The Phenomenology of Personality Change Due to Traumatic Brain Injury in Children and Adolescents
Abstract
METHODS
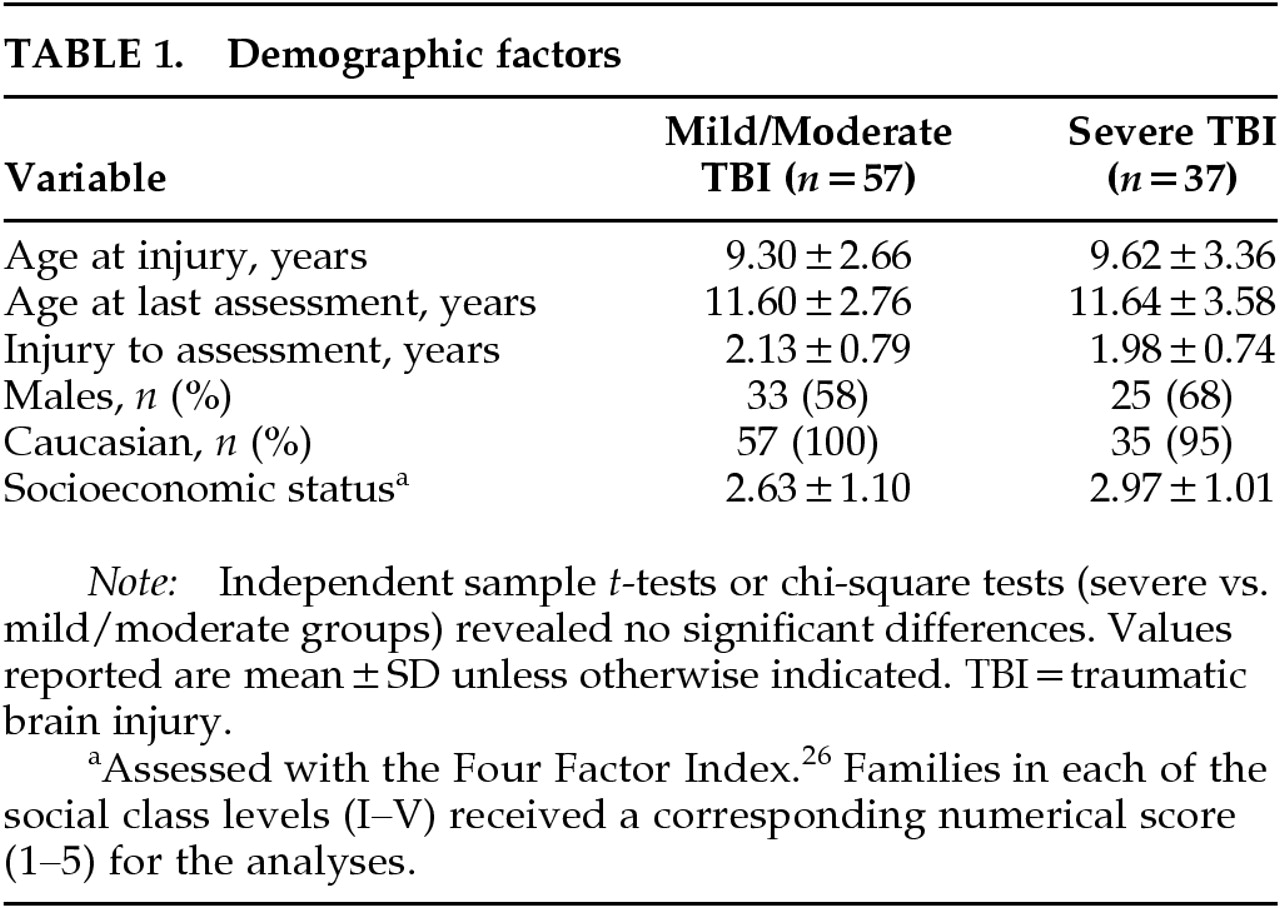
Subjects
Prospective Study
Retrospective Study
Psychiatric Measures
RESULTS
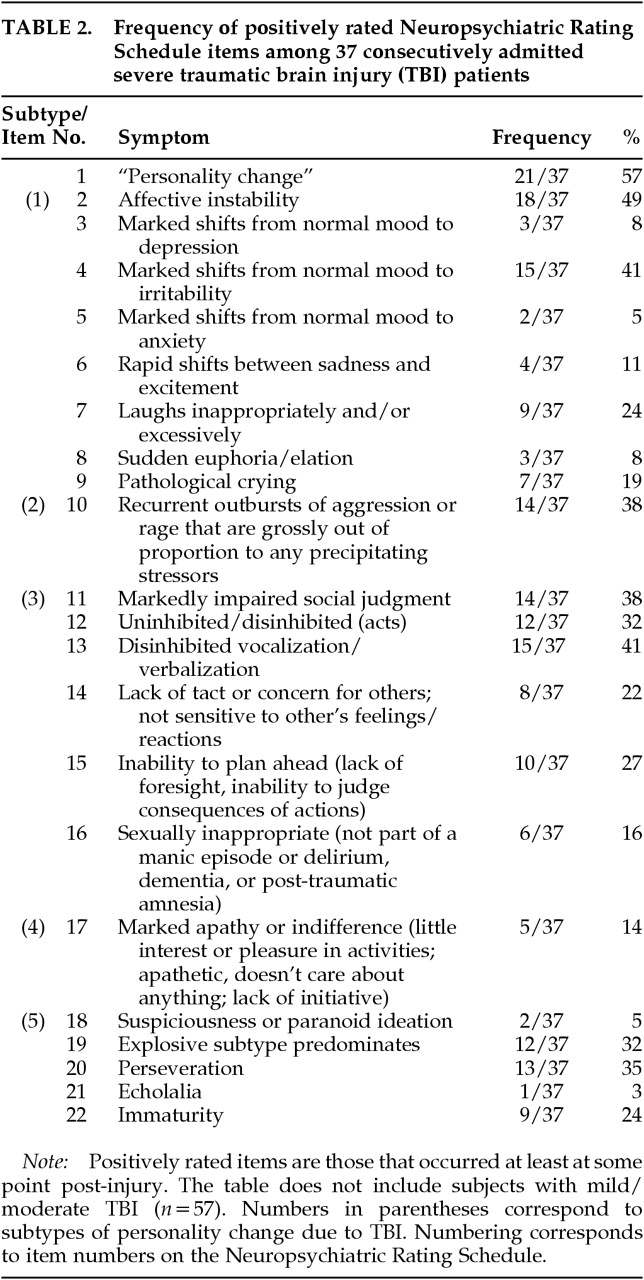
Personality Change (NPRS item #1):
Affective Instability/Labile Subtype (NPRS items #2–9)
Aggressive Subtype (NPRS item #10)
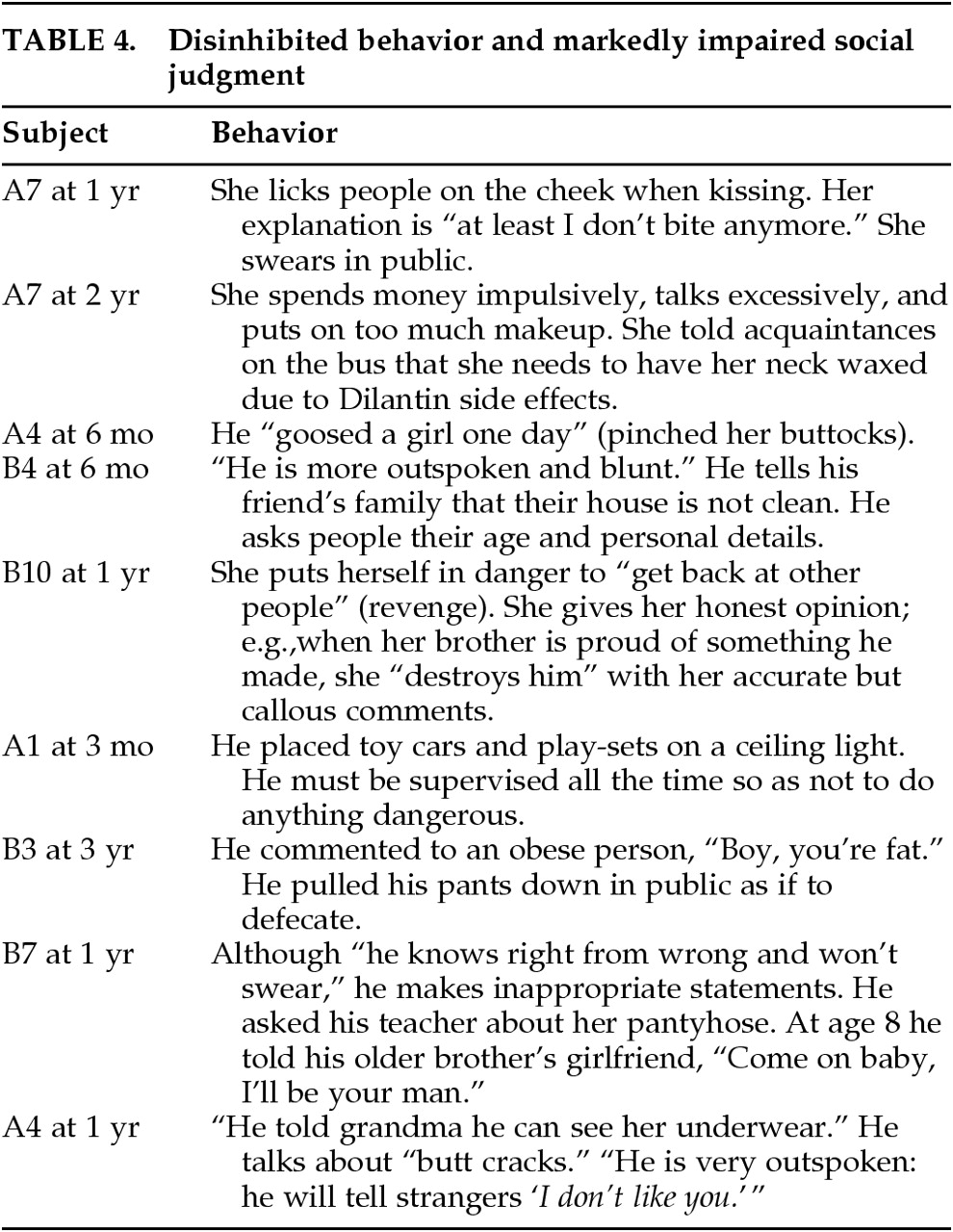
Impaired Social Judgment Subtype (NPRS items #11–16)
Apathetic Subtype (NPRS item #17)
Suspicious or Paranoid Subtype (NPRS item #18)
Other Symptoms Associated With PC (NPRS items #20–22)
CASE REPORT
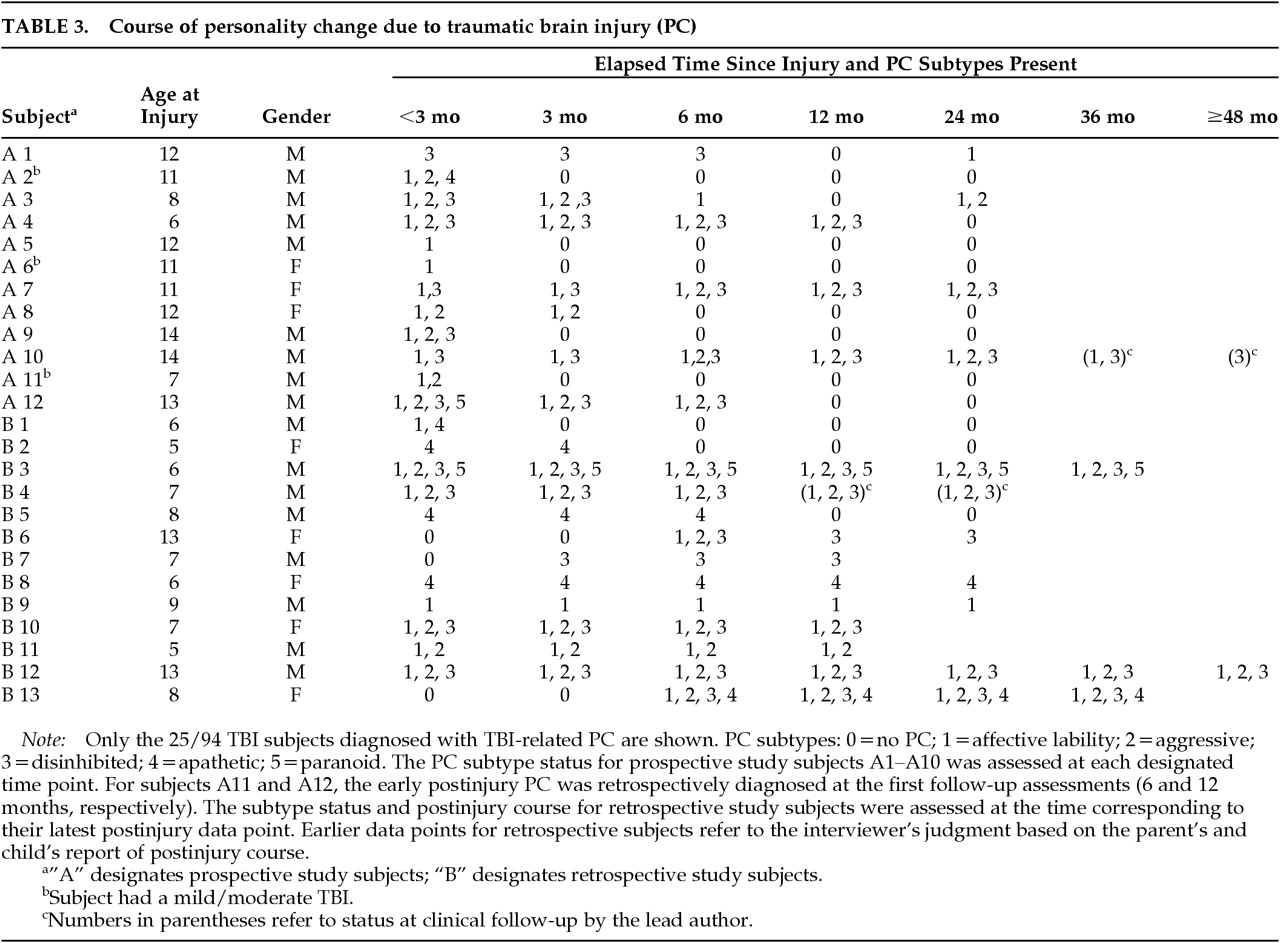
Subject A10 (Table 3). This 14-year-old white male was thrown over the handlebars of his bicycle. He landed on his unhelmeted head on a dirt road. A baseline K-SADS conducted with his parents 7 days after his TBI revealed that he had never met criteria for a psychiatric disorder before injury. His parents described him as “well-mannered, well-behaved, and polite,” a person who “goes with the flow.” He had no history of emotional lability, violent behavior, inappropriate social judgment, apathy, or paranoia. He planned ahead, for example, by saving money for a fishing pole.He was motivated by the challenges at school. His academic achievement was average and his preinjury score on his Iowa Test of Basic Skills Test National Percentile Rank for Vocabulary was 54.23 Soon after the injury, his schoolteacher, who had known him for 2 years, rated his preinjury behavior. She endorsed only 2 of more than 150 behavioral symptoms on the Pediatric Behavior Scale24 as occurring “often or pretty much” (i.e., “has a hard time making friends” and “quiet; doesn't talk very much”). No symptoms occurred “very often or very much.”Before the injury occurred, the nuclear family was a well-functioning unit as assessed by a semistructured standardized family interview25 conducted soon after the injury. There was no positive family psychiatric history for first-degree relatives, but there was a positive history of alcohol abuse in a second-degree relative. Within the first 2 years of follow-up, the mother of A10 developed an episode of major depressive disorder related to the stress she experienced attempting to manage him.The subject's LGCS was 3 and his duration of impaired consciousness (time from injury to consistently following simple commands) was 323 hours. Cumulative findings from a CT scan and MRI showed the following left-sided lesions: frontal operculum; anterior orbital frontal; posterior orbital frontal; subventricular area of orbital frontal lobe; prefrontal region; lenticular nucleus and caudate nucleus; anterior middle temporal gyrus; anterior inferior temporal gyrus; auditory region and areas anterior and posterior to the auditory region; and supramarginal gyrus.By the 3-month follow-up, the subject was diagnosed with the labile and disinhibited PC subtypes. His parents commented on his affective lability as follows: “He gets frustrated more easily”; “he thinks he is always right; when we try to convince him otherwise he goes off to the basement in a huff”; “he is laughing much more (than before injury)—he is so tickled.” His parents reported numerous examples of disinhibition, including his approaching them with a receipt during a church service, an inappropriate place for this type of transaction. He frequently kissed mother in public, and this was an uncomfortable change for the family. He publicly noted a blemish or scratch on his aunt's necklace. He was noted to be perseverative and subclinically more talkative: “He harps on the same topics e.g., talking about his brother's speed when driving.” He continued to the point where parents had to say “Stop!!”At the 6-month follow-up, he was diagnosed with the labile, aggressive, and disinhibited subtypes of PC and also met criteria for hypomania and ADHD with prominent symptoms of hyperactivity and inattention. Irritability was especially evident when limits were set. Usually his outbursts of anger were brief, but some were prolonged: “He was off the wall for 4 days when his broken musical instrument was not available for him to play.”He described his mood as “fantastic.” He felt he could fly and run faster than Carl Lewis. He evidenced a flight of ideas, discussed various plans for inventions, and spent considerable time imagining he had many possessions. Goal-directed activity was increased as he kept attempting to fix things. With difficulty, he was persuaded not to repair a gas line that was determined by the gas company to be too dangerous to fix. Disinhibition and markedly impaired judgment continued to be prominent: “He laughs too much at the dinner table. He puts inappropriate things in the microwave, e.g., metal; he ran his finger over the pilot light; he tried to reach a high point on the wall to get something—so he stepped into a drawer, which almost caused the dresser to topple over onto him. He bluntly asked girls whether they had a boyfriend (without any clue of appropriate flirting).”Eleven months postinjury he threatened suicide during an aggressive outburst. Carbamazepine was initiated, resulting in considerable improvement in his affective lability. At the 1-year follow-up, he continued to meet criteria for PC but not for mania or hypomania. He was explosive, aggressive, irritable, distractible, and had rapid speech. His parents characterized his irritability and aggression in the following ways: “He gets aggravated when instructed—he has a short fuse.” “Things out of routine upset him.” “He gets frustrated about others finding fault with him even though this was not intended.” “He will never acknowledge he is wrong.” “He pounds his head and the chairs when angry.” “He can go off at any point” for any reason. He continued to be disinhibited and impulsive and to follow through on impractical plans. Perseverative tendencies persisted (repeating catch-phrases like “what's going down”). “He is still bringing up the story of someone burping 6 months ago.” His parents reflected during rehabilitation and thereafter that he seemed to move up through the stages of childhood fairly rapidly as if he were reliving his life. He changed from being helpless, to relearning to walk and talk, then became very interested in playing with toys he had abandoned years before (e.g., playing with a sheriff's badge and holster at age 15).Thirteen months postinjury he was diagnosed with probable complex partial seizure disorder because of several possible staring spells, but the EEG was not epileptiform. In his second year postinjury, he continued to exhibit PC with labile, aggressive, and disinhibited subtypes. However, he developed mania toward the end of the year despite continued treatment with carbamazepine. He was often extremely irritable, explosive, and aggressive toward his parents and destructive to objects (e.g., frequently pinned his mother against the wall, locked her out of the house, attempted to attack his father with a knife and tried to strangle him). He smashed the dashboard of the car and punched a hole through the door. He poured grease all over the kitchen and pounded holes in the kitchen counter. He flung books off shelves and threw chairs in various outbursts. Yet after all this violence, this boy from a religious family yelled in anger, “I wish I could swear.”He started many projects and inventions; for instance, he destroyed a snow shovel when attempting to enhance its efficiency by adding various horizontal and vertical boards. His grandiosity was evident when he described the cure for AIDS in pages of written notes. Furthermore, he talked in public about how intelligent he was: “intelligent John Doe, John intelligent Doe, Doe intelligent John …”. Hyperactivity and distractibility were problematic. The combination of his rapid speech and flight of ideas led people to request that he repeat himself, which in turn led to angry retorts. His social judgment continued to be impaired. He told his speech therapist she needs a man or a husband to straighten her out because she is a female. His perseveration continued to be problematic. His parents stated that “he can't let go of a subject unless removed from the situation entirely.”Between 25 and 26 months postinjury, he required two hospitalizations for aggressive outbursts and school refusal. A trial of lithium, added to the previously ineffective carbamazepine and propranolol, was associated with improvement. He was transferred to a residential facility, where his mania resolved and all medications were discontinued. He was discharged after 2 months but required a prolonged readmission after about 2 months for continued school refusal. A subtler symptom noted by the family was that “he thinks things are funnier than they are but will miss puns.”His transition to young adulthood (ages 17 to 22; 33 to 93 months postinjury) was tumultuous even though there was no recurrence of mania or hypomania, nor any incidents of aggression toward others. The subject had psychiatric hospitalizations on five occasions for serious suicide attempts with overdoses of analgesics, sedatives, and even a household cleaner. These suicide attempts have always occurred in the midst of episodes of depression, which were invariably precipitated by disappointing news. The episodes were brief and lasted only 2 weeks. Periods of “remission” last about 2 months. He is managed on carbamazepine (reinstituted at 52 months postinjury, age 18) and on bupropion for his depression (sertraline and fluvoxamine were ineffective). carbamazepine is prescribed for psychiatric purposes since there is no evidence of seizures except for a few staring spells 1 year after injury. Furthermore, no seizures were evident even during the 2½-year period off carbamazepine.He has lived in several highly structured residential facilities. These settings, particularly those specialized for patients with brain injuries, were effective in keeping him safe. However, on several occasions he impulsively left without notice in poorly thought-out flights to “freedom.” On one occasion, 52 months postinjury, he withdrew $100 in savings and rode out of town on a bicycle. When his progress was limited by a tire puncture, he walked along a railway line to get further out of town. He then paid a trucker $100 to drive him another 30 miles to the next city. Out of money and plans, he called his parents to rescue him. Within weeks he was living unsupervised in an apartment. He began drinking alcohol excessively for the first time and was charged with public intoxication. Next, he stole a car while intoxicated and drove it wildly late at night in 2nd gear, leaving tracks on both sides of a highway. The car caught on fire and he continued to drive it “to put out the fire” until he was caught by police and forced to spend the night in jail. He was then committed by the court for alcohol treatment, his driver's license was revoked, and he was placed on probation.At age 22, the state of his life is very different from reasonable projections based on his preinjury status. He lives at home with his parents because he cannot function responsibly on his own, and he receives Social Security disability payments. His mother is his legal “representative payee” because of his financial irresponsibility (e.g., committing to buy a horse for $1,000 without funds to back up the purchase). He now receives an allowance of $10 per week and has reached a new equilibrium. He occupies himself on a nearby farm tending horses and refurbishing farm buildings with his father, all for no pay but with the opportunity to keep and ride his own and other horses. He does not see this as a real job because it is unpaid, and he intermittently becomes sad and irritable about his lot in life. He encourages himself, from lessons learned in various classes and psychotherapies, to believe that life is worth living. He dreams that someday he will have enough money to buy land for a horse farm. His family has thwarted further irresponsible attempts to buy another horse, and he still has years of payments to settle his current debts.He remains on probation for driving while intoxicated and does not have a driver's license. He is motivated not to use alcohol because of an alert probation officer who reinforces the fact that he faces 6 months in jail for any future alcohol offense. This has been more effective in dissuading his alcohol use than disulfiram. Despite compliance with disulfiram, he claims that he has consumed alcohol “half a dozen times” without ill effect.He has difficulties with organization and memory, and is easily distracted. These difficulties impair him in activities such as getting ready to leave the house and tending a busy meat counter in a supermarket. He finds it helpful to write himself reminder notes. He is irritated by noises when he attempts to concentrate, but he can read, play video games, and watch movies for hours.At present, he is more tactful and no longer makes inappropriate personal or sexual comments. Yet, in a major change from his premorbid style, he talks excessively in a nonpressured manner. He cares for others, nurtures his young nephews, and tries to comfort his parents if they express strong emotions. However, he finds it difficult to tolerate even normal emotions that family members express. Although he does not have antisocial personality disorder, he did steal two cars (once while intoxicated and once in a quest for “freedom”). He is not a daredevil and is overly afraid of car accidents. There has been no evidence of posttraumatic stress disorder, other anxiety disorders, eating disorders, tics, use of illicit substances, persistent apathy, or paranoia.
DISCUSSION
ACKNOWLEDGMENTS
References
Information & Authors
Information
Published In

History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
There are no citations for this item
View Options
View options
PDF/ePub
View PDF/ePubGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).