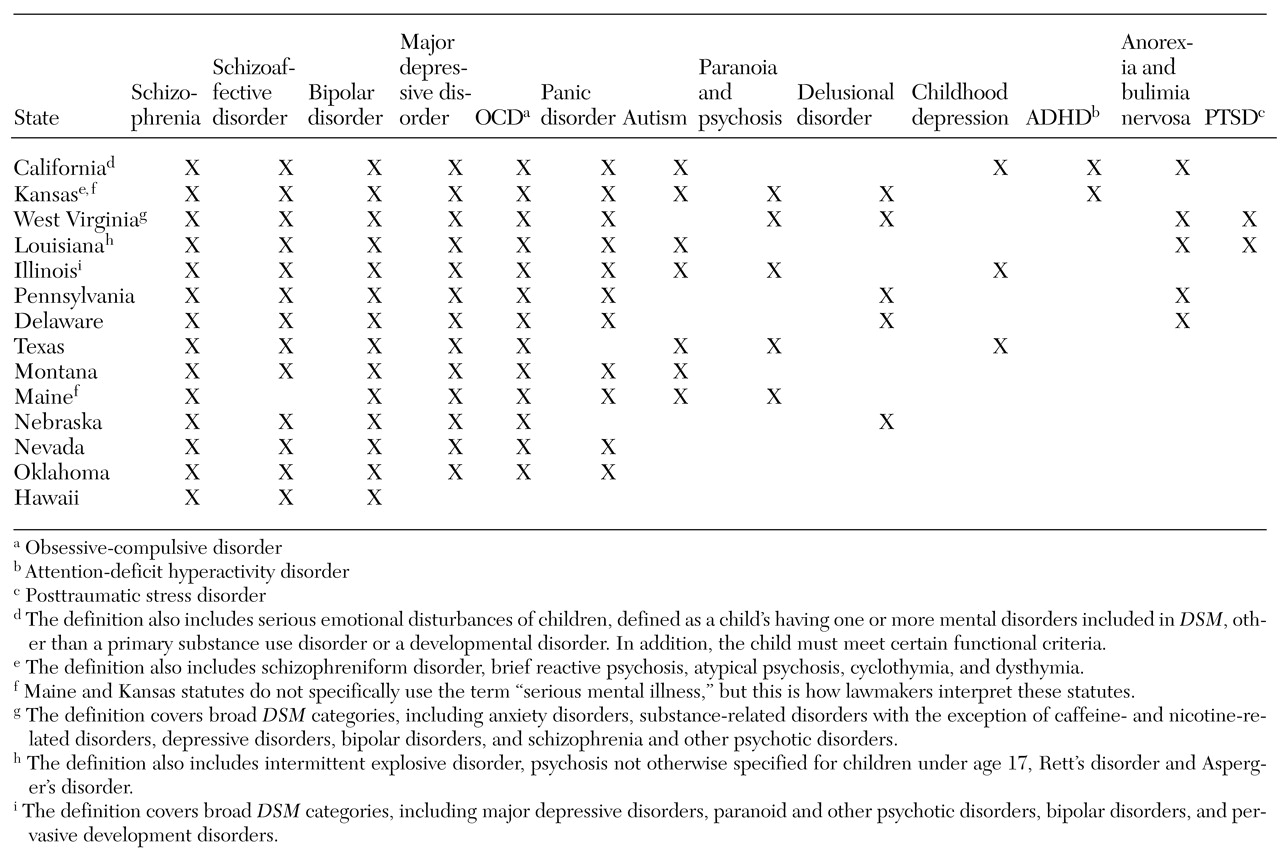
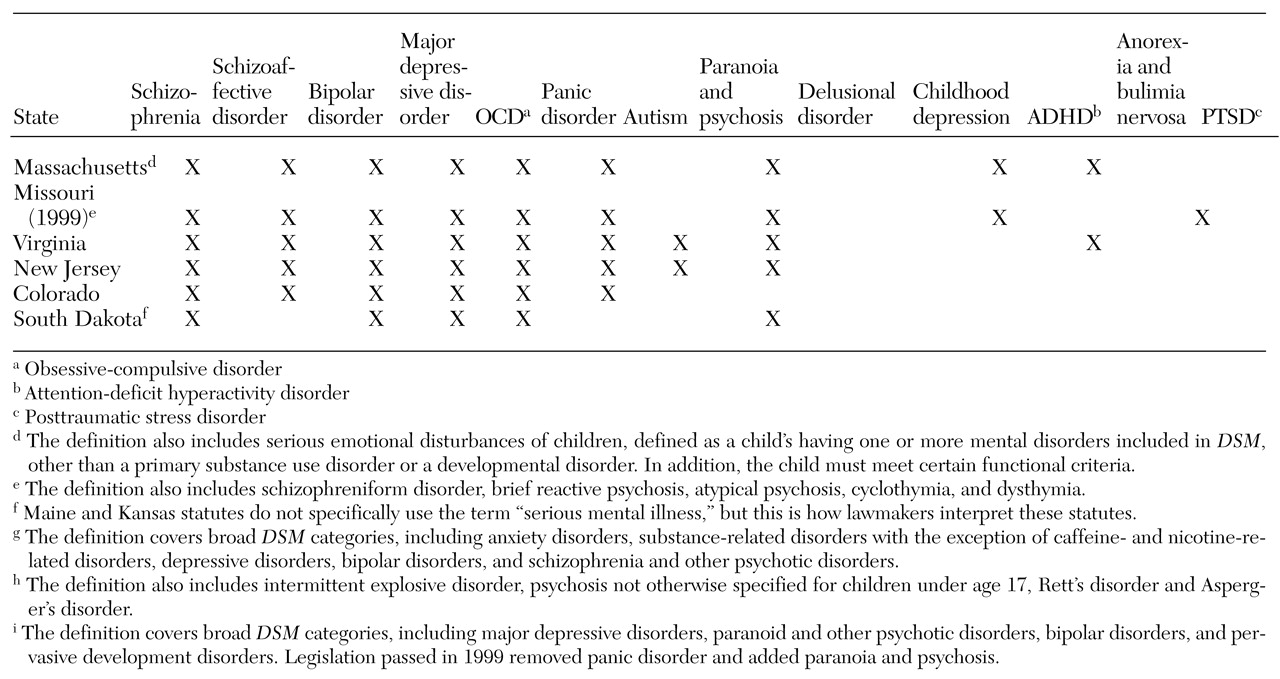
The tables highlight the wide variation found in the definitions of mental illness used in parity laws. This variation leads to the question of where states are getting their definitions of mental illness. Traditionally, states have relied on federal policy or clinical experience as guidelines when enacting mental health policy. However, when we compared the definitions of mental illness used in the clinical literature and in federal policy with those used in state parity laws, the only agreement we found was with the seven states that include all disorders in DSM. States that use "serious mental illness" as the definition are not using the accepted combination of criteria addressing diagnosis, duration, and disability. Instead, lawmakers include only diagnosis. Finally, states that use "biologically based mental illness" as the definition are charting new territory because the term has never been used in federal legislation and has no accepted clinical definition.
Factors influencing state definitions
How are states choosing which disorders to cover at parity? From our interviews and literature review, we determined that several factors are influential, including the ideologies of advocacy groups and parity opponents, cost, and political necessity. States rarely, if ever, considered disease prevalence, needs-based studies, and clinical judgment. In our opinion the definitions that states use result from a political and economic process involving mental health advocates and providers, pro- and antiparity legislators, insurers, and employers.
More than 90 percent of the people we interviewed agreed that mental health advocacy and the interests of providers most strongly influenced how mental illness is defined in a parity bill. There are two primary mental health advocacy groups: the National Alliance for the Mentally Ill (NAMI) and the National Mental Health Association (NMHA). In most states, either NAMI or NMHA have led the parity coalition. Advocates often drafted the bill, worked closely with the legislative sponsor, wrote critical testimony, and organized grassroots support.
NAMI and NMHA each conceptualize mental illness differently. NAMI emphasizes the importance of biological factors in the etiology of serious mental disorders and advocates for "equitable services for people with severe mental illnesses, which are known to be physical brain disorders" (
11). NAMI promotes ending discrimination and demanding fair legislative policies for "priority populations with serious mental illness." Priority populations include those with schizophrenia, schizoaffective disorder, major depressive disorder, obsessive-compulsive disorder, panic disorder and other severe anxiety disorders, and attention-deficit hyperactivity disorder.
In contrast, NMHA defines mental illness broadly, addressing a person's ability to function rather than his or her diagnosis. NMHA has historically focused on the prevention of mental and emotional disabilities and has developed an extensive Community Prevention Services Program (
12). In our analysis, we found that more than 85 percent of NAMI-drafted bills used the "biologically based" or "serious mental illness" definitions of mental illness, whereas 100 percent of NMHA-drafted bills used the "broad-based" definition.
The two main provider organizations involved with parity are the American Psychological Association and the American Psychiatric Association. The former works with NMHA to advocate for broad-based parity. District branches of the American Psychiatric Association in each state work with both NMHA and NAMI, writing testimony and educating providers. At the national level, the American Psychiatric Association's Institute for Research and Education is conducting a study examining the effects of parity on the federal employee health benefits program (
13).
State mental health advocacy and provider groups participate in social learning in the sense that they copy definitions of mental illness from existing state parity laws. Advocates report that using a definition of mental illness that is already being implemented is an important factor in convincing lawmakers that the definition is both practical and cost-effective. For example, the Montana chapter of NAMI drafted parity legislation based on language developed by the New Hampshire chapter of NAMI for the bill that was successful in becoming New Hampshire's parity law. Similarly, the legislation drafted by Connecticut and New Jersey legislators in cooperation with local NAMI chapters used language developed by Ken Lieber-toff, director of the Vermont Mental Health Association and author of Vermont's successful bill.
Cost was the second most influential factor cited by interviewees as shaping the definition of mental illness. Two major organizations, the Chamber of Commerce and the National Federation of Independent Business, strongly argued that mandates requiring coverage for all
DSM disorders would lead to uncontrolled demand for mental health services and would cause businesses to drop health insurance altogether, increasing the number of uninsured people by almost 6 percent (
14). In Hawaii, the only state requiring employers to provide health insurance, lawmakers narrowed the definition of mental illness in the mental health parity bill to three specific illnesses chosen by local insurers—schizophrenia, schizoaffective disorder, and bipolar disorder.
Third, the political strategy that has been used to "sell" parity has influenced the definition of mental illness. A biologically based definition of mental illness allows advocates to frame parity legislation as antidiscrimination legislation. Using positron emission tomography (PET) scans or magnetic resonance imaging (MRI) that shows obvious lesions, researchers have testified before Congress and state legislatures that mental illness is directly linked to brain dysfunction. Faced with such testimony, policy makers can hardly argue that mental illness is not a brain disorder and that it should not be treated like diseases of the heart or lungs.
Finally, political necessity has shaped the definition of mental illness. Many of the people we interviewed faced a "take it or leave it" scenario, in which definitions of mental illness were narrowed to increase the probability of a bill's passage. For example, risk-averse politicians in antiregulation states such as Delaware and South Dakota preferred an incremental approach, which made narrow bills more attractive. New Jersey, having failed to pass three successive parity bills that used a broad-based definition of mental illness and facing a fourth defeat, pared the definition of mental illness down to eight diagnoses. In such cases, advocates strategize that establishing limited parity is critical to paving the way for broader bills. For example, Connecticut passed a bill in 1997 that used the biologically based definition, and in 1999 the bill was amended to cover broad-based mental illness.
Implications of variation
Why should clinicians and policy makers be concerned about the definitions of mental illness used in parity laws? We could simply agree that a state's passage of parity legislation will increase access to mental health care for the privately insured population, regardless of the specific illnesses covered in the bill. However, this is not necessarily true—definitions matter, and research supports the fact that definitions matter. Narrow and colleagues (
15) applied three different clinical definitions of serious mental illness to the same population and found that the prevalence rates ranged from 3 percent to 23 percent.
Definitions used in parity laws have important access and cost implications, which are discussed below.
Access implications. Access to mental health services refers to the ability to obtain treatment for mental health disorders with appropriate professionals. An important determinant of access is the level of copayments, deductibles, and limits, which are all affected by parity laws (
5). Under all federal and state parity laws, insurers pay for care after a mental disorder is diagnosed. Thus the definition of mental illness used by an insurer is critical. To be considered for parity coverage, a person must qualify for a diagnosis included in the parity law in his or her state. Without such a diagnosis, it is unlikely that state laws will mandate insurers to cover any minimum level of treatment.
When states use political and economic criteria to choose reimbursable
DSM diagnoses, some populations in need of services will be missed.
DSM was not designed to prioritize the needs of mentally ill populations.
DSM outlines a clinical classification system that is based on a continuum of self-reported symptom clusters, not specific functional limitations. This makes the line between a disorder considered "serious" and one considered "not serious" arbitrary (
16).
For example, the
DSM criteria for major depression, considered a "serious mental illness" in state parity laws, can be met by having five of nine possible symptoms over a two-week period. Kendler and Gardner (
16) found that these
DSM criteria create an arbitrary cutoff on a continuum of depressive symptoms and do not accurately reflect the severity of illness. A study by Regier and colleagues (
17) found that simply changing the order of the questions used in epidemiological survey instruments can affect the prevalence rate for
DSM disorders.
Patients with subthreshold disorders—that is, those who have symptoms that do not meet
DSM criteria—may have significant disability, but they are denied access to care under limited-parity bills. For example, minor depression is defined as two or more depressive symptoms lasting at least two weeks but not meeting criteria for major depression or dysthymia (
18). A person with minor depression who lives alone in a dilapidated apartment may have more need of hospitalization than a person who has major depression and a supportive family (
19). Among persons with subthreshold depressive symptoms, the disorder progresses if it is untreated. Wells and colleagues (
20) showed that 54 percent of people with dysthymia developed major depression during a two-year follow-up period.
A second population missed by limited parity legislation is children. In 1982 Knitzer (
21) found that two-thirds of the three million American children with serious emotional disturbances were not receiving needed services. The report from the 2001 Surgeon General's Conference on Children's Mental Health (
22) highlighted this crisis and noted that most children with serious emotional disturbances who had private insurance were not receiving professional help. It is clear that children's mental health is an area in which parity laws can have an important impact.
Unfortunately, in states in which parity legislation has a limited definition of mental illness, it is almost impossible for a child to meet the criteria for a diagnosis that requires treatment under the law. Few children can verbalize the feelings that would lead to a diagnosis of more serious
DSM disorders. In addition, children's complex developmental changes pose diagnostic challenges—the expression and course of a disorder in a child and an adult are very different (
23).
Two states, California and Massachusetts, have addressed this lack of coverage by including children's parity provisions. To qualify for coverage at parity, a child must be diagnosed as having any DSM-IV disorder (excluding developmental and substance use disorders) and meet certain functional criteria, such as being at risk of removal from the home and at risk of violence. These new definitions broaden the scope of impairment and allow children to be treated earlier in the course of illness.
Cost implications. Untreated mental disorders not only incur costs to affected individuals but also have high social costs. Many factors contribute to these indirect costs, including lost work productivity, homelessness, and expenses to the criminal justice system. It has been estimated that lost productivity alone constitutes 45 percent of the total economic costs of mental disorders (
24).
In the evaluation of parity, how do definitions of mental illness affect indirect costs? Theoretically, narrower definitions lead to a higher burden of untreated illness and result in higher indirect costs. Several studies of depression indicate that subthreshold symptoms result in economic burden and that treatment can restore occupational functioning (
25,
26,
27).
Implications for behavioral health providers. The regulation of mental health treatment is not new. Previous mental health legislation excluded certain treatments or limited the number of visits. However, in past legislation eligibility for coverage was not determined by diagnosis. Linking diagnosis to reimbursement was first used in the early 1980s, when Medicare began prospective reimbursement based on diagnosis-related groups (DRGs). Under this system, Medicare pays hospitals on the basis of the "relative weight" of the DRG—that is, its overall complexity.
DRG-based reimbursement assumes that hospitals and physicians accurately code a patient's course of illness in the hospital. However, Hsia and associates (
28) found that the average hospital incorrectly codes a patient's DRG about 21 percent of the time and that these DRG changes did not occur randomly. More than 60 percent of the miscodings favored the hospital. In some cases, the codes used in reimbursement claims indicated more serious conditions or more intense treatment than was documented in the medical record—a phenomenon known as "DRG creep."
Mental health parity legislation introduces the possibility of DRG creep. The diagnosis of mental disorders is not an exact science, and minor diagnostic nuances that have little clinical importance can have major financial consequences. For physical illnesses, DRG creep is easily detected at the technical level; the results of laboratory tests, surgical procedures, and physical examinations can be used to verify coding. However, mental health records consist of self-reported data that are then translated into subjective DSM categories, which makes intentional upcoding difficult to detect.