The basal ganglia play an important role in the regulation of emotions, mood, motivation, and cognition, in addition to motor control. Although much has been written about the role of the basal ganglia in motor functions, less is known about their role in neuropsychiatric conditions. Idiopathic Parkinson's disease (PD) and progressive supranuclear palsy (PSP) are the most common hypokinetic basal ganglia disorders. Clinically, PD is characterized by unilateral onset of resting tremor, rigidity, and bradykinesia and later development of postural instability, whereas PSP is characterized by prominent postural instability at symptom onset, followed by development of symmetric bradykinesia and rigidity as well as vertical supranuclear ophthalmoparesis.
Five frontal-subcortical circuits unite the basal ganglia with regions of the frontal lobe and thalamus in functional systems that mediate motor, cognitive, and emotional behavior. Thus, it is not surprising that behavioral abnormalities, reflecting interruption of these circuits, are present in basal ganglia disorders such as PSP and PD. In both disorders there is involvement of the substantia nigra neurons and striatal dopaminergic depletion, but there are important neuroanatomic and neurochemical differences between these disorders. Anatomically, PSP patients have greater involvement of additional basal ganglia nuclei (i.e., putamen, globus pallidus, caudate, and subthalamus) and the orbitofrontal and medial frontal circuits than PD patients. Neurochemically, mesocortical dopaminergic, serotonergic, and noradrenergic nuclei are more severely affected in PD than in PSP.
1We compared the Neuropsychiatric Inventory (NPI)
2 scores in two clearly defined samples of PSP and PD patients to better understand the neurobiological basis for the psychiatric symptoms observed in these two hypokinetic disorders. After considering the differential neuroanatomical and neurochemical involvement, we hypothesized that PSP patients would manifest symptoms associated with disruption of the orbitofrontal (disinhibition) and medial frontal (apathy) circuits, whereas PD patients would exhibit symptoms related to monoaminergic dysfunction (e.g., depression, hallucinations). Because the psychiatric symptoms in these disorders may be secondary to the disease process, to drugs acting on the brain, or to interaction between the disease process and medications, we were careful to control for patients' medication and disease stage, in addition to their demographics.
RESULTS
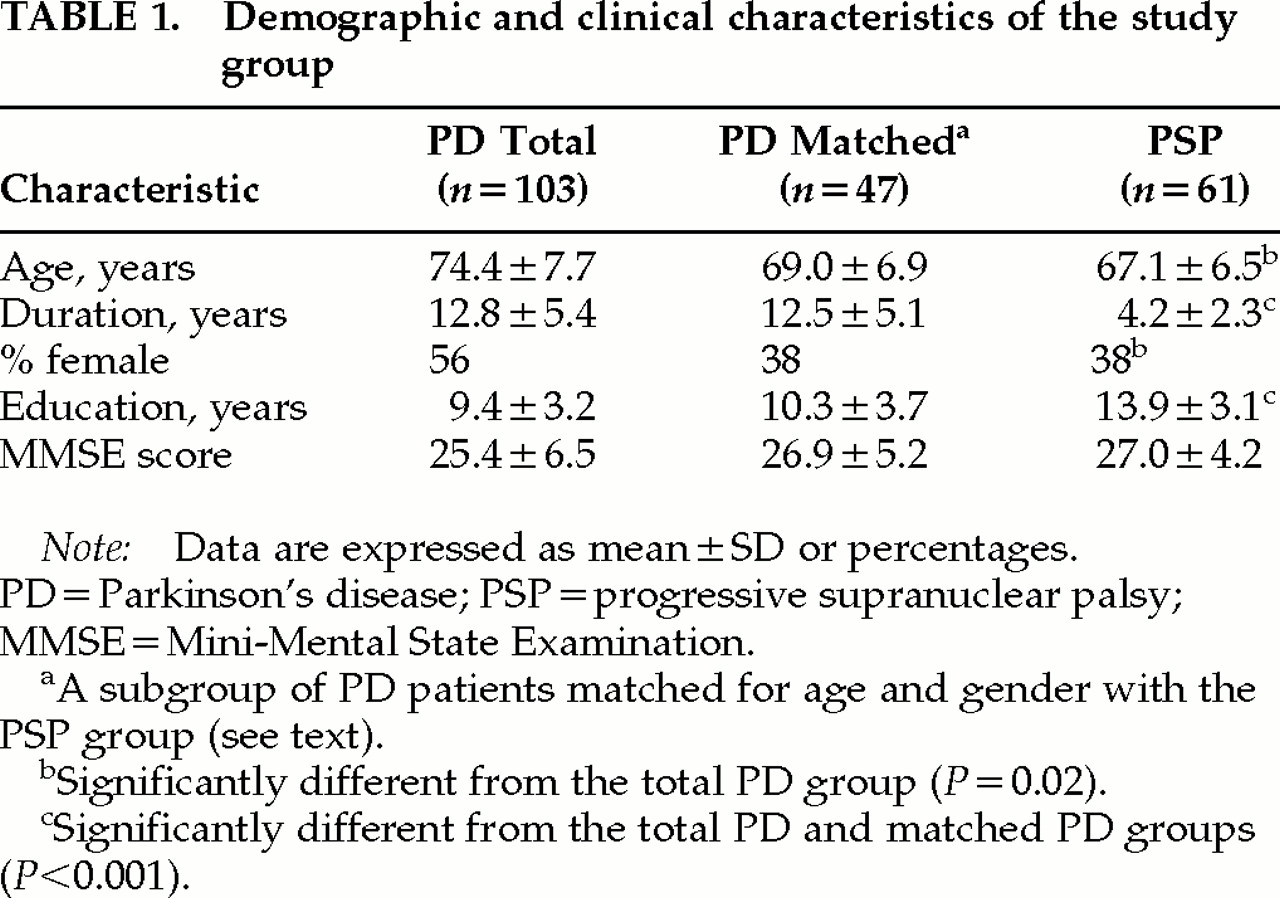
The PD full data set group was older, included more women, had a longer disease duration, and had fewer years of education than the PSP group (
Table 1). MMSE scores did not differ between groups (
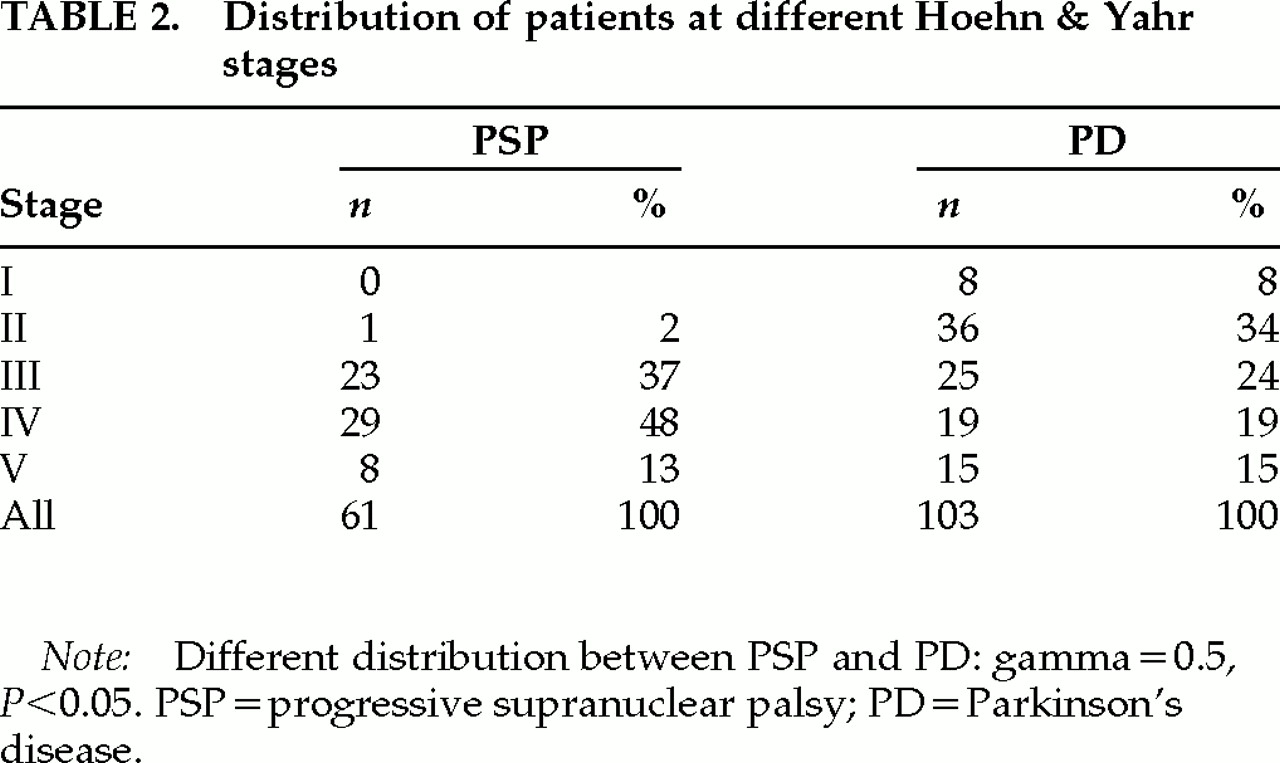
Table 1). The PSP patients had more advanced parkinsonism (
Table 2). To control for the potential influence of disease severity, medication, and age and gender distribution, we first compared the NPI scores for PSP and PD patients at similar Hoehn and Yahr stages. Subsequently, to control for differences in the use of medication, we compared only patients treated with dopaminergic agents. Finally, we compared the PSP group with a gender- and age-matched PD group.
Neuropsychiatric Symptoms and Disease Stage
Linear regression analyses were performed to examine the relationship between total NPI scores and Hoehn and Yahr stages. A significant relationship was found in PD patients (
F=10.2,
P=0.002), but not in PSP patients (
F=1.0,
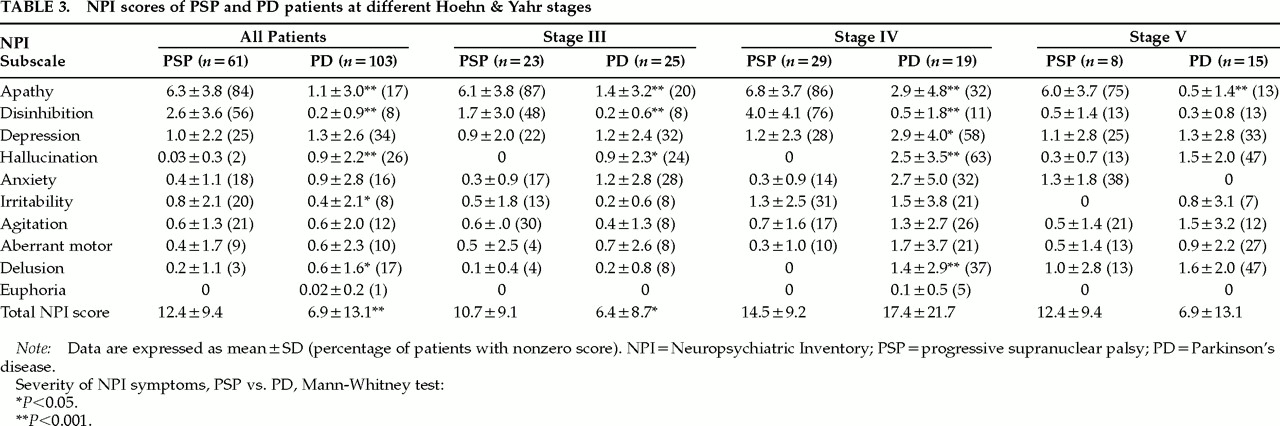
P=0.31). Only one PSP patient had a Hoehn and Yahr stage less than III. NPI scores in PSP and PD patients with Hoehn and Yahr stage III or later were compared (
Table 3). In subjects at stage III, a higher total NPI score was found in PSP than in PD patients (
z=2.1,
P<0.05). In patients at stage IV, the total NPI score was higher in PD patients than in PSP patients (
Table 3), but the difference was nonsignificant (
z=0.9,
P=0.3).
A double dissociation of neuropsychiatric symptoms in PSP and PD patients was found: PSP patients showed higher scores on apathy and disinhibition than PD patients, whereas scores for hallucination, delusion, and stage IV depression were higher in PD patients compared with PSP patients (
Table 3). This pattern of neuropsychiatric symptoms was consistent through the Hoehn and Yahr stages III, IV, and V. However, because of a small sample size, only the difference in apathy score reached statistical significance in patients at stage V.
Neuropsychiatric Symptoms and Medications
Neuropsychiatric symptoms may occur as a side effect of antiparkinsonian drugs.
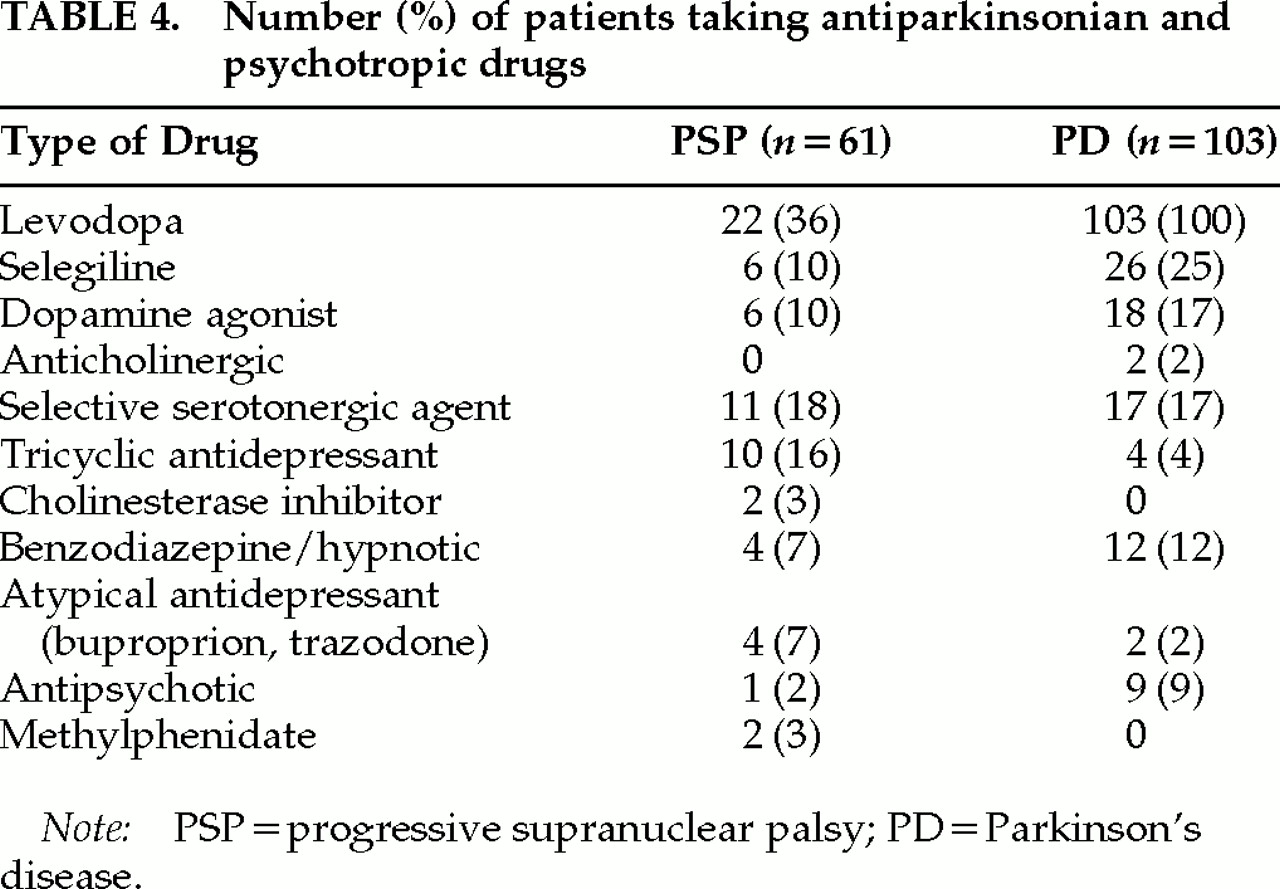
12 To investigate if the observed difference in neuropsychiatric symptoms between PSP and PD patients was associated with dopaminergic treatment, the NPI scores in PSP and PD patients who were taking antiparkinsonian agents were compared. The number and dosage of antiparkinsonian and psychotropic medications are shown in
Table 4. All PD patients were taking levodopa. The mean dose was 632 mg/day (SD=382), and the mean duration of treatment was 10.1 years (SD=4.8). Fifty-nine patients (57%) took one antiparkinsonian agent, 40 patients (39%) took two, and 4 patients (4%) took three. In the PSP group, 27 patients (44%) were taking antiparkinsonian drugs. Twenty-two subjects (36%) were taking levodopa. The mean dose of the PSP subjects taking levodopa was 593 mg/day (SD=300), not significantly different from that of the PD group (
t=0.4,
P=0.7). Eighteen PSP patients (29%) were taking one antiparkinsonian drug, and 9 (15%) were taking two. Thus, the proportion of patients taking dopaminergic drugs was higher among PD than among PSP patients (gamma=0.85,
P<0.001). There were no differences in the average dosage of dopaminergic agents (measured as percentage of DDD) between the 25 PSP subjects who took levodopa and/or a dopamine agonist (93%, SD=55) and the PD subjects (115%, SD=73;
t=1.4, df=126,
P=0.17).
The NPI scores in PSP and PD subjects with similar disease severity (i.e., Hoehn and Yahr stage III or later), who took one or two antiparkinsonian drugs were compared. The results were similar to those reported above. PSP patients had higher apathy (P<0.001) and disinhibition (P<0.001) scores as well as total NPI score (P<0.001) than PD patients. Hallucination (P<0.001), delusion, (P<0.05), and depression (P<0.05) scores were higher in patients with PD than in those with PSP. Finally, NPI scores in PSP (n=16) and PD (n=59) subjects receiving levodopa monotherapy were compared. Scores for apathy (z=4.3, P<0.001), disinhibition (z=5.1, P<0.001), irritability (z=2.0, P<0.05), and total NPI (z=2.9, P<0.005) were higher in PSP than PD patients, whereas more severe hallucination scores were found in PD (z=2.0, P<0.05). Hallucination and delusion scores were not associated with the number of dopaminergic agents, the daily levodopa dose, or the percentage of DDD in PSP or PD patients. There was no association between duration of treatment and psychotic symptoms in PD patients.
Many subjects were treated with psychotropic drugs (
Table 4). Twenty-one PSP patients (34%) and 22 PD patients (21%) were taking one or two antidepressants. There were no between-group differences in dosages of selective serotonin reuptake inhibitors or tricyclic antidepressants. Nine PD patients were taking clozapine (
n=7, dose range 12.5–75 mg/day) or another antipsychotic agent, compared with one PSP patient who was taking neuroleptics prn (Fisher's exact test,
P=0.09). To control for the possible confounding effect of antidepressants, PSP and PD patients who were not taking antidepressants were compared. No differences in anxiety and depression scores between PSP and PD patients were found, and the results on other NPI symptoms were also similar to those obtained when all subjects were included.
Neuropsychiatric Symptoms in PSP and PD Patients Matched for Age and Gender
Subsequently, we selected PD subjects matched with the PSP group according to gender and age. As seen in
Table 1, the age- and gender-matched PD subjects had longer disease duration and fewer years of education than the PSP patients. However, with the exception of a high correlation between the disinhibition score and duration of disease in the PD group, (
r=0.33,
P<0.01), the NPI scores did not correlate with disease duration or length of education in either group of patients.
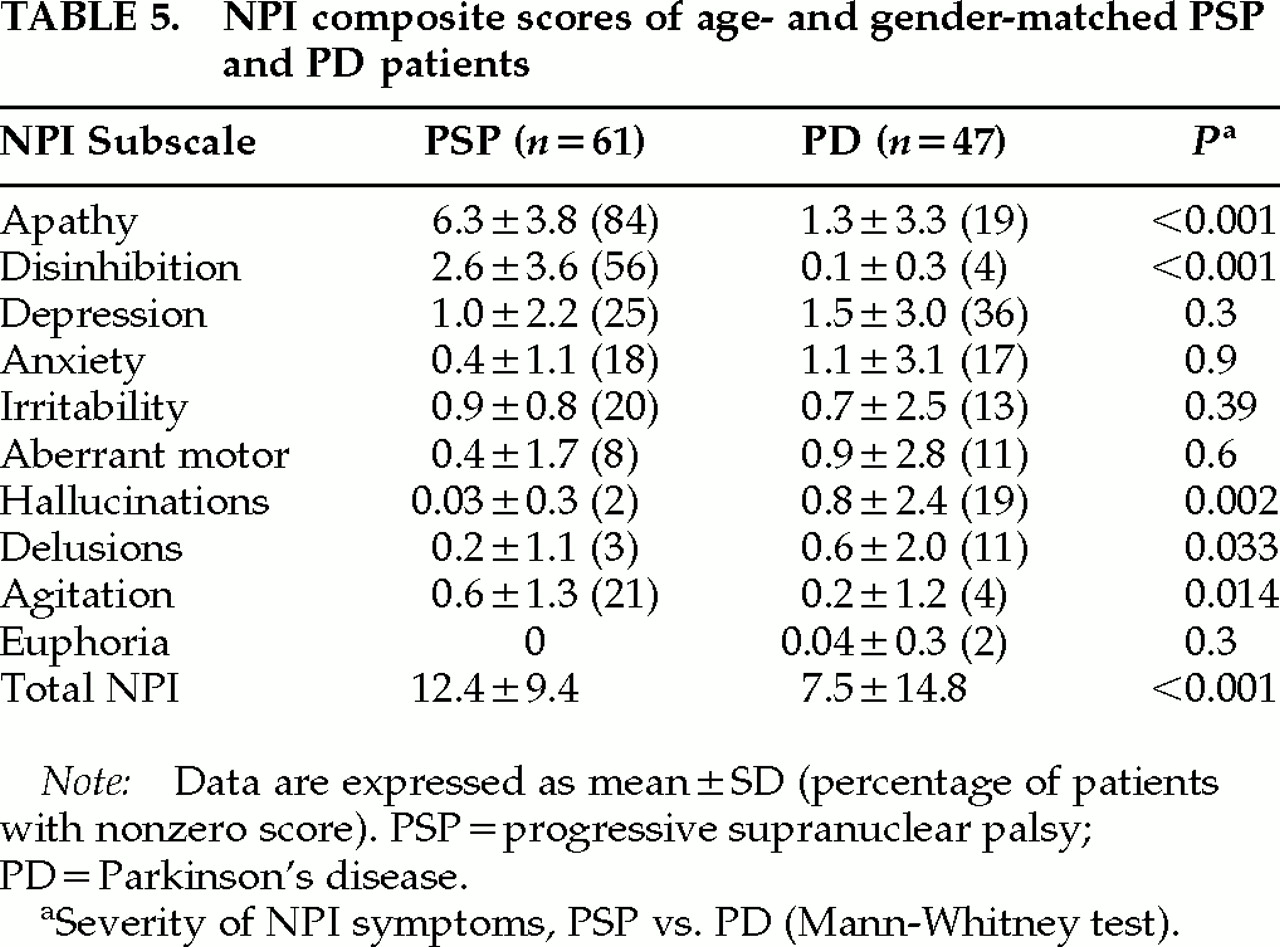
As shown in
Table 5, the PSP patients exhibited more neuropsychiatric symptoms, as measured by the total NPI score, than the age- and gender-matched PD group. The same disease-specific pattern of neuropsychiatric symptoms as found above emerged, with higher apathy and disinhibition scores in PSP patients and higher hallucination and delusion scores in the PD group. Fifty-six (92%) of the PSP patients had a positive score on at least one NPI symptom, compared with 25 (53%) of the PD patients (
z=3.6,
P<0.001).
DISCUSSION
The main finding in this study was a differential pattern of neuropsychiatric symptoms in patients with PSP and PD. Apathy and disinhibition were more common and severe in PSP patients, whereas hallucinations and delusions were more frequent in patients with PD. Depression was more severe in patients with PD than in those with PSP in subjects with Hoehn and Yahr stage IV, and in those receiving dopaminergic agents. Thus, the results support the hypotheses that neuropsychiatric symptoms are associated with the involvement of selected frontal-subcortical circuits in PSP, and distinct subcortico-cortical monoaminergic nuclei in PD. Neuropsychiatric symptoms were more common and severe in PSP than in PD, possibly due to the more widespread involvement of the basal ganglia in PSP.
1This is the first study comparing the neuropsychiatric symptoms of patients with these two hypokinetic movement disorders, although the neuropsychiatric features of PSP
4,13 and PD patients
8 have already been previously reported. The relatively large study sample, the use of a standardized and validated instrument to assess psychiatric symptoms in patients with brain disorders, and the use of specific inclusion and exclusion criteria for the diagnoses of PSP and PD
3,6 are the strengths of this study. Although the diagnostic criteria for PSP used in this study is highly specific and reliable,
14 occasionally it may be difficult to distinguish PSP from PD during the first 2 years of symptom onset when postural instability or ophthalmoplegia present late in the course of PSP.
15,16 To avoid this, several mutually exclusive criteria were used for the diagnoses of PSP and PD in the current study. Patients with a clinical diagnosis of PD and early hallucinations may in fact suffer from dementia with Lewy bodies.
17 Therefore, patients with features compatible with a diagnosis of probable DLB were not included in the PD group. Asymmetrical parkinsonism early in the disease, resting tremor, and excellent levodopa response, which were required for the diagnosis of definite PD in our study, are highly predictive of PD rather than DLB.
15 Inclusion of PSP or DLB patients in the PD group is therefore unlikely.
The differences in demographics and case ascertainment limit the interpretation of this study. The PD patients were drawn from an epidemiological study with high case ascertainment,
5 whereas the PSP patients consisted of patients referred to a tertiary care facility. This group may thus not be representative of the general PSP population, but it is difficult to ascertain enough subjects with PSP from the general population. Because only PD patients with a disease duration of at least 4 years were included, PD patients with a short disease duration and mild severity are underrepresented. This factor also limited our ability to explore if depression is more frequent during the early stages in PD than in PSP. On the other hand, because PSP is a rapidly progressing disease with a survival time of only 5 to 7 years,
18 inclusion of earlier and milder PD patients with shorter disease duration and thus less severe parkinsonism would have increased the difference in motor impairment between the two groups. Given the strong association between disease stage and neuropsychiatric disturbances in PD, this would have further increased a stage-dependent difference in neuropsychiatric morbidity between the two groups.
Other potential limitations can be noted. The differences in age, gender distribution, and years of education may have had an impact on the observed differences in neuropsychiatric symptoms; there were a few minor associations between NPI scores and demographic variables. However, after controlling for the differences in gender distribution and disease severity, the principal findings of this study were still evident. The NPI raters were not blind to diagnosis, but they were unaware of the hypotheses of the study at the time of assessment. Lack of interrater reliability assessment limits the strength of the findings, but the NPI has been shown to have acceptable reliability in previous studies.
2 Since it is caregiver rated, it may not be as accurate as symptoms rated by a clinician with input from a patient interview. We used the official Norwegian version of the NPI, which has been retranslated into English and authorized by the constructor of the instrument. Finally, no attempt was made to control for multiple comparisons. Accordingly, some statistically significant differences might have occurred by chance. However, the principal findings were robust and occurred in nearly all of the different comparisons performed.
Our findings of more severe apathy and disinhibition in PSP than PD are consistent with previous neuroanatomical and neuroradiological reports of a more marked involvement of the orbitofrontal and medial frontal circuits in PSP than in PD.
1 These conclusions extend previous findings of more severe executive impairment in PSP than in PD patients,
19 suggesting a greater involvement of also the dorsolateral frontal-subcortical circuit in PSP.
Hallucinations in PD patients are usually considered to represent a side effect of dopaminergic treatment.
12 However, several recent reports have suggested that other factors may be important. Hallucinations in PD were not associated with the number, dosage, and duration of treatment with dopaminergic agents (consistent with previous studies
20,21) and do not relate simply to the high levels or sudden changes in plasma levels of levodopa.
22 Almost half of the PSP patients in our study were taking dopaminergic agents, and surprisingly, the dosages of these agents were similar in PSP and PD patients. Dopaminergic agonists, which induce hallucinations more often than does levodopa, were somewhat more frequently administered in PD than PSP patients. Nevertheless, hallucinations were reported in only 1 of the 27 PSP patients who were treated with dopaminergic agents, compared with 27 of the 103 PD patients. Similar results emerged in the subgroup of patients on levodopa monotherapy. PD patients had longer disease duration and had been treated with dopaminergic agents for a longer time than the PSP patients. Theoretically, long-term dopaminergic treatment might increase the risk for hallucinations, possibly via dopamine receptor hypersensitivity.
23 However, in the present and other studies,
20,24,25 there was no association between the duration of levodopa treatment and risk for hallucinations in PD. Thus, although the study design precludes identifying the effect of dopaminergic medication on neuropsychiatric symptoms in the PD group, the results indicate that other factors contribute to hallucinations and delusions in PD.
It has been suggested that cortical cholinergic loss,
26,27imbalance of serotonergic-dopaminergic neurotransmission,
28 or poor visual discrimination
29 might contribute to hallucinations in PD patients. Cholinergic loss occurs in both PSP and PD patients. Although cholinergic loss is more severe in PSP than PD
1, there is some evidence suggesting a greater loss of cholinergic innervation to the cerebral cortex in PD, whereas there is a preferential loss of cholinergic innervation to the thalamus in PSP.
30 Monoaminergic nuclei are more involved in PD than in PSP patients.
1 These neurochemical differences are possible explanations for the finding of more frequent hallucinations in PD than in PSP patients.
Psychiatric symptoms in basal ganglia disorders are treatable
31 conditions with significant consequences for the care of patients
32 and the well-being of their caregivers.
33 The evaluation and treatment of neuropsychiatric abnormalities in patients with basal ganglia disorders may improve the quality of life for both patients and their caregivers. Our findings provide insight into the neurobiology of psychiatric symptoms in basal ganglia disorders, but neuroimaging and neuropathologic studies are needed to confirm these relationships.