in 2016 confirmed that competition in the generic medication market continued to reduce costs overall despite notable increases in costs of certain generic medications (
8). Despite these findings, portions of the generic medication market show increasing prices for some generic medications (
9).
There is significant variability in the retail cash pricing of generic medications (
10,
11), and prices may differ by pharmacy type (
12,
13). Studies of medications used to treat heart failure, oral antibiotics, commonly prescribed eardrops, and medications for chronic conditions found significant variability in cost by pharmacy type (chain, grocery, or independent pharmacy) (
10–
13). Of note, the results of these studies were conflicting regarding price variability across pharmacy types, with some results supporting claims that chain pharmacies had the lowest retail cash prices (
13) and others supporting claims that these pharmacies had the highest retail cash prices (
12).
Current schizophrenia treatment guidelines support the use of second-generation antipsychotics, with the exception of clozapine, as first-line therapy (
14). Five second-generation antipsychotics recommended for first-line treatment were available in a generic formulation in 2017: risperidone, olanzapine, quetiapine, ziprasidone, and aripiprazole. No studies have examined price variability in generic antipsychotic medications. Therefore, the objectives of this research were to examine the variability in pricing of generic antipsychotic medications used in the treatment of schizophrenia in the Kansas City metropolitan area and to determine whether prices varied by pharmacy type (independent, grocery store, or chain).
Methods
Pharmacies
The Missouri Division of Professional Registry and Kansas Board of Pharmacy provided information for retail pharmacies in Jackson, Clay, and Platte Counties in Missouri and Johnson and Wyandotte Counties in Kansas. The five counties selected encompass the majority of the Kansas City metropolitan region and a population of 1.7 million people. At the time of data collection, 281 pharmacies operated in the selected counties. Pharmacies excluded from data collection included nine specialty and three nonoperational pharmacies. Other exclusions included two duplicate listings, one pharmacy located outside the selected counties, and one pharmacy call service.
Medications of Interest
All the antipsychotic medications studied were listed among the top 300 prescribed medications in the United States for 2018 (
15). The recommended therapeutic dose for schizophrenia identified in product labeling determined the doses queried for each medication. Medication doses studied included: risperidone 4 mg per day, olanzapine 20 mg per day, quetiapine 600 mg per day (300 mg two times per day), ziprasidone 160 mg per day (80 mg two times per day), aripiprazole 20 mg per day, and haloperidol 10 mg per day. Haloperidol, an older but commonly used first-generation antipsychotic, served as a price comparison with the second-generation antipsychotics.
Study Design
Over 30 days (April 25–May 25, 2017), each pharmacy responded to phone queries requesting the cash price of a 30-day supply of two of the six antipsychotic medications. Pharmacy students assisted with phone queries. To mimic a patient’s interaction and limit questions from the pharmacy, each call included requests for the cash price of two medications at the specific strength and number of doses. Students called each pharmacy three separate times to obtain prices for all six medications. The requested price was for 30 doses or a 30-day supply of risperidone, haloperidol, olanzapine, and aripiprazole at the selected strength, because these medications are dosed once daily. Quetiapine and ziprasidone are dosed twice daily, and prices requested were for 60 doses of quetiapine 300 mg and ziprasidone 80 mg. If the requested strength was not available, the response was not included in the analysis. Discounted prices offered with the use of a membership card or coupon were not recorded.
Pricing data collection was managed with the REDCap electronic data capture tool hosted at the Center for Health Insights of the University of Missouri–Kansas City (UMKC) (
16). The UMKC Adult Health Sciences Institutional Review Board designated this study as not human subjects research.
Statistical Analysis
Statistical analyses were completed with IBM SPSS Statistics, version 24, and SAS, version 9.4. Descriptive statistics were used to generate median medication prices, both overall and for each medication by pharmacy type. Absolute cost variability for each medication was calculated as absolute cost variability=(maximum–minimum price). A max-min price ratio (maximum price/minimum price) was also calculated for each medication.
The Kruskal-Wallis H test for nonnormally distributed data was used to test the statistical significance of differences in median pricing for each of the six antipsychotic medications across the three pharmacy types. After a significant Kruskal-Wallis H test, pairwise comparisons between pharmacy types on median pricing of the six antipsychotic medications were assessed by using Dunn’s post hoc test. Levene’s test was used to assess variability in price across medications. Generalized linear models (PROC GLM in SAS) estimated the association of price with pharmacy type and interaction with medication type. Overall statistical significance was assessed with the alpha level set to 0.05. Alpha levels were adjusted with a Bonferroni correction to address the issue of multiple comparisons.
Results
Of the 265 pharmacies included in data collection, 147 were in Missouri and 118 in Kansas (a map of the pharmacy locations is included in an online supplement to this article). Each pharmacy was categorized as either a nationwide chain pharmacy (N=182), a grocery store pharmacy (N=53), or an independent pharmacy (N=30). Chain pharmacies included stores that also sell groceries, such as Walmart and Costco, because they have locations across the nation and purchasing power comparable to that of other chain pharmacies. Two nationwide chains accounted for over 50% of the included pharmacies (N=139).
Overall Pricing by Medication
Of the 265 pharmacies, 238 (90%) had all six medications in stock at the specified strengths. The median price of the six medications varied greatly (
Table 1). Medication prices did not follow a normal distribution. Examination of pricing across medications revealed that aripiprazole had the most absolute cost variability ($1,315.01) and haloperidol had the least ($82.99). Levene’s test confirmed statistically significant differences in price variability across medications (p<0.01).
Pricing by Pharmacy Type
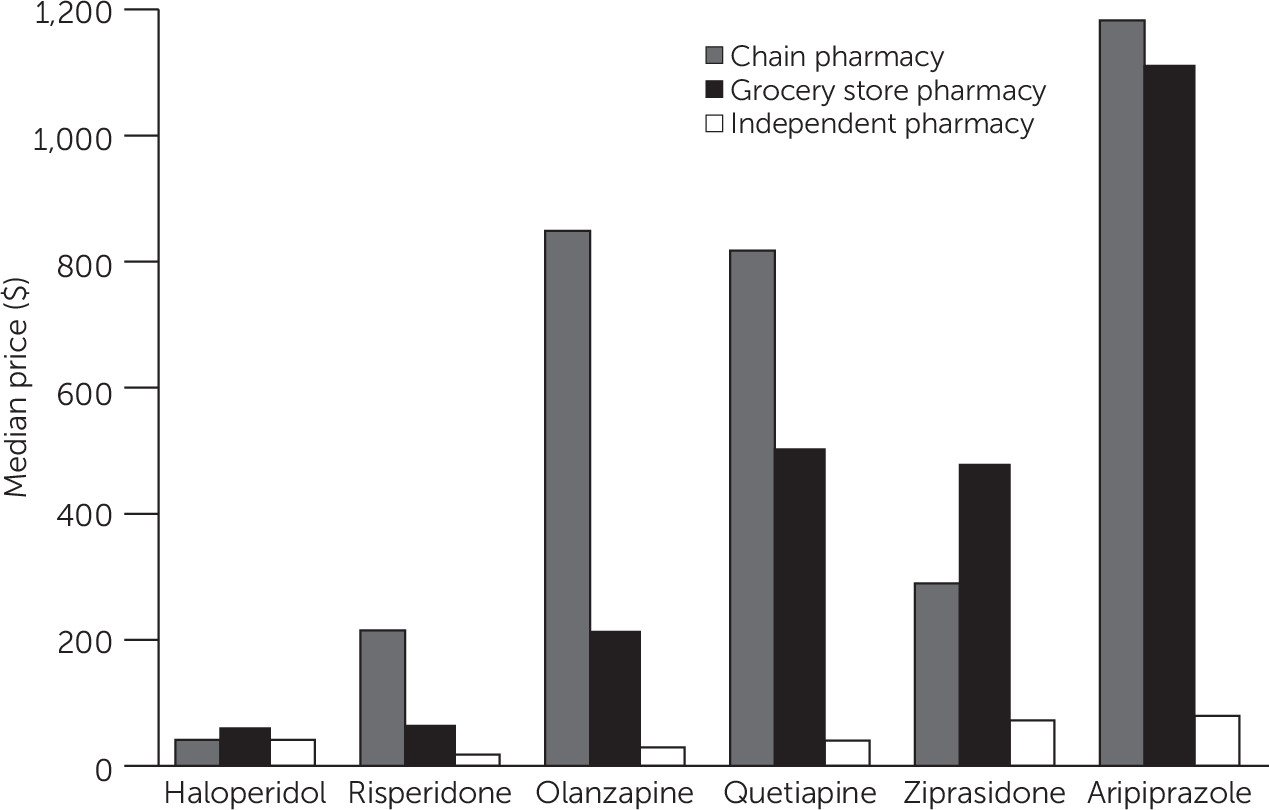
Pricing for all six antipsychotic medications varied significantly by pharmacy type (p<0.001 for all) (
Table 2). Pairwise comparisons showed a significant difference in pricing between all pharmacy types for four of the medications: olanzapine, ziprasidone, quetiapine, and aripiprazole. Prices for risperidone showed a significant difference for two of three pharmacy type comparisons. Prices for haloperidol significantly differed only between chain and grocery store pharmacies. Median prices were highest at grocery store pharmacies for ziprasidone and haloperidol (
Table 2). For all second-generation antipsychotics, the median price was significantly lower at independent pharmacies, compared with chain pharmacies (p<0.001), with the median price for these medications ranging from $196 to $1,100 higher at chain pharmacies.
Altogether, prices varied significantly by pharmacy type, with the prices generally highest at chain pharmacies, followed by grocery store pharmacies, and lowest at independent pharmacies. The interaction between medication price and pharmacy type was significant, confirming that the difference in pricing between medications varied by pharmacy type (
Table 3 and
Figure 1).
Discussion
In our study sample of pharmacies in the greater Kansas City area, retail cash prices for a 30-day supply of generic antipsychotics differed by more than $1,000 between pharmacies for half of the medications studied. Despite this wide price range, 30-day supplies of each medication could be obtained at one or more pharmacies for less than $40. Haloperidol, a first-generation antipsychotic that has been generically available since 1986, had the smallest variability in pricing, but it did not have the lowest quoted price. Individuals without insurance may be able to access a second-generation antipsychotic at the same or a lower price than a first-generation antipsychotic, because lower minimum prices were quoted for both risperidone and olanzapine, and the lowest quoted price for quetiapine was same ($20). At independent pharmacies, risperidone, olanzapine, and quetiapine had lower median prices, compared with haloperidol. The availability of three newer second-generation medications at a price lower than or the same as haloperidol may benefit patients with schizophrenia, considering the reduced risk of movement disorders associated with second-generation antipsychotics.
All six medications had significant differences in pricing between at least two pharmacy types. Overall, chain pharmacies had the highest prices, followed by grocery stores, and independent pharmacies. Within each nationwide pharmacy chain, multiple locations often had the same prices for each medication; however, prices varied across the metropolitan area in general. Prices were less consistent across grocery store chains, and only the largest regional chain (eight states) had consistent prices across multiple locations. This variability suggests that having access to a variety of pharmacy types and comparing prices across different locations of the same pharmacy may benefit patients.
In an effort to assist patients to pay the lowest price for their medications, some states have established website databases of publicly reported medication prices at pharmacies. The reliability of these databases, including a database for Missouri that is no longer operational, in terms of their having information for all pharmacies has not been demonstrated (
17). Given promising findings for differences in price by pharmacy type and the potential benefit of identifying the lowest cost for medication, such state websites may provide benefit to both providers and patients if the sites are well managed (
12).
Individuals with schizophrenia often have co-occurring cognitive deficits, and thus the utility of websites for price comparisons by these individuals remains questionable. A recent study of patients with severe mental illness in the Department of Veterans Affairs health system found that these patients were less likely to use the Internet, compared with patients without severe mental illness (51% versus 71%) (
18). Without access to the Internet, uninsured individuals may not benefit from prescription coupon websites, such as GoodRx or Blink Health. These individuals may also struggle to identify and contact multiple pharmacies by phone to find a lower price. Therefore, the best outcome for patients may be a combination of counseling patients on how to obtain low-priced medications and provision by health care providers of medication coupons to patients.
Strengths and Limitations
Although previous studies collected data from a random sample of pharmacies or pharmacies in a single county, this study included data for every retail pharmacy in a five-county metropolitan region. However, the study data were limited to one midwestern metropolitan area and may not be reflective of other areas. The selection of antipsychotics for evaluation was based on treatment guidelines for schizophrenia, with the addition of haloperidol as a comparator, because the selected medications reflected current antipsychotic prescribing patterns. Antipsychotic medications are used in the treatment of other psychiatric disorders, such as bipolar disorder and depression, and the results of this study may not reflect the costs associated with treating these disorders, because antipsychotic dosing recommendations are different.
Data on insurance coverage specific to patients with schizophrenia following implementation of the ACA are not yet available. At the time of data collection, Kansas and Missouri elected not to expand Medicaid coverage under the ACA. Patients with schizophrenia who are deemed disabled qualify for Medicaid coverage of their antipsychotic medications in both states. However, all nondisabled adults without dependent children remain ineligible for Medicaid coverage. As a result, gaps in coverage for patients with schizophrenia are likely, but the percentage of patients paying out-of-pocket costs for antipsychotic medications is unknown. Patients without insurance coverage may also benefit from medication assistance pharmacies and programs to help cover medication costs; however, these programs vary by facility. Prices from safety-net pharmacies were not included in this study.
Study data were collected over a short period, 1 month, to reduce any impact from market fluctuation in prices. However, cost data were not collected regarding availability of pharmacy discount plans, coupon pricing, or discount membership. On several occasions, the pharmacy employee offered suggestions on how to obtain the prescriptions at a lower price; however, data on how often this occurred were not recorded. In addition, the number of manufacturers and market demand affect generic medication prices, and generic medication prices are liable to fluctuate over time, which may limit the generalizability of study findings.
Data were collected by study staff and volunteer pharmacy students, and thus the data reflect information provided to an educated consumer. Individuals with cognitive and relational difficulties common in major mental illnesses such as schizophrenia may have greater difficulty providing the necessary information about their prescription to obtain pricing information.
Future Directions
Further analyses are necessary to determine whether socioeconomic or neighborhood characteristics contribute to price variability. A recent study in Chicago found significant differences in the pharmacy availability in segregated white and racial-ethnic minority communities (
19). The types of pharmacies available also significantly differed in segregated white and black communities. The visual representation of pharmacies by type in the map (see
online supplement) suggests that similar discrepancies may exist in the Kansas City metropolitan area.
Studies examining medication pricing and neighborhood characteristics using zip code–level information have revealed price discrepancies corresponding to race and income. A study in Wayne County, Michigan, found prices of generic levothyroxine to be higher in zip codes with lower income (
20). A study of publicly reported prices from a Florida prescription database discovered mean prices were 9% higher in poorer areas (
13); however, not all studies have replicated these findings (
12). Next steps for this study will be an examination of antipsychotic pricing and area-level characteristics, as well as access to pharmacy types. As prescription discount websites become increasingly popular, future studies should examine the variability in retail cash pricing in the context of these discount programs as well.
Study findings suggest that variability in the antipsychotic price range trended with the length of time the medication was available generically, with haloperidol having the lowest variability in price and aripiprazole the highest. Recent studies have found that prices are reduced as the number of generic manufacturers increases (
7). Additional analyses may examine the relationship between length of time a medication is available generically, number of manufacturers, and price in order to determine whether this trend exists for antipsychotic medications.
Conclusions
As has been found for medications with other indications, this study found that prices for antipsychotic medications varied greatly. Prices also varied significantly by pharmacy type. Overall, chain pharmacies had the highest pricing and independent pharmacies the lowest. Differences in prices by pharmacy type also varied for each medication. This information is potentially useful to health care professionals and other stakeholders engaged in the delivery of care to patients with prescribed antipsychotic medications. By understanding where and how patients can access low-cost antipsychotic medications, providers may be able to provide patients with the best possible treatment option at the lowest cost.