Currently 8 percent of children receiving mental health services use residential treatment centers, and this treatment consumes almost 30 percent of national children's mental health expenditures (
1). Furthermore, inpatient hospitalization consumes about half of mental health resources for children (
1). Family participation in children's mental health services is a primary principle guiding the implementation of the Child and Adolescent Service System Program (
2,
3) and the Comprehensive Community Mental Health Services for Children and Their Families Program (
4). This principle reflects the belief that services will be more appropriate and youths will respond more positively if the family is a full partner in care (
5,
6).
Previous studies have supported the benefits of family participation in out-of-home treatment. For example, family involvement has been positively correlated with shorter stays in out-of-home care and with postplacement success (
7), and considerably reduced inpatient stays have been associated with parents' participation in interdisciplinary team meetings on a psychiatric unit (
8). However, despite these positive findings, little information is available about families' experiences with participation in residential treatment and other out-of-home treatment programs or about the factors that hinder or facilitate participation.
Baker and associates (
9) conducted one of the few studies that have described family involvement, defined as participation in social and educational activities at residential treatment facilities, telephone contact, family visits, and visits home by the child. On the basis of a sample of three treatment facilities, they found that most children with mental retardation, mental health problems, or both had a low level of involvement with their families. Surveying staff members within the three facilities about their attitudes toward various types of family involvement, Baker and associates (
10) found that staff gave less endorsement to items related to empowering families to participate in decision making in the child's program compared with their support of family involvement in parent training or family therapy. Actual rates of family participation, measured by involvement in social and educational activities at the facility, telephone contact, visits at the facility, and home visits for the child, were much lower than staff members' perceptions of the rate of family participation (
9).
Distance and limited resources appeared to constrain families' involvement, and the authors reported that opportunities for family involvement were not well developed or well articulated to parents (
9). In addition to financial and geographic factors that inhibited family participation, staff attitudes also had effects. Greater support for family involvement was found among older staff members, female staff, professional staff, and staff members who felt that they knew the families better (
10). In a study conducted two years after a large residential treatment center had adopted a family-centered approach, Coleman (
11) found that attitudes about family involvement varied by staff members' positions and educational achievement. Administrators and persons with more education supported higher levels of family involvement.
Some efforts have been made to examine factors that may facilitate or hinder family participation. For example, Kazdin and colleagues (
12) developed a measure of barriers to treatment participation to assess factors that contribute to families' early withdrawal from participation in therapy. Four subscales were developed to measure stressors and obstacles that compete with treatment, treatment demands and issues, perceived relevance of treatment, and relationship with the therapist. Ratings on the scale were predictive of missed appointments and early dropout from treatment. These barriers that were measured significantly affected treatment outcomes for children with conduct disorder and their families.
Even less is known about supports for participation than about barriers to participation. Baker and associates (
9) concluded that agencies should plan to provide outreach services and resources to engage families who live at a great distance. Friesen and colleagues (
13) conducted focus groups of family members with children who were receiving mental health treatment in out-of-home settings. The family members described several factors that facilitated their participation, including staff behaviors, such as sharing information and being supportive, and agency practices, such as providing meals and providing opportunities for contact with other families.
Many of the previous studies in this area were limited by analyses that included aggregated groups of youths with mental retardation and youths with mental health problems. Thus it is difficult to ascertain to whom the findings apply. In addition, study findings from a single facility or from a few facilities that are part of the same corporation are difficult to generalize. The current study addressed these limitations through a national survey of family caregivers of children with behavioral and emotional issues who were receiving community or out-of-home treatment. This study was conducted to identify the caregivers' characteristics and amount of participation in their children's treatment as well as their perceptions of barriers and supports to their participation.
In this study we focused on the following three dimensions of caregivers' participation in children's out-of-home care: contact between the family caregivers and the child, educational planning, and service or treatment planning.
Methods
Sample and survey procedures
Eligible study participants were parents or other family caregivers with primary responsibility for youths from birth to age 20 years who had received at least three months of in-home treatment or at least 30 continuous days of out-of-home treatment for emotional, behavioral, or mental disorders between September 1, 1996, and August 31, 1998. This cross-sectional study used a sample of caregivers recruited through randomly selected chapters of the Federation of Families for Children's Mental Health and the mailing list of the Research and Training Center on Family Support and Children's Mental Health. Participation was anonymous; questionnaires were returned with no identifying information. Portland State University's institutional review board approved the study. The data were collected during 1999 and 2000.
Measures
In addition to including questions about demographic characteristics, the study questionnaire addressed topics related to family participation in children's out-of-home treatment, including contact between parents and children and caregivers' involvement in educational planning and service or treatment planning. Family caregivers were asked to indicate how often they spoke with the child by telephone, how often they made on-campus and away-from-campus visits, and how often the child came home for visits after the initial adjustment period. The response choices were "daily," "two to six times per week," "weekly," "two to three times per month," "monthly," "six to 11 times per year," "one to five times per year," and "never." The total amount of contact was calculated by converting responses for each type of contact into contact episodes per day and summing them.
Family caregivers were asked to rate their satisfaction with each type of contact by using a 4-point continuum from 1, "extremely dissatisfied," to 4, "extremely satisfied." The mean±SD satisfaction rating for the different types of contact was used for the analysis (mean=3.05±.65).
We examined the two domains of educational planning and service or treatment planning by including parallel sets of 12 questions about participation in each domain. Caregivers were asked to respond to the questions on a 4-point continuum on which 1 represented "not at all"; 2, "some"; 3, "a little"; and 4, "a lot." Examples of items are, "To what extent were your ideas valued in education planning for this child?" and "How much did staff make changes in the educational plans as a result of your suggestions?" As a result of principal-components analysis, each measure was reduced to seven items. Cronbach's alpha for the retained items was .93 for the educational planning measure and .95 for the service or treatment planning measure. The two measures were moderately correlated (r=.55, p<.001), indicating that similar but distinct constructs were being measured.
Results
The total number of survey forms received for the entire sample was 486. A total of 114 usable surveys were returned from family caregivers in 31 states whose children were in out-of-home care, for a response rate of 57 percent. The response rate for families whose children were receiving services while living at home did not differ from the response rate for families whose children were in out-of-home care. The analysis focused on a subset of the sample consisting of 102 parents whose children received out-of-home treatment in a residential treatment center (68 respondents, or 67 percent), a psychiatric hospital or psychiatric unit (21 respondents, or 21 percent), or a group home (13 respondents, or 13 percent).
Chi square and t test analyses indicated no significant demographic differences among families and children being served in the three settings in terms of caregivers' marital status, income adjusted for family size, caregivers' education, children's gender, ethnicity, age, children's number of diagnoses, and age at onset of the children's emotional, behavioral, or mental health problems. The only statistically significant difference among the three groups was legal status at the time of placement: the state had legal custody of eight (38 percent) of the children in group homes, five (12 percent) of those in residential treatment, and one (5 percent) of those in psychiatric hospital settings (χ2=8.04, df=2, p<.02). Because of the similarities across the three groups, the groups were aggregated for the rest of the analyses.
Eight male and 94 female caregivers reported on 74 boys and 28 girls. Most of the respondents were birth mothers (70 respondents, or 69 percent) or adoptive mothers (19 respondents, or 19 percent). More than half of the family caregivers (54 respondents, or 53 percent) had a college degree, and the median yearly household income ranged from $35,000 to $44,999. Although the median income range appears high in light of U.S. household income data, 17 respondents (17 percent) had very low incomes (less than 50 percent of the U.S. median), and one-half of those families were at or below the federal poverty threshold (
14,
15).
Seventy-eight respondents (78 percent) had legal custody of their children at the time of placement. A majority of those without legal custody (11 respondents, or 52 percent) reported relinquishment of parental rights as a prerequisite for state funding of services (
16). Eighty (78 percent) of the children described by their caregivers were white, nine (9 percent) were African American, six (6 percent) were multiracial, three (3 percent) were Hispanic, and two (2 percent) were Native American. The mean±SD age at which parents reported that they first noticed the child's problems was 6.1±3.8 years, and the child's mean age at first receipt of mental health services was 7.2±3.7 years.
The mean age of the children at the time of data collection was 14.1±3.1 years, with a range from 6.7 to 20.6 years. Eighty-nine children (89 percent) had more than one diagnosis (mean number of diagnoses=3.9± 2.1). The most common reported diagnoses were attention-deficit hyperactivity disorder (50 children, or 49 percent), bipolar disorder (43 children, or 42 percent), and oppositional defiant disorder (41 children, or 40 percent). The mean accumulated length of out-of-home placement over the two-year study period was 13.8±7.6 months. About one-third of the children (35 children, or 34 percent) were reported to have had more than one out-of-home placement during the two-year study period.
Caregiver-child contact
Of the different forms of contact, telephone contact occurred most frequently: 90 (88 percent) of the parents reported telephone contact at least once a week; 63 (63 percent), 33 (33 percent), and 23 (24 percent) reported that visits occurred once a week or more on campus, off campus, and at home, respectively. The total amount of contact varied with the child's age, distance from home to the placement, and limits on contact. Younger children had more contact with their families (r=-.29, p<.01), as did children in treatment facilities closer to home (r=-.26, p<.05). No significant differences were found in the frequency of contact on the basis of the children's sex, race, or severity of condition, nor were significant differences found on the basis of the caregivers' characteristics, such as sex, race, age, income, education, custody status, or marital status. Caregivers who reported less total contact reported less satisfaction with the amount of contact (r=.36, p<.01).
Caregiver participation
The mean±SD rating on the measure of participation in educational planning was 2.77±.91, between "a little" and "some," with a range of ratings from 1 to 4. Ratings on the measure of participation in service or treatment planning were similar, with a mean rating of 2.88±.88, between "a little" and "some," and a range of ratings from 1 to 4.
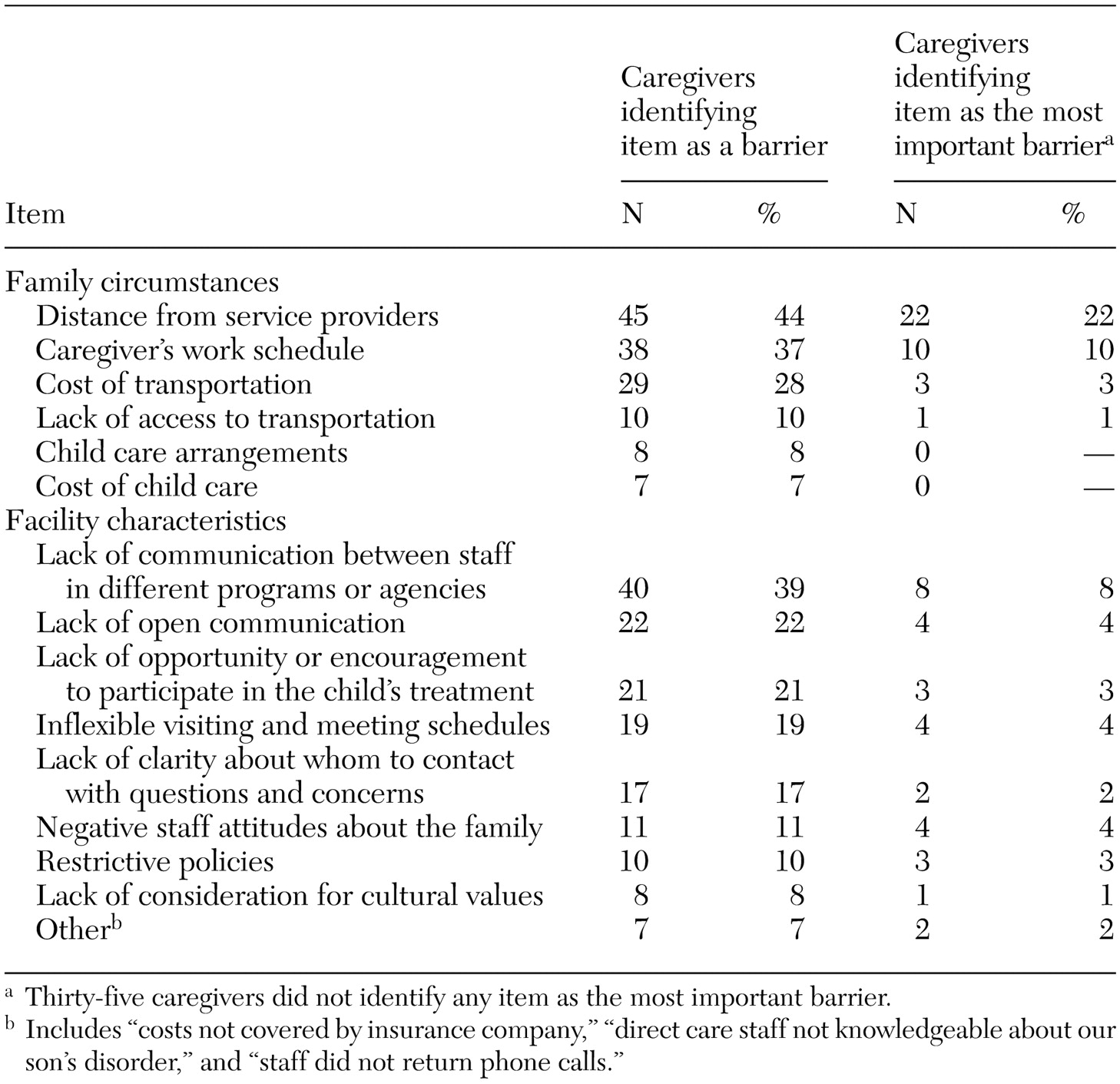
Barriers to participation
Caregivers were presented with a list of potential barriers and were asked to check all items describing things that made it difficult for them to participate in their children's education or treatment. The items on the measure of barriers to participation are shown in
Table 1, which also shows the percentage of family caregivers who selected each item and, for each item, the percentage of caregivers who selected the item as the most important barrier. For the analysis, the barriers were divided into two groups: family circumstances and facility characteristics. Distance from service providers was the most frequently identified family circumstance that was a barrier to participation in treatment. The most frequently identified facility characteristic was the lack of communication between staff in different programs (reported by 40 respondents, or 39 percent). Among the 67 caregivers who endorsed a particular barrier as the greatest hindrance to participation, distance to service providers was the most frequently identified barrier.
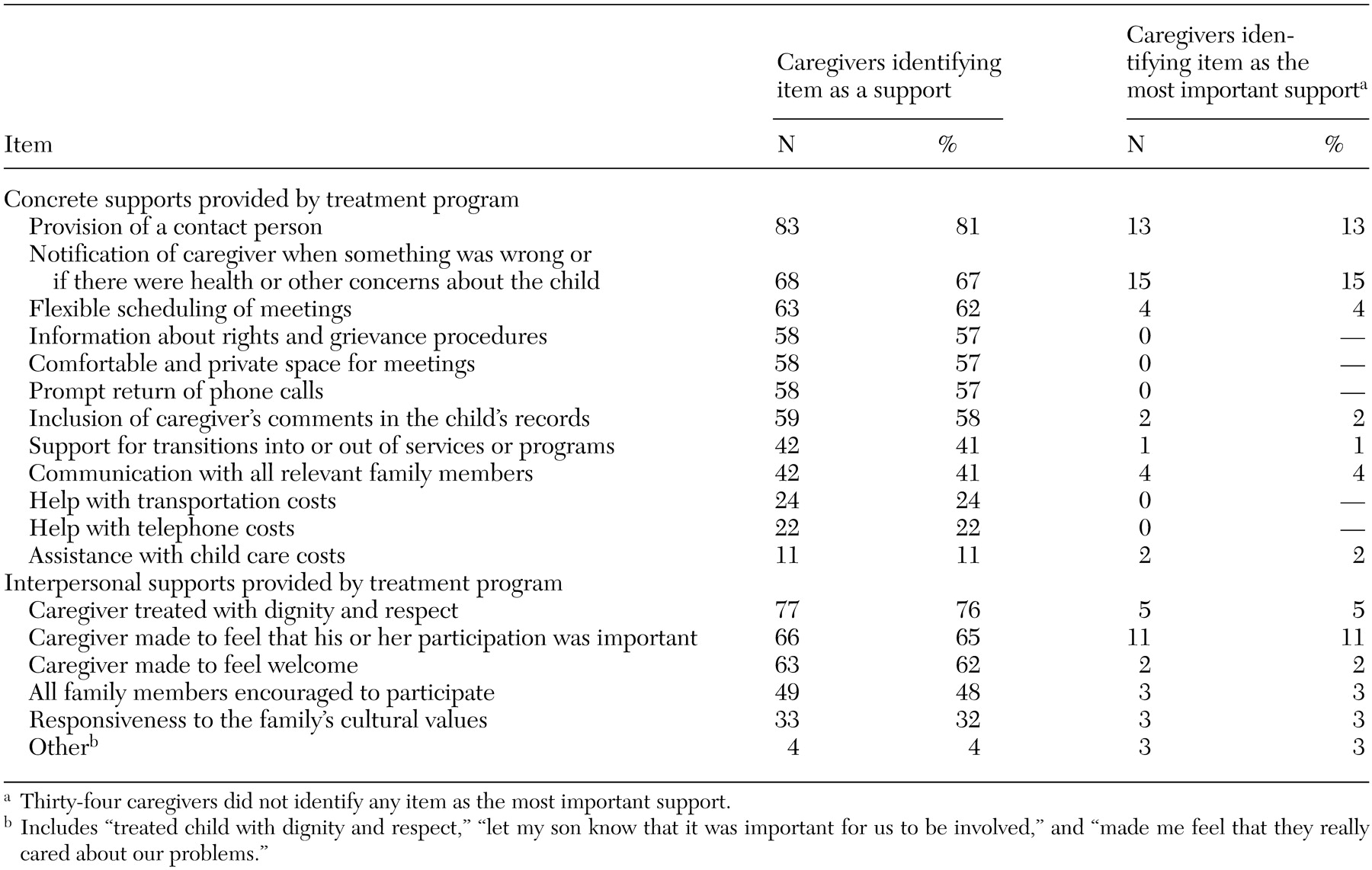
Supports to participation
Caregivers were presented with a list of possible supports to participation and asked to check "all the ways that program staff or case workers supported your participation in your child's out-of-home care."
Table 2 lists the items in the two categories of staff support developed for this analysis—concrete and interpersonal supports—and indicates the supports most frequently identified by caregivers as well as the supports that were considered most important. The most frequently mentioned support was the provision of a contact person, checked by 83 caregivers (81 percent). Of the 68 caregivers (67 percent) who named a particular support as most important, the highest ranking was given to notification when something was wrong or when there were health or other concerns involving the child, followed closely by provision of a contact person.
Importance of barriers and supports
To assess the relationship of barriers and supports to measures of participation and family caregivers' satisfaction, summed indexes were developed from the items listed in
Table 1 and
Table 2. The alpha coefficients of .72 for the barriers index and .87 for the supports index reflect high internal consistency for the two measures. Family caregivers' reports of more barriers were associated with less total contact with the child (r=-.43, p<.01), a lower rate of participation in educational planning (r=-.55, p<.01), a lower rate of participation in treatment planning (r=-.65, p<.01), and less satisfaction with the amount of contact (r=-.54, p<.01).
Conversely, family reports of more supports were associated with having more total contact with the child (r=.24, p<.05), a higher rate of participation in educational planning (r=.66, p<.01), and a higher rate of participation in service or treatment planning (r=.79, p<.01). The more supports families perceived, the higher they rated their satisfaction with the amount of contact (r=.56, p<.01).
Discussion and conclusions
In 1989, Jenson and Whittaker (
17) identified barriers and proposed specific policies and strategies for increasing parental involvement at each stage of the placement process. Many of the barriers described by Jenson and Whittaker are reflected in the findings of the study reported here.
Furthermore, the findings of this study support the important relationship between family caregivers' perceptions of barriers and supports and their participation in their children's out-of-home treatment. Although family participation has generally been viewed as a function of the geographic and demographic characteristics of the child and the family, these results underscore the importance of the policies and practices of placement facilities and the attitudes of staff members. Perceived parental resistance or reluctance to participate in their child's treatment may be reframed as a need for resources to pay for transportation or the need for additional encouragement to participate.
Although, to our knowledge, no outcome studies have documented negative consequences of family involvement, staff member may perceive family visits as disruptive or upsetting to children, and parents may perceive that staff members blame them for their children's difficulties (
7). Professionals' perceptions of families as causal agents in their children's mental illness and their negative attitudes toward parents are believed to constrain family participation in treatment (
18,
19).
This study had several limitations. Because no listings are available to identify families whose children have received mental health services, a sampling frame was created on the basis of lists from organizations that provide services and supports to this population. Although our sampling strategy allowed us to survey a national sample of parents, the sample did not fully represent the population of interest—caregivers of children with serious emotional problems—in that it included only caregivers who chose to be added to a national mailing list or who were connected to family organizations. These caregivers represent only a small proportion of all families of children with serious emotional disorders, and they may differ from the wider population of family caregivers in several ways. For example, members of family organizations are perhaps more likely than other caregivers to be aware of their rights to participate in their children's treatment and to have advocacy skills. Previous studies have found that parents who are very rich or very poor tend not to be members of support organizations (
20,
21). The caregivers in this study may represent those who have had the most positive experiences caregivers are likely to have. Future research would benefit from efforts to obtain a more representative sample and efforts to identify more clearly which barriers and supports are most germane to each of the multiple dimensions of family participation.
These findings offer staff members information that can be used in reviewing their programs and considering possible changes. Addressing barriers such as the costs of transportation or providing overnight accommodations will involve additional resources. Family caregivers' perceptions of whether they are being treated with respect and being made to feel welcome are intangible, and programs will need to make additional efforts to find out how caregivers experience the programs' services and what changes will be most supportive of caregivers' involvement.
Acknowledgments
This work was supported by the National Institute on Disability and Rehabilitation Research, the U.S. Department of Education, and the Center for Mental Health Services of the Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Services (grant H122B40021-96, 97).